
Topical Wound Oxygen Therapy in the Treatment of Chronic Diabetic Foot Ulcers

Abstract
:1. Introduction
Oxygen and Wound Healing
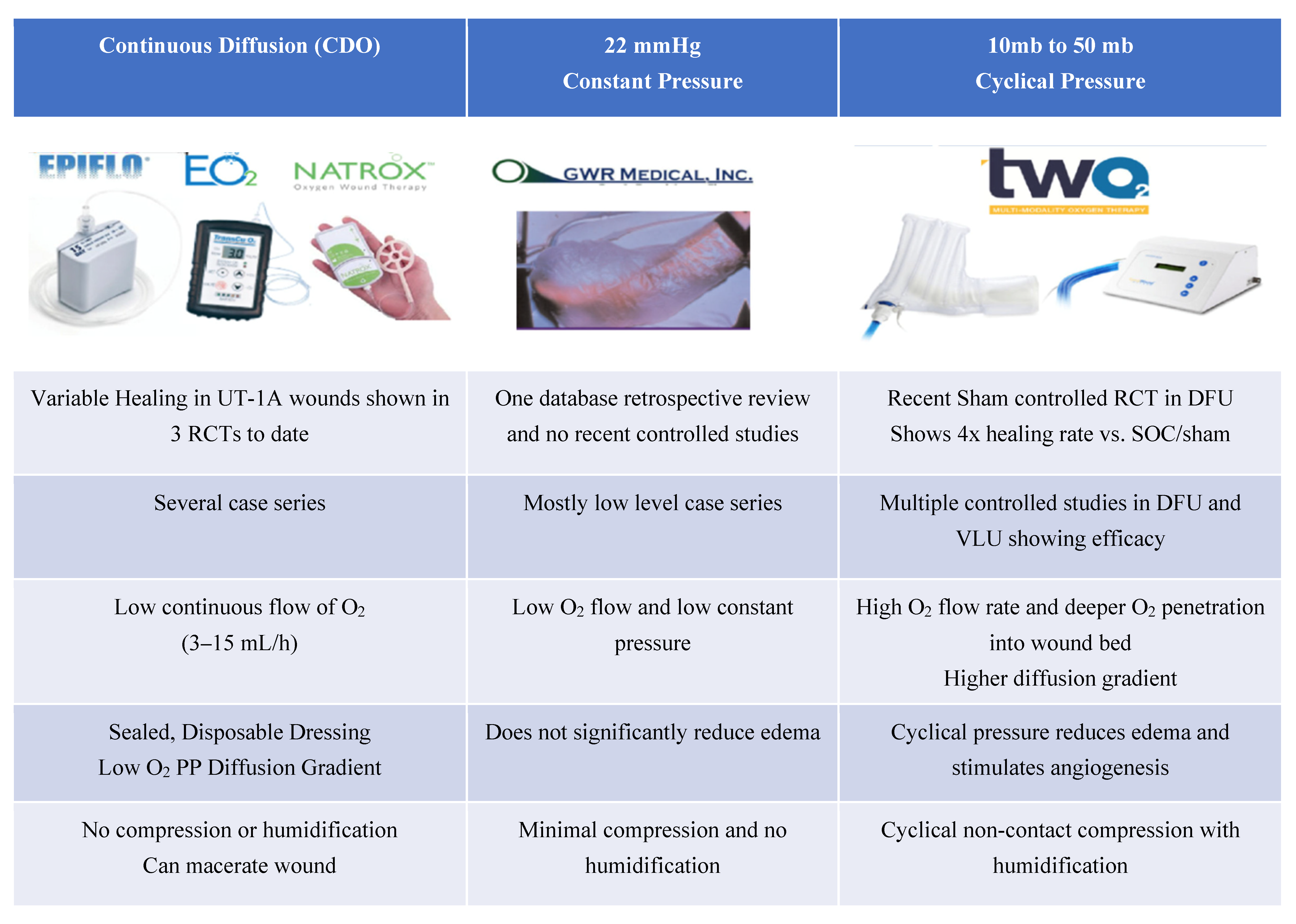
2. Topical Oxygen Devices
3. Topical Oxygen Effect on Wound Healing—The Evidence
4. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Fischer, B.H. Topical hyperbaric oxygen treatment of pressure sores and skin ulcers. Lancet 1969, 2, 405–409. [Google Scholar] [CrossRef]
- Leslie, C.A.; Sapico, F.L.; Ginunas, V.J.; Adkins, R.H. Randomized controlled trial of topical hyperbaric oxygen for treatment of diabetic foot ulcers. Diabetes Care 1988, 11, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Gottrup, F.; Dissemond, J.; Baines, C.; Frykberg, R.; Jensen, P.O.; Kot, J.; Kroger, K.; Longobardi, P. Use of Oxygen Therapies in Wound Healing. J. Wound Care 2017, 26, S1–S43. [Google Scholar] [CrossRef]
- Londahl, M.; Katzman, P.; Nilsson, A.; Hammarlund, C. Hyperbaric oxygen therapy facilitates healing of chronic foot ulcers in patients with diabetes. Diabetes Care 2010, 33, 998–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Margolis, D.J.; Gupta, J.; Hoffstad, O.; Papdopoulos, M.; Glick, H.A.; Thom, S.R.; Mitra, N. Lack of effectiveness of hyperbaric oxygen therapy for the treatment of diabetic foot ulcer and the prevention of amputation: A cohort study. Diabetes Care 2013, 36, 1961–1966. [Google Scholar] [CrossRef] [Green Version]
- Santema, K.T.B.; Stoekenbroek, R.M.; Koelemay, M.J.W.; Reekers, J.A.; van Dortmont, L.M.C.; Oomen, A.; Smeets, L.; Wever, J.J.; Legemate, D.A.; Ubbink, D.T.; et al. Hyperbaric Oxygen Therapy in the Treatment of Ischemic Lower- Extremity Ulcers in Patients With Diabetes: Results of the DAMO2CLES Multicenter Randomized Clinical Trial. Diabetes Care 2018, 41, 112–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Smet, G.H.J.; Kroese, L.F.; Menon, A.G.; Jeekel, J.; van Pelt, A.W.J.; Kleinrensink, G.J.; Lange, J.F. Oxygen therapies and their effects on wound healing. Wound Repair Regen. 2017, 25, 591–608. [Google Scholar] [CrossRef]
- Oropallo, A.R.; Serena, T.E.; Armstrong, D.G.; Niederauer, M.Q. Molecular Biomarkers of Oxygen therapy in Patients with Diabetic Foot Ulcers. Biomolecules 2021, 11, 925. [Google Scholar] [CrossRef]
- Dunnill, C.; Patton, T.; Brennan, J.; Barrett, J.; Dryden, M.; Cooke, J.; Leaper, D.; Georgopoulos, N.T. Reactive oxygen species (ROS) and wound healing: The functional role of ROS and emerging ROS-modulating technologies for augmentation of the healing process. Int. Wound J. 2017, 14, 89–96. [Google Scholar] [CrossRef]
- Sen, C.K. Wound healing essentials: Let there be oxygen. Wound Repair Regen. 2009, 17, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Gordillo, G.M.; Sen, C.K. Evidence-based recommendations for the use of topical oxygen therapy in the treatment of lower extremity wounds. Int. J. Low Extrem. Wounds 2009, 8, 105–111. [Google Scholar] [CrossRef]
- Wattel, F.; Mathieu, D. Oxygen and wound healing. Bull Acad. Natl. Med. 2005, 189, 853–864; discussion 864–855. [Google Scholar]
- Dissemond, J.; Kroger, K.; Storck, M.; Risse, A.; Engels, P. Topical oxygen wound therapies for chronic wounds: A review. J Wound Care 2015, 24, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Niederauer, M.Q. How can we deliver oxygen to wounds? J. Wound Care 2021, 30, S3–S4. [Google Scholar] [CrossRef] [PubMed]
- Serena, T.E.; Bullock, M.N.; Cole, W.; Lantis, J.; Li, L.; Moore, S.; Patel, K.; Sabo, M.; Wahab, N.; Price, P. Topical oxygen therapy in the treatment of diabetic foot ulcers: A multicentre, open, randomised controlled clinical trial. J. Wound Care 2021, 30, S1–S8. [Google Scholar] [CrossRef]
- Driver, V.R.; Reyzelman, A.; Kawalec, J.; French, M. A Prospective, Randomized, Blinded, Controlled Trial Comparing Transdermal Continuous Oxygen Delivery to Moist Wound Therapy for the Treatment of Diabetic Foot Ulcers. Ostomy Wound Manag. 2017, 63, 12–28. [Google Scholar]
- Driver, V.R.; Yao, M.; Kantarci, A.; Gu, G.; Park, N.; Hasturk, H. A prospective, randomized clinical study evaluating the effect of transdermal continuous oxygen therapy on biological processes and foot ulcer healing in persons with diabetes mellitus. Ostomy Wound Manag. 2013, 59, 19–26. [Google Scholar]
- Niederauer, M.Q.; Michalek, J.E.; Liu, Q.; Papas, K.K.; Lavery, L.A.; Armstrong, D.G. Continuous diffusion of oxygen improves diabetic foot ulcer healing when compared with a placebo control: A randomised, double-blind, multicentre study. J Wound Care 2018, 27, S30–S45. [Google Scholar] [CrossRef] [PubMed]
- Gordillo, G.M.; Roy, S.; Khanna, S.; Schlanger, R.; Khandelwal, S.; Phillips, G.; Sen, C.K. Topical oxygen therapy induces vascular endothelial growth factor expression and improves closure of clinically presented chronic wounds. Clin. Exp. Pharmacol. Physiol. 2008, 35, 957–964. [Google Scholar] [CrossRef] [Green Version]
- Fries, R.B.; Wallace, W.A.; Roy, S.; Kuppusamy, P.; Bergdall, V.; Gordillo, G.M.; Melvin, W.S.; Sen, C.K. Dermal excisional wound healing in pigs following treatment with topically applied pure oxygen. Mutat. Res. 2005, 579, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Kalliainen, L.K.; Gordillo, G.M.; Schlanger, R.; Sen, C.K. Topical oxygen as an adjunct to wound healing: A clinical case series. Pathophysiology 2003, 9, 81–87. [Google Scholar] [CrossRef]
- Copeland, K.; Purvis, A.R. A Retrospective Chart Review of Chronic Wound Patients Treated with Topical Oxygen Therapy. Adv. Wound Care (New Rochelle) 2017, 6, 143–152. [Google Scholar] [CrossRef]
- Ladizinsky, D.; Roe, D. New Insights Into Oxygen Therapy for Wound Healing. Wounds 2010, 22, 294–300. [Google Scholar] [PubMed]
- Tawfick, W.; Sultan, S. Does topical wound oxygen (TWO2) offer an improved outcome over conventional compression dressings (CCD) in the management of refractory venous ulcers (RVU)? A parallel observational comparative study. Eur. J. Vasc. Endovasc. Surg. 2009, 38, 125–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tawfick, W.A.; Sultan, S. Technical and clinical outcome of topical wound oxygen in comparison to conventional compression dressings in the management of refractory nonhealing venous ulcers. Vasc. Endovasc. Surg. 2013, 47, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Blackman, E.; Moore, C.; Hyatt, J.; Railton, R.; Frye, C. Topical wound oxygen therapy in the treatment of severe diabetic foot ulcers: A prospective controlled study. Ostomy Wound Manag. 2010, 56, 24–31. [Google Scholar]
- Frykberg, R.G.; Franks, P.J.; Edmonds, M.; Brantley, J.N.; Teot, L.; Wild, T.; Garoufalis, M.G.; Lee, A.M.; Thompson, J.A.; Reach, G.; et al. A Multinational, Multicenter, Randomized, Double-Blinded, Placebo-Controlled Trial to Evaluate the Efficacy of Cyclical Topical Wound Oxygen (TWO2) Therapy in the Treatment of Chronic Diabetic Foot Ulcers: The TWO2 Study. Diabetes Care 2020, 43, 616–624. [Google Scholar] [CrossRef] [Green Version]
- Gordillo, G.M.; Schlanger, R.; Wallace, W.A.; Bergdall, V.; Bartlett, R.; Sen, C.K. Protocols for topical and systemic oxygen treatments in wound healing. Methods Enzymol. 2004, 381, 575–585. [Google Scholar] [CrossRef]
- Gordillo, G.M.; Hunt, T.K.; Sen, C.K. Significance of oxygen therapeutics. Wound Repair Regen. 2003, 11, 393. [Google Scholar] [CrossRef]
- Gordillo, G.M.; Sen, C.K. Revisiting the essential role of oxygen in wound healing. Am. J. Surg. 2003, 186, 259–263. [Google Scholar] [CrossRef]
- Lavery, L.A.; Killeen, A.L.; Farrar, D.; Akgul, Y.; Crisologo, P.A.; Malone, M.; Davis, K.E. The effect of continuous diffusion of oxygen treatment on cytokines, perfusion, bacterial load, and healing in patients with diabetic foot ulcers. Int. Wound J. 2020, 17, 1986–1995. [Google Scholar] [CrossRef] [PubMed]
- Yellin, J.I.; Gaebler, J.A.; Zhou, F.F.; Niecko, T.; Novins, O.; Ockert, A.; Krzynowek, D.; Garoufalis, M.G.; Lee, A.M.; Frykberg, R.G. Reduced Hospitalizations and Amputations in Patients with Diabetic Foot Ulcers Treated with Cyclical Pressurized Topical Wound Oxygen Therapy: Real World Outcomes. 2021; submit. [Google Scholar]
- Nataraj, M.; Maiya, A.G.; Karkada, G.; Hande, M.; Rodrigues, G.S.; Shenoy, R.; Prasad, S.S. Application of Topical Oxygen Therapy in Healing Dynamics of Diabetic Foot Ulcers—A Systematic Review. Rev. Diabet. Stud. 2019, 15, 74–82. [Google Scholar] [CrossRef] [Green Version]
- Thanigaimani, S.; Singh, T.; Golledge, J. Topical oxygen therapy for diabetes-related foot ulcers: A systematic review and meta-analysis. Diabet. Med. 2021, e14585. [Google Scholar] [CrossRef]


{kind=link}
| Oxygen-Dependent Product | Enzyme or Substrate | Function | Cytokine, Cell Mediators; or Cellular/Tissue Effect |
|---|---|---|---|
| ATP | ATP synthase, Cytochrome C, Electronic Transport Chain | Chemical Energy for metabolism | |
| Reactive Oxygen Species (ROS) “respiratory burst” (Superoxide, Hydrogen peroxide (H2O2)) | NADPH oxidase | Cellular Signaling/transduction Bacterial defenses Angiogenesis | Cell division and migration. Upregulation of Growth Factors (VEGF, PDGF, etc.) (leukocyte migration and phagocytosis, bacteriostatic H2O2) VEGF, PDGF, NO, etc. |
| Collagen synthesis | Prolyl hydroxylase, lysyl hydroxylase | Collagen deposition and crosslinking | Fibroblasts |
| Nitric oxide (NO) | Nitric oxide synthase | Vasodilatation, angiogenesis | Endothelium |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frykberg, R.G. Topical Wound Oxygen Therapy in the Treatment of Chronic Diabetic Foot Ulcers. Medicina 2021, 57, 917. https://doi.org/10.3390/medicina57090917
Frykberg RG. Topical Wound Oxygen Therapy in the Treatment of Chronic Diabetic Foot Ulcers. Medicina. 2021; 57(9):917. https://doi.org/10.3390/medicina57090917
Chicago/Turabian StyleFrykberg, Robert G. 2021. "Topical Wound Oxygen Therapy in the Treatment of Chronic Diabetic Foot Ulcers" Medicina 57, no. 9: 917. https://doi.org/10.3390/medicina57090917
APA StyleFrykberg, R. G. (2021). Topical Wound Oxygen Therapy in the Treatment of Chronic Diabetic Foot Ulcers. Medicina, 57(9), 917. https://doi.org/10.3390/medicina57090917