
Activity of Total Alcohol Dehydrogenase, Alcohol Dehydrogenase Isoenzymes and Aldehyde Dehydrogenase in the Serum of Patients with Alcoholic Fatty Liver Disease

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Blood Collection
2.3. Determination of Total ADH Activity
2.4. Determination of ADH I and ADH II Isoenzyme Activity
2.5. Determination of ADH III Isoenzyme Activity
2.6. Determination of ADH IV Isoenzyme Activity
2.7. Determination of Total ALDH Activity
2.8. Statistical Calculations
3. Results
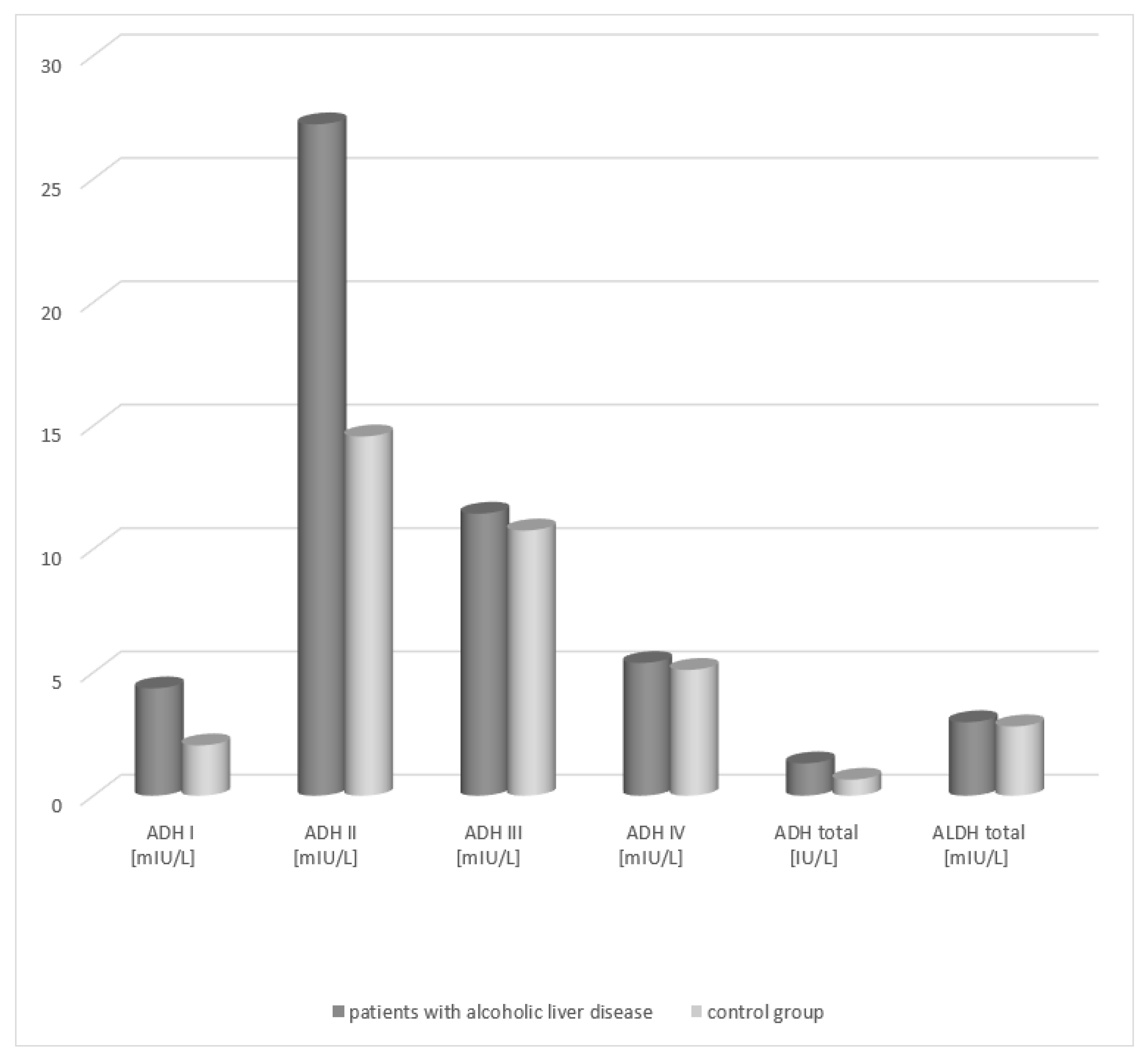
3.1. Assessment of ADH and Its Isoenzymes and ALDH Activity in the Serum of Patients with Alcoholic Fatty Liver and in the Control Group
3.2. Comparison of the Activity of ADH and Its Isoenzymes and ALDH Depending on the Degree of Hepatic Tissue Cirrhosis
3.3. ROC Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mikołajczyk, I.; Rosołowski, M.; Łukaszyk, M. Choroba stłuszczeniowa wątroby. Przegl. Gastroenterol. 2008, 3, 276–282. [Google Scholar]
- O’Shea, R.S.; Dasarathy, S.; McCullough, A.J. Practice Guideline Committee of the American Association for the Study of Liver Diseases. Alcoholic liver disease. Hepatology 2010, 51, 307–328. [Google Scholar]
- Kamper-Jorgensen, M.; Gronbaek, M.; Tolstrup, J. Alcohol and cirrhosis: Dose-response or threshold effect. J. Hepatol. 2004, 41, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Beier, J.I.; McClain, C.J. Mechanisms and cell signaling in alcoholic liver disease. Biol. Chem. 2010, 391, 1249–1264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jelski, W.; Strumnik, A.; Orywal, K.; Lapinski, T.W.; Swiderska, M.; Szmitkowski, M. Activity of alcohol dehydrogenase isoenzymes and aldehyde dehydrogenase in sera of patients with hepatitis C. Arch. Med. Sci. 2018, 14, 281–287. [Google Scholar] [CrossRef] [Green Version]
- Jelski, W.; Zalewski, B.; Szmitkowski, M. Alcohol dehydrogenase (ADH) isoenzymes and aldehyde dehydrogenase (ALDH) in the sera of patients with liver cancer. J. Clin. Lab. Anal. 2008, 22, 204–209. [Google Scholar] [CrossRef]
- Jelski, W.; Wolszczak-Biedrzycka, B.; Zasimowicz-Majewska, E.; Orywal, K.; Piechota, J.; Lapinski, T.W.; Bednarczyk, M.; Szmitkowski, M. The Activity of Alcohol Dehydrogenase Isoenzymes and Aldehyde Dehydrogenase in the Sera of Patients with Autoimmune Hepatitis. Clin. Lab. 2018, 64, 477–481. [Google Scholar] [CrossRef]
- Jelski, W.; Wolszczak-Biedrzycka, B.; Zasimowicz-Majewska, E.; Orywal, K.; Lapinski, T.W.; Szmitkowski, M. Alcohol Dehydrogenase Isoenzymes and Aldehyde Dehydrogenase Activity in the Serum of Patients with Non-alcoholic Fatty Liver Disease. Anticancer. Res. 2018, 38, 4005–4009. [Google Scholar] [CrossRef]
- Gaggini, M.; Navarro, R.; Stefanini, A. Correlation between METAVIR scores and Raman spectroscopy in liver lesions induced by hepatitis C virus: A preliminary study. Lases. Med. Sci. 2015, 5, 1347–1355. [Google Scholar] [CrossRef] [PubMed]
- Skursky, L.; Kovar, J.; Stachova, M. A sensitive photometric assay for alcohol dehydrogenase activity in blood serum. Anal. Biochem. 1999, 99, 65–71. [Google Scholar] [CrossRef]
- Jelski, W.; Chrostek, L.; Szmitkowski, M. The activity of class I, II, III and IV of alcohol dehydrogenase (ADH) isoenzymes and aldehyde dehydrogenase (ALDH) in the breast cancer. Clin. Exp. Med. 2006, 6, 89–93. [Google Scholar] [CrossRef]
- Jelski, W.; Orywal, K.; Panek, B. The activity of class I, II, III and IV of alcohol dehydrogenase (ADH) isoenzymes and aldehyde dehydrogenase (ALDH) in the wall of abdominal aortic aneurysms. Exp. Mol. Path. 2009, 87, 59–62. [Google Scholar] [CrossRef]
- Jelski, W.; Kozłowski, M.; Laudański, J. The activity of class I, II, III and IV alcohol dehydrogenase (ADH) isoenzymes and aldehyde dehydrogenase (ALDH) in esophageal cancer. Dig. Dis. Sci. 2009, 54, 725–730. [Google Scholar] [CrossRef]
- Orywal, K.; Jelski, W.; Zdrodowski, M. The activity of class I, II, III and IV alcohol dehydrogenase isoenzymes and aldehyde dehydrogenase in cervical cancer. Clin. Bioch. 2011, 44, 1231–1234. [Google Scholar] [CrossRef] [PubMed]
- Jelski, W.; Srumnik, A.; Orywal, K. The activity of alcohol dehydrogenase (ADH) in the serum of patients with hepatitis C. Archiv. Med. Sci. 2018, 14, 281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chrostek, L.; Szmitkowski, M. Isoenzymes of class I and II alcohol dehydrogenase in chronic hepatitis. Clin. Chem. Lab. Med. 1999, 37, 145–147. [Google Scholar] [CrossRef]
- Chrostek, L.; Cylwik, B.; Szmitkowski, M. Interakcja pomiędzy metabolizmem etanolu i serotoniny. Twój Mag. 2004, 7, 10–15. [Google Scholar]
- Jelski, W.; Zalewski, B.; Szmitkowski, M. The activity of class I, II, III and IV of alcohol dehydrogenase (ADH) isoenzymes and aldehyde dehydrogenase (ALDH) in liver cancer. Dig. Dis. Sci. 2008, 53, 2550–2555. [Google Scholar] [CrossRef]
- Jelski, W.; Mroczko, B. Biochemical diagnostics of pancreatic cancer—Present and future. Clin. Chim. Acta. 2019, 498, 47–51. [Google Scholar] [CrossRef]
- Guo, E.; Wei, H.; Liao, X. Prognostic value of alcohol dehydrogenase mRNA expression in gastric cancer. Oncol. Lett. 2018, 15, 5505–5516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enomoto, N.; Takase, S.; Takada, N. Alcoholic liver disease in heterozygotes of mutant and normal aldehyde dehydrogenase-2 genes. Hepatology 1991, 13, 1071–1075. [Google Scholar] [CrossRef]
- Wei, R.R.; Zhang, M.Y.; Rao, H.L. Identification of ADH4 as a novel and potential prognostic marker in hepatocellular car-cinoma. Med. Oncol. 2012, 29, 2737–2743. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J. The diagnosis and management of non-alcoholic fatty liver disease: Practice guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012, 55, 2005–2023. [Google Scholar] [CrossRef] [PubMed]
- Hubacek, J.A.; Pelclova, D.; Seidl, Z. Rare alleles within the CYP2E1 (MEOS system) could be associated with better short-term health outcome after acute methanol poisoning. Clin. Pharmacol. Toxicol. 2015, 116, 168–172. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| STUDY GROUPS | ADH I | ADH II | ADH III | ADH IV | ADH Total | ALDH Total |
|---|---|---|---|---|---|---|
| Median | Median | Median | Median | Median | Median | |
| Range | Range | Range | Range | Range | Range | |
| Mean | Mean | Mean | Mean | Mean | Mean | |
| Patients with alcoholic fatty liver (n = 38) | 4.45 | 29.21 | 12.43 | 5.18 | 1.41 | 3.08 |
| 1.25–6.84 | 11.42–48.76 | 6.85–20.11 | 2.54–11.66 | 0.33–2.82 | 1.36–6.58 | |
| 4.17 | 26.54 | 11.03 | 5.2 | 1.14 | 2.84 | |
| Control group (n = 40) | 2.14 | 15.56 | 11.75 | 5.02 | 0.63 | 2.8 |
| 0.86–5.36 | 5.84–22.30 | 6.86–19.14 | 2.20–10.92 | 0.23–1.99 | 1.22–6.21 | |
| 1.85 | 13.44 | 10.42 | 4.98 | 0.52 | 2.68 | |
| p < 0.01 | p < 0.01 | p = 0.362 | p = 0.514 | p < 0.001 | p = 0.551 |
| STUDY GROUPS | ADH I | ADH II | ADH III | ADH IV | ADH Total | ALDH Total |
|---|---|---|---|---|---|---|
| Median | Median | Median | Median | Median | Median | |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |
| 1st degree | 3.85 | 26.32 | 11.08 | 5.01 | 1.2 | 2.72 |
| (n = 12) | 3.77 ± 2.32 | 26.07 ± 23.26 | 11.06 ± 9.45 | 4.89 ± 4.26 | 1.08 ± 0.99 | 2.62 ± 3.21 |
| 2nd degree | 4.08 | 26.94 | 11.21 | 5.15 | 1.29 | 2.84 |
| (n = 8) | 3.95 ± 2.61 | 26.48 ± 24.75 | 11.16 ± 9.22 | 5.02 ± 4.64 | 1.11 ± 1.03 | 2.78 ± 3.64 |
| 3rd degree | 4.21 | 27.32 | 11.36 | 5.42 | 1.4 | 3.01 |
| (n = 13) | 4.07 ± 2.56 | 26.85 ± 24.01 | 11.34 ± 9.02 | 5.34 ± 4.35 | 1.26 ± 1.01 | 2.95 ± 3.12 |
| 4th degree | 4.44 | 27.38 | 11.62 | 5.45 | 1.39 | 3.09 |
| (n = 5) | 4.33 ± 2.14 | 27.46 ± 24.53 | 11.48 ± 9.90 | 5.30 ± 4.77 | 1.20 ± 1.05 | 3.04 ± 3.54 |
| Control group | 2.14 | 14.56 | 10.75 | 5.1 | 0.65 | 2.7 |
| (n = 40) | 1.85 ± 1.66 | 13.44 ± 8.66 | 10.42 ± 8.34 | 4.98 ± 4.82 | 0.52 ± 1.25 | 2.58 ± 3.41 |
| pa < 0.01 | pa < 0.01 | pa = 0.464 | pa = 0.416 | pa < 0.01 | pa = 0.532 | |
| pb < 0.01 | pb < 0.01 | pb = 0.421 | pb = 0.347 | pb < 0.01 | pb = 0.495 | |
| pc < 0.01 | pc < 0.01 | pc = 0.376 | pc = 0.404 | pc < 0.01 | pc = 0.566 | |
| pd < 0.01 | pd < 0.01 | pd = 0.301 | pd = 0.337 | pd < 0.01 | pd = 0.548 |
| Parameter | AUC | p-Value | Cut-Off Value | Sensitivity (%) | Specificity (%) | 95% Confidence Interval |
|---|---|---|---|---|---|---|
| ADH I | 0.784 | <0.01 | 5.05 | 74.56 | 78.35 | 1.25–6.84 |
| ADH II | 0.758 | <0.01 | 36.81 | 70.15 | 75.72 | 11.42–48.76 |
| ADH total | 0.706 | <0.001 | 2.45 | 66.42 | 70.33 | 0.33–2.82 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolszczak-Biedrzycka, B.; Zasimowicz-Majewska, E.; Bieńkowska, A.; Biedrzycki, G.; Dorf, J.; Jelski, W. Activity of Total Alcohol Dehydrogenase, Alcohol Dehydrogenase Isoenzymes and Aldehyde Dehydrogenase in the Serum of Patients with Alcoholic Fatty Liver Disease. Medicina 2022, 58, 25. https://doi.org/10.3390/medicina58010025
Wolszczak-Biedrzycka B, Zasimowicz-Majewska E, Bieńkowska A, Biedrzycki G, Dorf J, Jelski W. Activity of Total Alcohol Dehydrogenase, Alcohol Dehydrogenase Isoenzymes and Aldehyde Dehydrogenase in the Serum of Patients with Alcoholic Fatty Liver Disease. Medicina. 2022; 58(1):25. https://doi.org/10.3390/medicina58010025
Chicago/Turabian StyleWolszczak-Biedrzycka, Blanka, Elżbieta Zasimowicz-Majewska, Anna Bieńkowska, Grzegorz Biedrzycki, Justyna Dorf, and Wojciech Jelski. 2022. "Activity of Total Alcohol Dehydrogenase, Alcohol Dehydrogenase Isoenzymes and Aldehyde Dehydrogenase in the Serum of Patients with Alcoholic Fatty Liver Disease" Medicina 58, no. 1: 25. https://doi.org/10.3390/medicina58010025