Abstract
Background and Objectives: In 2020, the World Health Organization (WHO) reported 9.9 million deaths from cancer, with a mortality rate of 10.65%. Early detection of cancer can decrease mortality and increase the chance of cure. In Saudi Arabia, multiple studies were performed for awareness and attitudes toward cancer, but few studies evaluated the awareness of familial and inherited cancers. Materials and Methods: This is a cross-sectional observational survey of the awareness, knowledge, and attitudes of Saudi women toward familial and inherited cancers. The estimated sample size was 385. Questionnaires were distributed through social media platforms from 1 January 2021 to 22 January 2021. Results: Of the 385 participants, the majority have a bachelor’s degree. More than half (68.9%) know that family history is related to cancer, and approximately 57.2% are aware of genetic testing. The most common indication of genetic testing is premarital testing (18.5%). An inverse relationship is noted between the awareness of familial and inherited cancers and age (p = 0.003, CI = 0.723–0.938). However, awareness of inherited and familial cancer is positively associated with awareness of the association of genetic mutation to cancer (p = 0.013, CI = 1.080–1.921) and knowledge about genetic testing (p > 0.000, CI = 2.487–8.426). Conclusions: Our results reveal that Saudi women, especially older adults, have suboptimal knowledge about inherited and familial cancers, and poor attitudes toward genetic screening. We recommend increasing public awareness regarding risk factors and screening for inherited and familial cancers.
1. Introduction
Cancer is a common cause of morbidity and mortality. In 2020, breast, lung, colorectal, prostate, stomach, and liver cancers were the most common cancers worldwide [1]. The World Health Organization (WHO) reports 19.29 million new cancer cases every year [1]. Malignancy is the second most common cause of death, accounting for approximately 20% of all deaths in 2017 [2]. In 2020, the WHO reported 9.9 million cancer deaths (mortality rate: 10.65%) [1]. Cancer also has a substantial economic burden; it was estimated that the national cancer care in 2020 will cost USD 157.77 billion [3].
In Saudi Arabia, the number of newly diagnosed cancer cases in 2020 was 27,885 (14,253 were males and 13,632 were females). The most common cancers in males were colorectal cancer, non-Hodgkin lymphoma, leukemia, and thyroid and lung cancers. In females, the most common types of cancer were breast, thyroid, colorectal, and uterine cancers, and leukemia. The number of deaths due to cancer was 13,069 (mortality rate: 5.41%) [4].
Given the huge impact of malignancy, early cancer detection and treatment initiation can decrease mortality and increase the chance of cure [5]. The most common method to detect cancer early is screening, such as a mammogram for breast cancer, colonoscopy for colorectal cancer, or Pap smear for cervical cancer [6,7,8]. Familial and inherited cancer can present at an early age; thus, screening for these cancers should be performed earlier than in the general population [9]. Early screening decreases cancer mortality and morbidity [10].
Many studies addressed the Saudi populations’ awareness and attitude toward cancer. Awareness of breast cancer among Saudi women was found to be poor [11,12]. Misinformation about mammographic screening was found to significantly reduce its use by 56% (OR = 0.44; 95% CI = 0.22–0.88) [12]. In addition, Saudis had poor-to-moderate awareness of cervical cancer [13,14]. While a study in Qassim shows negative attitudes toward Pap screening and human papillomavirus (HPV) vaccination [13], another study shows a preference for adding HPV testing to premarital screening [14]. A survey about colorectal cancer awareness in Riyadh reveals some misconceptions regarding universally accepted screening protocols, symptoms, and a general understanding of colorectal cancer in Saudi Arabia [15].
There are many etiologies of cancer; one of them is inherited/familial, such as Lynch syndrome [16] and BRCA1 and 2 gene mutations [17]. About 30% of patients with colorectal cancer have a family history of colorectal cancer [18], and a positive family history is associated with a worse prognosis in patients with head and neck cancer than in those without a family history [19].
Despite the availability and tangibility of information in the Internet era, worldwide communities had poor–moderate knowledge about inheritance features and factors of breast cancer [20,21] and prostate cancer [22]. It was found that awareness of inherited prostatic cancer was associated with elder age and having a family member with cancer. However, no association was found in education level [22]. Meanwhile, there was a significant association between age and level of education in the knowledge of inherited breast cancer in Saudi women [23]. A systematic review shows that ethnic minorities have lower knowledge of inherited cancer and genetic testing [24]. Roberts et al. show that awareness of genetic testing is significantly associated with non-Hispanic, middle age, and higher education levels [25] This study assessed the awareness and attitude of Saudis toward familial and inherited cancer, as well as the associated factors.
2. Materials and Methods
This was a cross-sectional observational survey of the awareness, knowledge, and perception of Saudi women toward familial and inherited cancers. On the basis of the Saudi female census of 2018, which included 10,192,732 females, the sample size was estimated. With a confidence level of 95% and a confidence interval of 5%, the approximate sample size was 385.
There were two major sections of close-ended elements in the questionnaire. The first section included sociodemographic data, and the second evaluated the respondents’ awareness of familial and inherited cancer, adapted from a study in Jordan [26,27]. A pilot with 50 participants was conducted to modify the survey according to the study objectives and review for consistency. The electronic questionnaire was shared on social media platforms to recruit participants through convenient sampling. The inclusion criteria involved Saudi women > 17 years old. Data collection started on 1 January 2021, and was concluded at the completion of the sample size on 22 January 2021.
Data were then exported for analysis using SPSS for Windows, version 21.0 (SPSS Inc., Chicago, IL, USA). Categorical variables are expressed as percentages. The odds ratio was used to study association between different variables. Univariate and multivariate logistic regression were used to assess the predictive factors of the awareness of familial and inherited cancer among Saudis, with p < 0.05 considered significant.
The study was approved by the King Saud University Institutional Review Board (E-20-5397). The participants completed the online surveys anonymously and voluntarily. Furthermore, each participant had a unique IP address to prevent duplication, and the participants were not offered rewards or incentives for their participation.
3. Results
A total of 385 participants completed the questionnaire. Most participants are 18–24 years (35%), have a bachelor’s degree (65%), are single (55.9%), are unemployed (77.2%), and have no health insurance (68.4%). Only 3.5% of them are smokers, and 32.7% have children (Table 1).

Table 1.
Sociodemographic data.
Table 2 describes the awareness of these participants toward familial and inherited cancer, manifested by awareness of the association of cancer with consanguinity (21.8%), family history (68.9%), and genetic mutations (57.5%), along with the association of consanguinity with congenital malformations (79.2%). More than half of these participants know about genetic testing (57.2%), but only a quarter (25.32%) have undergone some sort of genetic testing. The most common indication of genetic testing is premarital testing (18.5%), as requested by the court (15.7%). Most of those who partake in the test (11.4%) are neither briefed about or consented to it before performing the test, but are generally satisfied (16.8%) with the level of privacy offered. Furthermore, 57% are willing to be screened for cancer through genetic testing, but only 21.8% know about the role of the genetic counselor.
Table 2.
Awareness, perceptions, and attitudes towards familial and inherited cancer (n = 395).
There is a huge variation in the awareness of the participants toward familial and inherited cancer in different cities in Saudi Arabia (Figure 1).
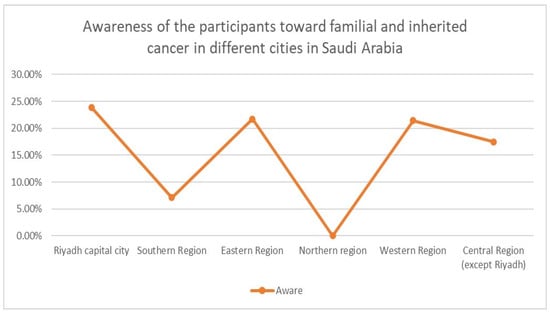
Figure 1.
Awareness of the participants toward familial and inherited cancer in different regions in Saudi Arabia. X axis: main regions in Saudi Arabia. Y axis: percentage of the awareness toward familial and inherited cancer.
Awareness of familial and inherited cancer is associated with only a few factors, including younger age (OR = 0.863, p = 0.017, CI = 0.765–0.973), awareness of the association of genetic mutation with cancer (OR = 1.542, p = 0. 002, CI = 1.169–2.034), and the knowledge about genetic testing (OR = 4.291, p = 0. 000, CI = 2.385–7.718) (Table 3). However, some of the factors have a wide CI, which can indicate less precision of our sample. In multivariate analysis, younger age (OR = 0.823, p = 0.003, CI = 0.723–0.938), awareness about the association of genetic mutation with cancer (OR=1. 441, p = 0.013, CI = 1.080–1.921), and knowledge about genetic testing (OR = 4. 578, p > 0.000, CI = 2.487–8.426) are found to be significant for awareness of familial and inherited cancer (Table 4).
Table 3.
Univariate analysis for the assessment of the factors influencing awareness of family and inherited cancer.
Table 4.
Multivariate analysis of significant variables influencing awareness of family and inherited cancer (p < 0.05).
4. Discussion
This study addressed the awareness and attitude of Saudi women toward inherited cancer and assessed the associated factors. Although most participants are educated (with a bachelor’s degree), most have suboptimal knowledge about inherited and familial cancers. Moreover, an inverse relationship is observed between awareness of familial and inherited cancers and age; older participants are significantly less aware (OR = 0. 823, p = 0.003, CI = 0.723–0.938).
Saudi Arabia has a high rate of consanguinity (56%), with some regional variations, and the highest prevalence being in rural areas [28]. Consanguineous marriage is proven to be associated with congenital anomalies [29,30] as well as specific cancers, such as leukemia, lymphoma, colorectal, and prostate cancers [31]. In this study, 53.4% of the study participants thought that cancer has no association with consanguinity, but they are more aware of the association of consanguinity with congenital anomalies (79.2%). This highlights the importance of educating the population about the risks of consanguinity and its effect on inherited diseases.
Most participants are aware of the association of family history (68.9%) and genetic mutations (57.5%) with cancer. Although more than half of the respondents (57.2%) know that there are genetic tests to detect familial and inherited cancers, the majority (74.2%) have never undergone genetic testing. Costs and lack of insurance are reported as major factors that discourage genetic testing [32,33,34]. Most of our participants are unemployed (77.2%), and have no health insurance (68.4%).
Of the 105 participants who underwent genetic testing, 59% participated for premarital testing (which was under the Healthy Marriage Program), and only 7.6% through a family physician. The low tendency of participants toward genetic testing could be linked to the fact that most participants (68.4%) do not have insurance to cover it. Furthermore, only 21.8% understand the role of the genetic counselor. The Healthy Marriage Program is a national premarital screening program for some of the highly prevalent inherited diseases in Saudi Arabia, such as sickle cell disease and thalassemia [35]. Only 73 participants (18.5%) have undergone premarital testing. However, this might be because the program was initiated and mandated in 2004.
Family physicians and general practitioners play a vital role in referring at-risk patients to genetic counselors or clinical geneticists. However, one study shows that general practitioners have limited knowledge about hereditary cancers, testing services, and genetic counseling [36], which may delay the referral of high-risk patients and their families to specialized care [36].
The attitudes of our participants toward genetic screening are not reassuring: 43% are unwilling to undergo cancer screening through genetic testing. Further efforts are required to ensure the proper counseling, consenting, and privacy of those undergoing genetic testing.
This study has a few limitations. The study design is a cross-sectional study, which may be prone to incidence–prevalence bias. The sample size only includes women, who happen to be mostly bachelor’s degree graduates. Therefore, the results of this study cannot be generalized to the general Saudi population. Also, there is an inflation of the CI due to the use of 95% CI, therefore, the problem of the monotonic likelihood of the univariate model may be noted in this study [37]. We recommend future cohort studies addressing this topic to include a more representative sample with a larger sample size.
5. Conclusions
In conclusion, our findings indicate suboptimal knowledge among Saudi women, particularly older women, about inherited and familial cancers, and poor attitudes toward genetic screening. We recommend increasing public awareness regarding risk factors and screening for inherited and familial cancers.
Author Contributions
Conceptualization, K.M.A.; methodology, L.A. and N.I.A.; software, L.A. and L.Y.A.; validation, N.I.A.; formal analysis, L.A. and L.Y.A.; investigation, A.S.A., N.I.A. and L.A.; resources, A.S.A.; data curation, L.A.; writing—original draft preparation, A.S.A., L.A. and L.Y.A.; writing—review and editing, A.S.A., L.A. and K.M.A.; supervision, K.M.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of King Saud University Institutional Review Board (E-20-5397 on 30 December 2020).
Informed Consent Statement
The participants completed the online surveys anonymously and voluntarily. Furthermore, each participant had a unique IP address to prevent duplication, and the participants were not offered rewards or incentives for their participation.
Data Availability Statement
The data used to support the findings of the study can be available at request to the corresponding author.
Acknowledgments
We thank Raed Alenezi, Aisha Alharbi, Aseel Tammar, Khalid Alshehri, Mohammed Alqahtani, Anwar Alanazi, and Khalid Alzhrani for their contributions to data collection.
Conflicts of Interest
The authors declare that there are no conflicts of interest regarding the publication of this paper.
References
- All Cancers. 2020. Available online: https://gco.iarc.fr/today (accessed on 28 September 2022).
- Heron, M. National Vital Statistics Reports Volume 68, Number 6, June 24, 2019, Deaths: Leading Causes for 2017. 2019. Available online: https://www.cdc.gov/nchs/products/index.htm (accessed on 28 September 2022).
- Mariotto, A.B.; Yabroff, K.R.; Shao, Y.; Feuer, E.J.; Brown, M.L. Projections of the Cost of Cancer Care in the United States: 2010–2020. J. Natl. Cancer Inst. 2011, 103, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.A.; Oeffinger, K.C. The Importance of Cancer Screening. Med Clin. N. Am. 2020, 104, 919–938. [Google Scholar] [CrossRef] [PubMed]
- Monticciolo, D.L. Current Guidelines and Gaps in Breast Cancer Screening. J. Am. Coll. Radiol. 2020, 17, 1269–1275. [Google Scholar] [CrossRef]
- Montminy, E.M.; Jang, A.; Conner, M.; Karlitz, J.J. Screening for Colorectal Cancer. Med. Clin. N. Am. 2020, 104, 1023–1036. [Google Scholar] [CrossRef]
- Fontham, E.T.H.; Wolf, A.M.D.; Church, T.R.; Etzioni, R.; Flowers, C.R.; Herzig, A.; Guerra, C.E.; Oeffinger, K.C.; Shih, Y.T.; Walter, L.C.; et al. Cervical cancer screening for individuals at average risk: 2020 guideline update from the American Cancer Society. CA Cancer J. Clin. 2020, 70, 321–346. [Google Scholar] [CrossRef]
- van den Broek, J.J.; Schechter, C.B.; van Ravesteyn, N.T.; Janssens, A.C.J.W.; Wolfson, M.C.; Trentham-Dietz, A.; Simard, J.; Easton, D.F.; Mandelblatt, J.S.; Kraft, P.; et al. Personalizing Breast Cancer Screening Based on Polygenic Risk and Family History. J. Nat. Cancer Inst. 2021, 113, 434–442. [Google Scholar] [CrossRef]
- Levin, B.; Lieberman, D.A.; McFarland, B.; Andrews, K.S.; Brooks, D.; Bond, J.; Dash, C.; Giardiello, F.M.; Glick, S.; Johnson, D.; et al. Screening and Surveillance for the Early Detection of Colorectal Cancer and Adenomatous Polyps, 2008: A Joint Guideline From the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. Gastroenterology 2008, 134, 1570–1595. [Google Scholar] [CrossRef]
- Alshareef, B.; Yaseen, W.; Jawa, W.; Barnawe, Y.; AlShehri, W.; Alqethami, H.; Bukari, W.; Alqumaili, O. Breast Cancer Awareness among Female School Teachers in Saudi Arabia: A Population Based Survey. Asian Pac. J. Cancer Prev. 2020, 21, 337–342. [Google Scholar] [CrossRef]
- Al-Zalabani, A.H.; Alharbi, K.D.; Fallatah, N.I.; Alqabshawi, R.I.; Al-Zalabani, A.A.; Alghamdi, S.M. Breast Cancer Knowledge and Screening Practice and Barriers Among Women in Madinah, Saudi Arabia. J. Cancer Educ. 2018, 33, 201–207. [Google Scholar] [CrossRef]
- Alnafisah, R.A.; Alsuhaibani, R.A.; Alharbi, M.A.; Alsohaibani, A.A.; Ismai, A.A. Saudi women’s knowledge and attitude toward cervical cancer screening, treatment, and prevention: A cross-sectional study in Qassim Region (2018–2019). Asian Pac. J. Cancer Prev. 2019, 20, 2965–2969. [Google Scholar] [CrossRef] [PubMed]
- Almehmadi, M.M.; Salih, M.M.; Al-Hazmi, A.S. Awareness of human papillomavirus infection complications, cervical cancer, and vaccine among the saudi population: A cross-sectional survey. Saudi Med. J. 2019, 40, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Zubaidi, A.M.; Alsubaie, N.M.; Alhumaid, A.A.; Shaik, S.A.; Alkhayal, K.A.; Alobeed, O.A. Public awareness of colorectal cancer in Saudi Arabia: A survey of 1070 participants in Riyadh. Saudi J. Gastroenterol. 2015, 21, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Stoffel, E.M.; Kastrinos, F. Familial colorectal cancer, beyond lynch syndrome. Clin. Gastroenterol. Hepatol. 2014, 12, 1059–1068. [Google Scholar] [CrossRef] [PubMed]
- Wendt, C.; Margolin, S. Identifying breast cancer susceptibility genes—A review of the genetic background in familial breast cancer. Acta Oncol. 2019, 58, 135–146. [Google Scholar] [CrossRef]
- Henrikson, N.B.; Webber, E.M.; Goddard, K.A.; Scrol, A.; Piper, M.; Williams, M.S.; Zallen, D.T.; Calgone, N.; Ganiats, T.G.; Janssens, A.C.J.W.; et al. Family history and the natural history of colorectal cancer: Systematic review. Genet. Med. 2015, 17, 702–712. [Google Scholar] [CrossRef]
- Renkonen, S.; Lee, M.; Mäkitie, A.; Lindström, L.S.; Czene, K. Site-specific familial risk and survival of familial and sporadic head and neck cancer. Int. J. Cancer 2017, 141, 497–502. [Google Scholar] [CrossRef]
- Seven, M.; Bağcivan, G.; Akyuz, A.; Bölükbaş, F. Women with Family History of Breast Cancer: How Much Are They Aware of Their Risk? J. Cancer Educ. 2018, 33, 915–921. [Google Scholar] [CrossRef]
- Miller, M.; Bailey, B.; Govindarajah, V.; Levin, L.; Metzger, T.; Pinney, S.M.; Leung, Y.-K.; Ho, S.-M. A community survey on knowledge of the impact of environmental and epigenetic factors on health and disease. Perspect. Public Health 2016, 136, 345–352. [Google Scholar] [CrossRef]
- Weinrich, S.; Vijayakumar, S.; Powell, I.J.; Priest, J.; Hamner, C.A.; McCloud, L.; Pettaway, C. Knowledge of Hereditary Prostate Cancer Among High-Risk African American Men. Oncol. Nurs. Forum 2007, 34, 854–860. [Google Scholar] [CrossRef]
- Amin, T.T.; Al-Wadaani, H.A.; Al-Quaimi, M.M.; Aldairi, N.A.; Alkhateeb, J.M.; Al-Jaafari, A.A.L. Saudi women’s interest in breast cancer gene testing: Possible influence of awareness, perceived risk and sociodemographic factors. Asian Pac. J. Cancer Prev. 2012, 13, 3879–3887. [Google Scholar] [CrossRef]
- Hann, K.E.J.; Freeman, M.; Fraser, L.; Waller, J.; Sanderson, S.C.; Rahman, B.; Side, L.; Gessler, S.; Lanceley, A.; PROMISE study team. Awareness, knowledge, perceptions, and attitudes towards genetic testing for cancer risk among ethnic minority groups: A systematic review. BMC Public Health 2017, 17, 503. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.C.; Foss, K.S.; Henderson, G.E.; Powell, S.N.; Saylor, K.W.; Weck, K.E.; Milko, L.V. Public Interest in Population Genetic Screening for Cancer Risk. Front. Genet. 2022, 13, 886640. [Google Scholar] [CrossRef] [PubMed]
- Al-Gamal, E.; Othman, A.; Nasrallah, E. Knowledge, Attitudes and Practices towards Cancer Prevention and Care in Jordan. 2011. Available online: https://www.researchgate.net/publication/266731359 (accessed on 28 September 2022).
- Kolak, A.; Kamińska, M.; Sygit, K.; Budny, A.; Surdyka, D.; Kukiełka-Budny, B.; Burdan, F. Primary and secondary prevention of breast cancer. Ann. Agric. Environ. Med. 2017, 24, 549–553. [Google Scholar] [CrossRef] [PubMed]
- El-Mouzan, M.I.; Al-Salloum, A.A.; Al-Herbish, A.S.; Qurachi, M.M.; Al-Omar, A.A. Regional Variations in the Prevalence of Consanguinity in Saudi Arabia. Available online: www.smj.org.sa (accessed on 28 September 2022).
- Kamal, N.M. Consanguinity Marriage Increases Risk of Newborn’s Congenital Anomalies in Sulaimani City. Available online: www.intechopen.com (accessed on 28 September 2022).
- Tayebi, N.; Yazdani, K.; Naghshin, N. The Prevalence of Congenital Malformations and its Correlation with Consanguineous Marriages. Oman Med. J. 2010, 25, 37–40. [Google Scholar] [CrossRef]
- Bener, A.; Ayoubi, H.R.E.; Chouvhane, L.; Ali, A.I.; Al-Kubaisi, A.; Al-Sulaiti, H.; Teebi, A.S. Impact of Consanguinity on Cancer in a Highly EndogamousPopulation. Asian Pac. J. Cancer Prev. 2009, 10, 35–40. Available online: http://journal.waocp.org/article_24870_fe108a42c173546fe9df297d55be2c59.pdf (accessed on 19 December 2021).
- Olusola, P.; Banerjee, H.N.; Philley, J.V.; Dasgupta, S. Human papilloma virus-associated cervical cancer and health disparities. Cells 2019, 8, 622. [Google Scholar] [CrossRef]
- Kurian, A.W.; Ward, K.C.; Howlader, N.; Deapen, D.; Hamilton, A.S.; Mariotto, A.; Miller, D.; Penberthy, L.S.; Katz, S.J. Genetic testing and results in a population-based cohort of breast cancer patients and ovarian cancer patients. J. Clin. Oncol. 2019, 37, 1305. [Google Scholar] [CrossRef]
- Scott, D.; Friedman, S.; Telli, M.L.; Kurian, A.W. Decision Making about Genetic Testing among Women with a Personal and Family History of Breast Cancer. JCO Oncol. Pract. 2020, 16, e37–e55. [Google Scholar] [CrossRef]
- Gosadi, I.M. National screening programs in Saudi Arabia: Overview, outcomes, and effectiveness. J. Infect. Public Health 2019, 12, 608–614. [Google Scholar] [CrossRef]
- van Wyk, C.; Wessels, T.M.; Kromberg, J.G.R.; Krause, A. Knowledge regarding basic concepts of hereditary cancers, and the available genetic counseling and testing services: A survey of general practitioners in Johannesburg, South Africa. S. Afr. Med. J. 2016, 106, 268–271. [Google Scholar] [CrossRef] [PubMed]
- Tzeng, I.S. Dealing with the Problem of Monotone Likelihood in the Inflation of Estimated Effects in Clinical Studies. Comment on Hasegawa et al. Impact of Blood Type O on Mortality of Sepsis Patients: A Multicenter Retrospective Observational Study. Diagnostics 2020, 10, 826. Available online: https://www.mdpi.com/2075-4418/12/10/2295 (accessed on 28 September 2022).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).