
Comparative Analysis of Laparoscopic and Robotic Transperitoneal Adrenalectomy Performed at a Single Institution

Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Patients
2.3. Statistics and Ethical Considerations
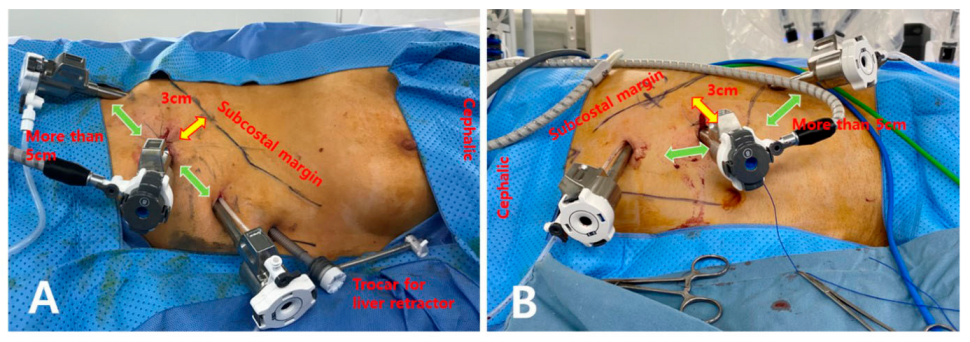
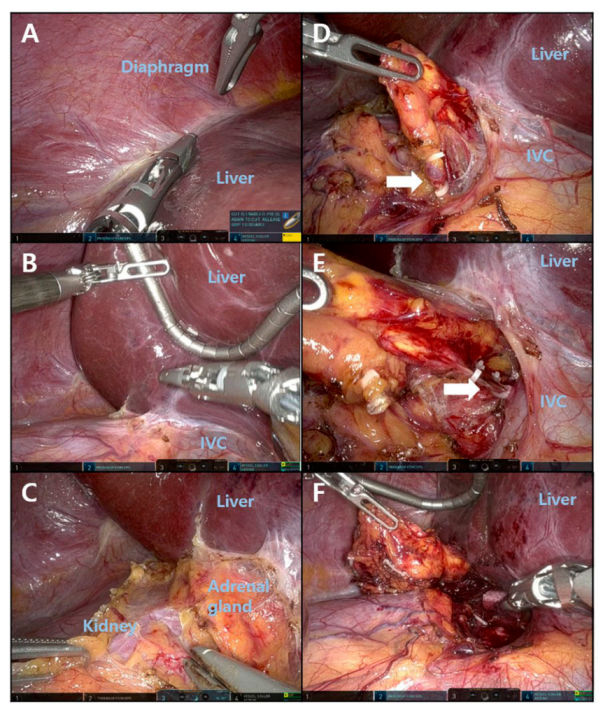
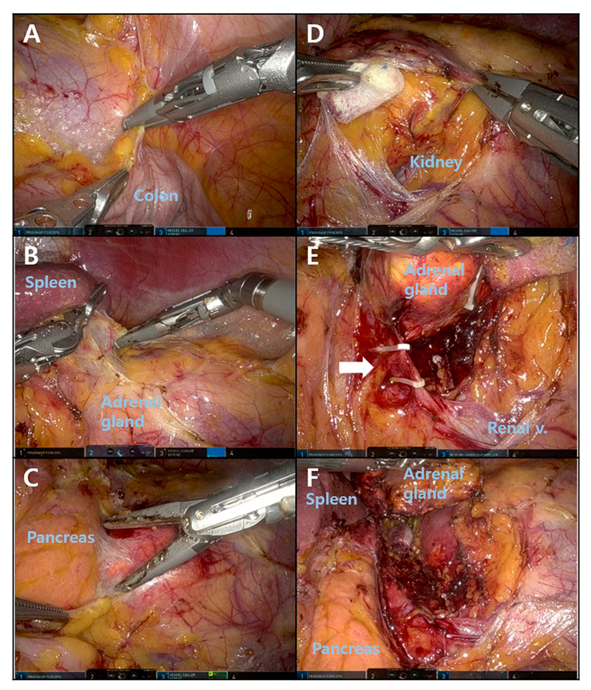
2.4. Operative Procedure for RA
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shah, M.H.; Goldner, W.S.; Benson, A.B.; Bergsland, E.; Blaszkowsky, L.S.; Brock, P.; Chan, J.; Das, S.; Dickson, P.V.; Fanta, P. Neuroendocrine and adrenal tumors, version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 839–868. [Google Scholar] [CrossRef]
- Thornton, J. Abdominal nephrectomy for large sarcoma of the left suprarenal capsule: Recovery. Trans. Clin. Soc. Lond. 1890, 23, 150–153. [Google Scholar]
- Hughes, S.; Lynn, J. Surgical anatomy and surgery of the adrenal glands. In Surgical Endocrinology; Elsevier: Amsterdam, The Netherlands, 1993; pp. 458–467. [Google Scholar]
- Mayo, C.H. Paroxysmal hypertension with tumor of retroperitoneal nerve: Report of case. J. Am. Med. Assoc. 1927, 89, 1047–1050. [Google Scholar] [CrossRef]
- Harris, D.A.; Wheeler, M.H. History of adrenal surgery. In Adrenal Glands; Springer: Berlin/Heidelberg, Germany, 2005; pp. 1–6. [Google Scholar]
- Gagner, M. Laparoscopic adrenalectomy in Cushing’s syndrome and pheochromocytoma. N. Engl. J. Med. 1992, 327, 1033. [Google Scholar] [PubMed]
- Mercan, S.; Seven, R.; Ozarmagan, S.; Tezelman, S. Endoscopic retroperitoneal adrenalectomy. Surgery 1995, 118, 1071–1076. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.D.; Weber, C.J.; Amerson, J.R. Laparoscopic adrenalectomy: New gold standard. World J. Surg. 1999, 23, 389. [Google Scholar] [CrossRef]
- Piazza, L.; Caragliano, P.; Scardilli, M.; Sgroi, A.; Marino, G.; Giannone, G. Laparoscopic robot-assisted right adrenalectomy and left ovariectomy. Chir. Ital. 1999, 51, 465–466. [Google Scholar]
- Horgan, S.; Vanuno, D. Robots in laparoscopic surgery. J. Laparoendosc. Adv. Surg. Tech. 2001, 11, 415–419. [Google Scholar] [CrossRef]
- Grogan, R.H. Current status of robotic adrenalectomy in the United States. Gland Surg. 2020, 9, 840. [Google Scholar] [CrossRef]
- Makay, O.; Erol, V.; Ozdemir, M. Robotic adrenalectomy. Gland Surg. 2019, 8, S10. [Google Scholar] [CrossRef]
- Palep, J.H. Robotic assisted minimally invasive surgery. J. Minimal Access Surg. 2009, 5, 1. [Google Scholar] [CrossRef] [PubMed]
- Economopoulos, K.P.; Mylonas, K.S.; Stamou, A.A.; Theocharidis, V.; Sergentanis, T.N.; Psaltopoulou, T.; Richards, M.L. Laparoscopic versus robotic adrenalectomy: A comprehensive meta-analysis. Int. J. Surg. 2017, 38, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Nomine-Criqui, C.; Demarquet, L.; Schweitzer, M.L.; Klein, M.; Brunaud, L.; Bihain, F. Robotic adrenalectomy: When and how? Gland Surg. 2020, 9, S166–S172. [Google Scholar] [CrossRef]
- Chai, Y.J.; Yu, H.W.; Song, R.-Y.; Kim, S.-J.; Choi, J.Y.; Lee, K.E. Lateral transperitoneal adrenalectomy versus posterior retroperitoneoscopic adrenalectomy for benign adrenal gland disease: Randomized controlled trial at a single tertiary medical center. Ann. Surg. 2019, 269, 842–848. [Google Scholar] [CrossRef] [PubMed]
- Winter, J.; Talamini, M.; Stanfield, C.; Chang, D.; Hundt, J.; Dackiw, A.; Campbell, K.; Schulick, R. Thirty robotic adrenalectomies. Surg. Endosc. Other Interv. Tech. 2006, 20, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Brunaud, L.; Ayav, A.; Zarnegar, R.; Rouers, A.; Klein, M.; Boissel, P.; Bresler, L. Prospective evaluation of 100 robotic-assisted unilateral adrenalectomies. Surgery 2008, 144, 995–1001. [Google Scholar] [CrossRef] [PubMed]
- Giulianotti, P.; Buchs, N.; Addeo, P.; Bianco, F.; Ayloo, S.; Caravaglios, G.; Coratti, A. Robot-assisted adrenalectomy: A technical option for the surgeon? Int. J. Med. Robot. Comput. Assist. Surg. 2011, 7, 27–32. [Google Scholar] [CrossRef]
- Nordenström, E.; Westerdahl, J.; Hallgrimsson, P.; Bergenfelz, A. A prospective study of 100 robotically assisted laparoscopic adrenalectomies. J. Robot. Surg. 2011, 5, 127–131. [Google Scholar] [CrossRef]
- Agcaoglu, O.; Aliyev, S.; Karabulut, K.; Siperstein, A.; Berber, E. Robotic vs laparoscopic posterior retroperitoneal adrenalectomy. Arch. Surg. 2012, 147, 272–275. [Google Scholar] [CrossRef]
- D’Annibale, A.; Lucandri, G.; Monsellato, I.; De Angelis, M.; Pernazza, G.; Alfano, G.; Mazzocchi, P.; Pende, V. Robotic adrenalectomy: Technical aspects, early results and learning curve. Int. J. Med. Robot. Comput. Assist. Surg. 2012, 8, 483–490. [Google Scholar] [CrossRef]
- Aksoy, E.; Taskin, H.E.; Aliyev, S.; Mitchell, J.; Siperstein, A.; Berber, E. Robotic versus laparoscopic adrenalectomy in obese patients. Surg. Endosc. 2013, 27, 1233–1236. [Google Scholar] [CrossRef] [PubMed]
- Aliyev, S.; Karabulut, K.; Agcaoglu, O.; Wolf, K.; Mitchell, J.; Siperstein, A.; Berber, E. Robotic versus laparoscopic adrenalectomy for pheochromocytoma. Ann. Surg. Oncol. 2013, 20, 4190–4194. [Google Scholar] [CrossRef] [PubMed]
- Brandao, L.F.; Autorino, R.; Zargar, H.; Krishnan, J.; Laydner, H.; Akca, O.; Mir, M.C.; Samarasekera, D.; Stein, R.; Kaouk, J. Robot-assisted laparoscopic adrenalectomy: Step-by-step technique and comparative outcomes. Eur. Urol. 2014, 66, 898–905. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.S.; Arghami, A.; Dy, B.M.; McKenzie, T.J.; Thompson, G.B.; Richards, M.L. Robotic single-site adrenalectomy. Surg. En-dosc. 2016, 30, 3351–3356. [Google Scholar] [CrossRef]
- Morelli, L.; Tartaglia, D.; Bronzoni, J.; Palmeri, M.; Guadagni, S.; Di Franco, G.; Gennai, A.; Bianchini, M.; Bastiani, L.; Moglia, A. Robotic assisted versus pure laparoscopic surgery of the adrenal glands: A case-control study comparing surgical techniques. Langenbeck’s Arch. Surg. 2016, 401, 999–1006. [Google Scholar] [CrossRef] [PubMed]
- Greilsamer, T.; Nomine-Criqui, C.; Thy, M.; Ullmann, T.; Zarnegar, R.; Bresler, L.; Brunaud, L. Robotic-assisted unilateral adrenalectomy: Risk factors for perioperative complications in 303 consecutive patients. Surg. Endosc. 2019, 33, 802–810. [Google Scholar] [CrossRef]
- Kim, W.W.; Lee, Y.M.; Chung, K.W.; Hong, S.J.; Sung, T.Y. Comparison of robotic posterior retroperitoneal adrenalectomy over laparoscopic posterior retroperitoneal adrenalectomy: A single tertiary center experience. Int. J. Endocrinol. 2019, 2019, 9012910. [Google Scholar] [CrossRef] [Green Version]
- De Crea, C.; Arcuri, G.; Pennestrì, F.; Paolantonio, C.; Bellantone, R.; Raffaelli, M. Robotic adrenalectomy: Evaluation of cost-effectiveness. Gland Surg. 2020, 9, 831–839. [Google Scholar] [CrossRef]
- Fu, S.-Q.; Zhuang, C.-S.; Yang, X.-R.; Xie, W.-J.; Gong, B.-B.; Liu, Y.-F.; Liu, J.; Sun, T.; Ma, M. Comparison of robot-assisted retroperitoneal laparoscopic adrenalectomy versus retroperitoneal laparoscopic adrenalectomy for large pheochromocytoma: A single-centre retrospective study. BMC Surg. 2020, 20, 227. [Google Scholar] [CrossRef]
- Ji, C.; Lu, Q.; Chen, W.; Zhang, F.; Ji, H.; Zhang, S.; Zhao, X.; Li, X.; Zhang, G.; Guo, H. Retrospective comparison of three minimally invasive approaches for adrenal tumors: Perioperative outcomes of transperitoneal laparoscopic, retroperitoneal laparoscopic and robot-assisted laparoscopic adrenalectomy. BMC Urol. 2020, 20, 66. [Google Scholar] [CrossRef]
- Ozdemir, M.; Dural, A.C.; Sahbaz, N.A.; Akarsu, C.; Uc, C.; Sertoz, B.; Alis, H.; Makay, O. Robotic transperitoneal adrenalectomy from inception to ingenuity: The perspective on two high-volume endocrine surgery centers. Gland Surg. 2020, 9, 815–825. [Google Scholar] [CrossRef] [PubMed]
- Fang, A.M.; Rosen, J.; Saidian, A.; Bae, S.; Tanno, F.Y.; Chambo, J.L.; Bloom, J.; Gordetsky, J.; Srougi, V.; Phillips, J.; et al. Perioperative outcomes of laparoscopic, robotic, and open approaches to pheochromocytoma. J. Robot. Surg. 2020, 14, 849–854. [Google Scholar] [CrossRef] [PubMed]
- Agcaoglu, O.; Karahan, S.N.; Tufekci, T.; Tezelman, S. Single-incision robotic adrenalectomy (SIRA): The future of adrenal sur-gery? Gland Surg. 2020, 9, 853–858. [Google Scholar] [CrossRef] [PubMed]
- Knežević, N.; Penezić, L.; Kuliš, T.; Zekulić, T.; Saić, H.; Hudolin, T.; Kaštelan, Ž. Senhance robot-assisted adrenalectomy: A case series. Croat. Med. J. 2022, 63, 197–201. [Google Scholar] [CrossRef]
- Erdemir, A.; Rasa, K. Robotic adrenalectomy: An initial experience in a Turkish regional hospital. Front. Surg. 2022, 9, 847472. [Google Scholar] [CrossRef] [PubMed]
- Al-Thani, H.; Al-Thani, N.; Al-Sulaiti, M.; Tabeb, A.; Asim, M.; El-Menyar, A. A descriptive comparative analysis of the surgical management of adrenal tumors: The open, robotic, and laparoscopic approaches. Front. Surg. 2022, 9, 848565. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.E.; Rao, J.; Youn, Y.-K. Endoscopic thyroidectomy with the da Vinci robot system using the bilateral axillary breast ap-proach (BABA) technique: Our initial experience. Surg. Laparosc. Endosc. Percutaneous Tech. 2009, 19, e71–e75. [Google Scholar] [CrossRef]
- Yang, H.K.; Suh, Y.S.; Lee, H.J. Minimally invasive approaches for gastric cancer—Korean experience. J. Surg. Oncol. 2013, 107, 277–281. [Google Scholar] [CrossRef]
- Mendoza, A.S., III; Han, H.S.; Yoon, Y.S.; Cho, J.Y.; Choi, Y. Laparoscopy-assisted pancreaticoduodenectomy as minimally in-vasive surgery for periampullary tumors: A comparison of short-term clinical outcomes of laparoscopy-assisted pancreaticoduodenectomy and open pancreaticoduodenectomy. J. Hepato-Biliary-Pancreat. Sci. 2015, 22, 819–824. [Google Scholar] [CrossRef]
- Barbash, G.I. New technology and health care costs—The case of robot-assisted surgery. N. Engl. J. Med. 2010, 363, 701. [Google Scholar] [CrossRef] [Green Version]
- Yeganeh, H. An analysis of emerging trends and transformations in global healthcare. Int. J. Health Gov. 2019, 24, 169–180. [Google Scholar] [CrossRef]
- Park, J.H.; Walz, M.K.; Kang, S.-W.; Jeong, J.-J.; Nam, K.-H.; Chang, H.-S.; Chung, W.-Y.; Park, C.-S. Robot-assisted posterior retroperitoneoscopic adrenalectomy: Single port access. J. Korean Surg. Soc. 2011, 81, S21–S24. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 56) | RA (n = 24) | LA (n = 32) | p-Value |
|---|---|---|---|---|
| Age (years, mean ± SD) | 52.9 ± 11.2 (25–76) | 48.6 ± 9.7 (29–71) | 56.1 ± 11.4 (25–76) | 0.013 |
| Gender | ||||
| Male | 28 (50%) | 12 (21%) | 16 (29%) | 1.000 |
| Female | 28 (50%) | 12 (21%) | 16 (29%) | |
| BMI a (kg/m2, mean ± SD) | 25.9 ± 4.4 (17.3–35.0) | 26.6 ± 4.9 (18.2–35.0) | 25.4 ± 4.1 (17.3–32.7) | 0.344 |
| Clinical diagnosis | ||||
| Primary aldosteronism | 16 (28.6%) | 9 (37.5%) | 7 (21.9%) | |
| Cushing’s syndrome | 14 (25.0%) | 6 (25.0%) | 8 (25%) | |
| Non-functioning Adenoma | 12 (21.4%) | 3 (12.5%) | 9 (28.1%) | |
| PPGLs b | 9 (16.1%) | 5 (20.8%) | 4 (12.5%) | |
| r/o Metastatic mass | 3 (5.4%) | 1 (4.2%) | 2 (6.25%) | |
| Adrenal cortical cancer | 2 (3.6%) | 0 (0.0%) | 2 (6.25%) | |
| Tumor location | ||||
| Right | 27 (48%) | 14 (25%) | 13 (23%) | 0.196 |
| Left | 29 (52%) | 10 (18%) | 19 (34%) | |
| Tumor size (cm, mean ± SD) | 3.5 ± 2.2 (1.3–9.6) | 3.1 ± 1.8 (1.3–8.0) | 3.8 ± 2.4 (1.3–9.6) | 0.269 |
| Combined operation | 3 | |||
| Cholecystectomy | 2 | 2 | 1 | |
| Partial nephrectomy | 1 | 2 | 0 | |
| TH + BSO c | 3 | 1 | 0 |
| Variable | Total (n = 56) | RA (n = 24) | LA (n = 32) | p-Value |
|---|---|---|---|---|
| Operation time (minute, mean ± SD) | 100.0 ± 48.6 (46–295) | 76.1 ± 28.2 (46–140) | 118.0 ± 54.3 (60–295) | <0.001 |
| Estimated blood loss (mL, mean ± SD) | 152.1 ± 132.7 (0–400) | 164.6 ± 144.8 (0–400) | 142.8 ± 124.5 (0–400) | 0.548 |
| Hospital stay after operation (days, mean ± SD) | 4.0 ± 1.9 (2–9) | 4.3 ± 2.1 (2–9) | 3.8 ± 1.7 (2–9) | 0.326 |
| Visual analog scale | ||||
| Postoperative day 1 (0–10, mean ± SD) | 2.9 ± 0.6 (0–5) | 2.9 ± 0.9 (0–5) | 2.9 ± 0.4 (2–4) | 0.737 |
| Postoperative day 2 (0–10, mean ± SD) | 2.5 ± 0.7 (0–3) | 2.5 ± 0.8 (0–3) | 2.5 ± 0.7 (1–3) | 0.873 |
| Complication | ||||
| Port-site hernia | 1 (1.8%) | 0 (0.0%) | 1 (3.1%) | 0.382 |
| Cost of surgery (US dollar c, mean ± SD) | 2528.8 ± 2422.5 (352.8–5288.5) | 5288.5 | 441.5 ± 136.8 (352.8–1167.1) | <0.001 |
| Pathologic diagnosis | ||||
| Adrenal cortical adenoma | 35 (62.5%) | 16 (66.7%) | 19 (59.4%) | |
| PPGLs a | 6 (10.7%) | 5 (20.8%) | 1 (3.1%) | |
| Myelolipoma | 5 (8.9%) | 2 (3.6%) | 3 (9.4%) | |
| Adrenal cortical cancer | 2 (3.6%) | 0 (0.0%) | 2 (6.3%) | |
| Others b | 8 (14.3%) | 1 (4.2%) | 7 (21.9%) |
| Year | Study Design | Patient (n) | Tumor Size (cm) | Operation Time (min) | |
|---|---|---|---|---|---|
| 2006 | Winter [17] | Case series | 30 | 2.4 | 185 |
| 2008 | Brunaaud [18] | Case series | 100 | 2.9 | 171 |
| 2011 | Giulianotti [19] | Case series | 42 | 5.5 | 118 |
| 2011 | Nordenström [20] | Case series | 100 | 5.3 | 113 |
| 2012 | Agcaoglu [21] | Comparative | 31 | 3.1 | 163.2 |
| 2012 | D’Annibale [22] | Case series | 30 | 5.1 | 200 |
| 2013 | Aksoy [23] | Comparative | 42 | 4.0 | 186 |
| 2013 | Aliyev [24] | Comparative | 26 | - | 149 |
| 2014 | Brandao [25] | Comparative | 30 | 3 | 120 |
| 2016 | Lee [26] | Case series | 33 | - | 234 |
| 2016 | Morelli [27] | Comparative | 41 | - | 177 |
| 2019 | Greilsamer [28] | Case series | 303 | 3.6 | 89 |
| 2019 | Kim [29] | Comparative | 61 | 3.7 | 138 |
| 2020 | Carmela [30] | Comparative | 12 | - | 93.3 |
| 2020 | Fu [31] | Comparative | 19 | 8 | 166.3 |
| 2020 | Changwei [32] | Comparative | 87 | 4.7 | 136.1 |
| 2020 | Ozdemir [33] | Case series | 111 | 3.9 | 135.4 |
| 2020 | Fang [34] | Comparative | 41 | 6.2 | 210.4 |
| 2021 | Piccoli [35] | Comparative | 76 | 4.0 | 100.3 |
| 2022 | Knežević [36] | Case series | 12 | - | 165.1 |
| 2022 | Erdemir [37] | Case series | 30 | 8.3 | 194.9 |
| 2022 | Al-Thani [38] | Comparative | 76 | 4.8 | 174 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, Y.S.; Lee, J.S.; Yi, J.W. Comparative Analysis of Laparoscopic and Robotic Transperitoneal Adrenalectomy Performed at a Single Institution. Medicina 2022, 58, 1747. https://doi.org/10.3390/medicina58121747
Choi YS, Lee JS, Yi JW. Comparative Analysis of Laparoscopic and Robotic Transperitoneal Adrenalectomy Performed at a Single Institution. Medicina. 2022; 58(12):1747. https://doi.org/10.3390/medicina58121747
Chicago/Turabian StyleChoi, Yun Suk, Ji Sun Lee, and Jin Wook Yi. 2022. "Comparative Analysis of Laparoscopic and Robotic Transperitoneal Adrenalectomy Performed at a Single Institution" Medicina 58, no. 12: 1747. https://doi.org/10.3390/medicina58121747