
Characteristics of Surface Electromyograph Activity of Cervical Extensors and Flexors in Nonspecific Neck Pain Patients: A Cross-Sectional Study


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.1.1. Participants of NSNP and Control Groups
2.1.2. Inclusion and Exclusion Criteria of the NSNP Group
- Inclusion criteria: Patients with pain in the neck and/or shoulder.
- Exclusion criteria: Patients who had neither pain nor stiffness in the neck and shoulder; patients with neurological symptoms such as numbness or hypesthesia in the neck, shoulder, and upper extremity; and patients who suffered from cervical spine diseases such as cervical disc herniation, central and peripheral neuropathy, rheumatoid arthritis, or medical diseases [27].
2.1.3. Inclusion and Exclusion Criteria of the Control Group
- Inclusion criteria: Patients with neither pain nor stiffness in the neck, shoulder and/or upper extremity, and no neurological symptoms such as numbness or hypesthesia.
- Exclusion criteria: Patients who had pain or stiffness in the neck, shoulder, and upper extremity, or who had neurological symptoms such as numbness or hypesthesia, cervical spine disease such as cervical disc herniation, central and peripheral neuropathy, rheumatoid arthritis, or medical disease [25].
2.2. Procedures for Measuring Cervical Muscle Activity
2.2.1. Surface Electromyogram (sEMG)
2.2.2. Procedures for Measuring Muscle Activity
2.3. Assessment of Head and Neck Posture
2.4. Evaluation of NSNP
2.5. Data Analysis
2.5.1. Calculation of Grand Ensemble Average
2.5.2. Calculation of Muscle Activity Ratio
2.5.3. Calculation of CVA
2.6. Statistical Analysis
3. Results
3.1. Demographics
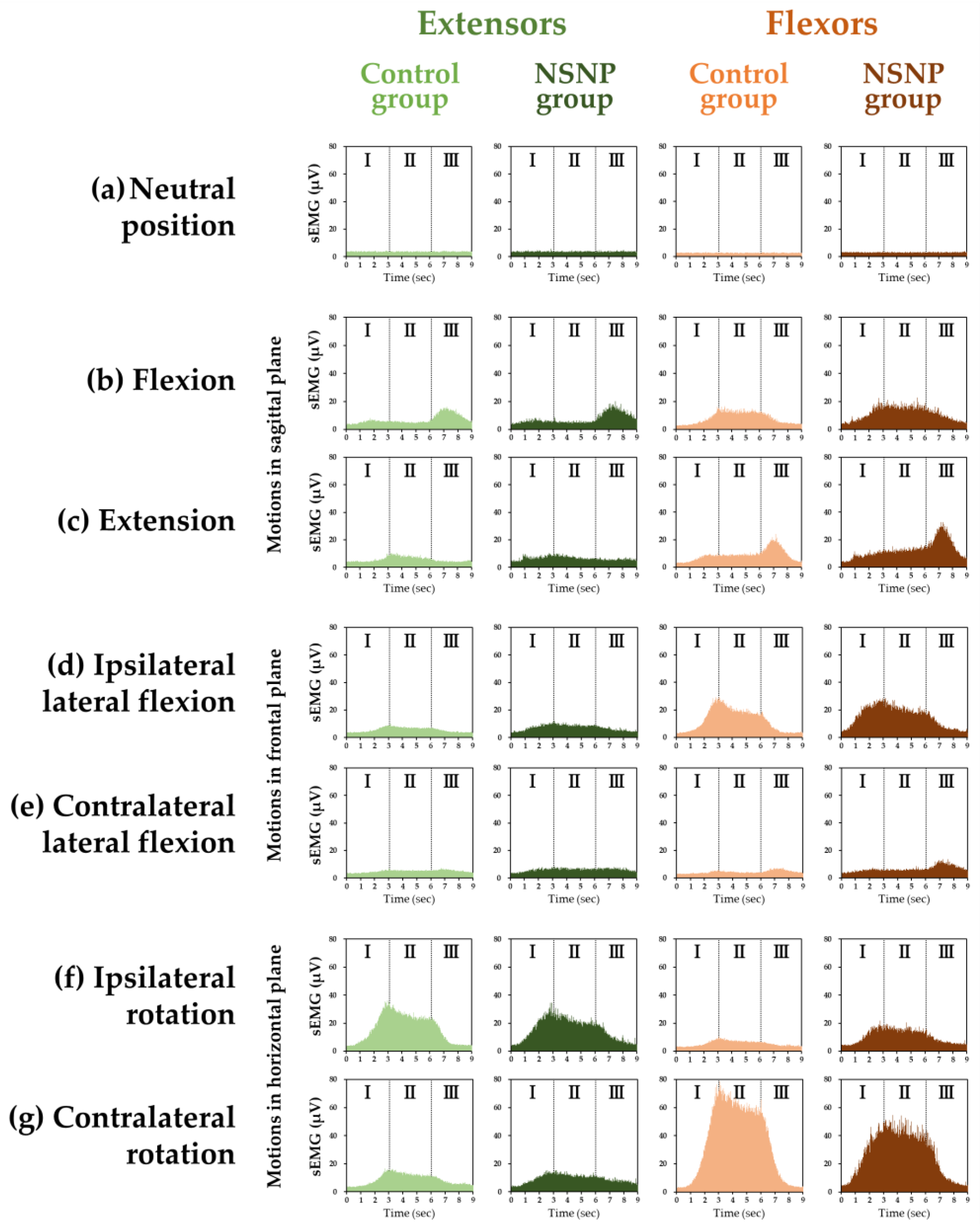
3.2. Grand Ensemble Average in Healthy Participants and NSNP Patients
3.3. Ratio of Muscle Activity of Each Motion to the Neutral Position in the NSNP and Control Groups
3.4. Flexor–Extensor Ratios in the NSNP and Control Groups
3.5. CVA in the NSNP and Control Groups
3.5.1. Comparison of the NSNP and Control Groups
3.5.2. Correlation of CVA and Flexion–Extension Ratio in the Neutral Position
4. Discussion
4.1. Ratio of Muscle Activity in Motions to the Neutral Position in Each Phase in the Extensors and Flexors
4.2. Flexor–Extensor Ratio in Each Phase in Each Motion
4.3. Relationship between Neck Posture and Cervical Muscle Activity
4.4. Clinical Significance
4.5. Limitations and Strengths
4.6. Overall Interpretation of the Results
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hidalgo, B.; Hall, T.; Bossert, J.; Dugeny, A.; Cagnie, B.; Pitance, L. The efficacy of manual therapy and exercise for treating non-specific neck pain: A systematic review. J. Back Musculoskelet. Rehabil. 2017, 30, 1149–1169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Price, J.; Rushton, A.; Tyros, I.; Heneghan, N.R. Effectiveness and optimal dosage of resistance training for chronic non-specific neck pain: A protocol for a systematic review with a qualitative synthesis and meta-analysis. BMJ Open 2019, 9, e025158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoving, L.; Koes, B.W.; de Vet, H.C.; van der Windt, D.A.; Assendelft, W.J.; van Mameren, H.; Devillé, W.L.; Pool, J.J.; Scholten, R.J.; Bouter, L.M. Manual therapy, physical therapy, or continued care by a general practitioner for patients with neck pain. A randomized, controlled trial. Ann. Intern. Med. 2002, 136, 713–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binder, A.I. Cervical spondylosis and neck pain. BMJ 2007, 334, 527–531. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.; Jaiswal, P.; Chhabra, D. A comparative study between postisometric relaxation and isometric exercises in non-specific neck pain. J. Exerc. Sci. Phys. 2008, 4, 88–94. [Google Scholar] [CrossRef] [Green Version]
- Panjabi, M.M.; Cholewicki, J.; Nibu, K.; Grauer, J.; Babat, L.B.; Dvorak, J. Critical load of the human cervical spine: An in vitro experimental study. Clin. Biomech. 1998, 13, 11–17. [Google Scholar] [CrossRef]
- Ming, Z.; Närhi, M.; Siivola, J. Neck and shoulder pain related to computer use. Pathophysiology 2004, 11, 51–56. [Google Scholar] [CrossRef]
- Akagi, R.; Kusama, S. Comparison between neck and shoulder stiffness determined by shear wave ultrasound elastography and a muscle hardness meter. Ultrasound Med. Biol. 2015, 41, 2266–2271. [Google Scholar] [CrossRef]
- Kumar, S.; Prasad, N. Cervical EMG profile differences between patients of neck pain and control. Disabil. Rehabil. 2010, 32, 2078–2087. [Google Scholar] [CrossRef]
- Airaksinen, M.K.; Kankaanpää, M.; Aranko, O.; Leinonen, V.; Arokoski, J.P.; Airaksinen, O. Wireless on-line electromyography in recording neck muscle function: A pilot study. Pathophysiology 2005, 12, 303–306. [Google Scholar] [CrossRef]
- Murphy, B.A.; Marshall, P.W.; Taylor, H.H. The cervical flexion-relaxation ratio: Reproducibility and comparison between chronic neck pain patients and controls. Spine 2010, 35, 2103–2108. [Google Scholar] [CrossRef] [PubMed]
- Maroufi, N.; Ahmadi, A.; Mousavi Khatir, S.R. A comparative investigation of flexion relaxation phenomenon in healthy and chronic neck pain subjects. Eur. Spine J. 2013, 22, 162–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jull, G.; Kristjansson, E.; Dall'Alba, P. Impairment in the cervical flexors: A comparison of whiplash and insidious onset neck pain patients. Man. Ther. 2004, 9, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Johnston, V.; Jull, G.; Souvlis, T.; Jimmieson, N.L. Neck movement and muscle activity characteristics in female office workers with neck pain. Spine 2008, 33, 555–563. [Google Scholar] [CrossRef]
- Ylinen, J.; Salo, P.; Nykänen, M.; Kautiainen, H.; Häkkinen, A. Decreased isometric neck strength in women with chronic neck pain and the repeatability of neck strength measurements. Arch. Phys. Med. Rehabil. 2004, 85, 1303–1308. [Google Scholar] [CrossRef]
- Rezasoltani, A.; Ali-Reza, A.; Khosro, K.K.; Abbass, R. Preliminary study of neck muscle size and strength measurements in females with chronic non-specific neck pain and healthy control subjects. Man. Ther. 2010, 15, 400–403. [Google Scholar] [CrossRef]
- Peolsson, A.; Kjellman, G. Neck muscle endurance in nonspecific patients with neck pain and in patients after anterior cervical decompression and fusion. J. Manip. Physiol. Ther. 2007, 30, 343–350. [Google Scholar] [CrossRef]
- Reddy, R.S.; Tedla, J.S.; Alshahrani, M.S.; Asiri, F.; Kakaraparthi, V.N. Comparison and correlation of cervical proprioception and muscle endurance in general joint hypermobility participants with and without non-specific neck pain-a cross-sectional study. PeerJ. 2022, 10, e13097. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Albert-Sanchís, J.C.; Buil, M.; Benitez, J.C.; Alburquerque-Sendín, F. Cross-sectional area of cervical multifidus muscle in females with chronic bilateral neck pain compared to controls. J. Orthop. Sport. Phys. Ther. 2008, 38, 175–180. [Google Scholar] [CrossRef]
- Shamsi, H.; Khademi-Kalantari, K.; Akbarzadeh-Baghban, A.; Izadi, N.; Okhovatian, F. Cervical flexion relaxation phenomenon in patients with and without non-specific chronic neck pain. J. Back Musculoskelet Rehabil. 2021, 34, 4614–4668. [Google Scholar] [CrossRef]
- Dieterich, A.V.; Andrade, R.J.; Le Sant, G.; Falla, D.; Petzke, F.; Hug, F.; Nordez, A. Shear wave elastography reveals different degrees of passive and active stiffness of the neck extensor muscles. Eur. J. Appl. Physiol. 2017, 117, 171–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennett, S.E.; Schenk, R.J.; Simmons, E.D. Active range of motion utilized in the cervical spine to perform daily functional tasks. J. Spinal Disord. Tech. 2002, 15, 307–311. [Google Scholar] [CrossRef] [PubMed]
- van den Heuvel, S.G.; van der Beek, A.J.; Blatter, B.M.; Bongers, P.M. Do work-related physical factors predict neck and upper limb symptoms in office workers? Int. Arch. Occup. Environ. Health 2006, 79, 585–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ariëns, G.A.; Bongers, P.M.; Hoogendoorn, W.E.; van der Wal, G.; van Mechelen, W. High physical and psychosocial load at work and sickness absence due to neck pain. Scand. J. Work Environ. Health 2002, 28, 222–231. [Google Scholar] [CrossRef]
- Yajima, H.; Nobe, R.; Takayama, M.; Takakura, N. The mode of activity of cervical extensors and flexors in healthy adults: A cross-sectional study. Medicina 2022, 58, 728. [Google Scholar] [CrossRef]
- Netto, K.J.; Burnett, A.F. Reliability of normalisation methods for EMG analysis of neck muscles. Work 2006, 26, 123–130. [Google Scholar]
- Cramer, H.; Lauche, R.; Hohmann, C.; Lüdtke, R.; Haller, H.; Michalsen, A.; Langhorst, J.; Dobos, G. Randomized-controlled trial comparing yoga and home-based exercise for chronic neck pain. Clin. J. Pain 2013, 29, 216–223. [Google Scholar] [CrossRef]
- Burnett, A.; O'Sullivan, P.; Caneiro, J.P.; Krug, R.; Bochmann, F.; Helgestad, G.W. An examination of the flexion-relaxation phenomenon in the cervical spine in lumbo-pelvic sitting. J. Electromyogr. Kinesiol. 2009, 19, e229–e236. [Google Scholar] [CrossRef]
- Falla, D.; Dall'Alba, P.; Rainoldi, A.; Merletti, R.; Jull, G. Location of innervation zones of sternocleidomastoid and scalene muscles-a basis for clinical and research electromyography applications. Clin. Neurophysiol. 2002, 113, 57–63. [Google Scholar] [CrossRef]
- Benatto, M.T.; Florencio, L.L.; Bragatto, M.M.; Lodovichi, S.S.; Dach, F.; Bevilaqua-Grossi, D. Extensor/flexor ratio of neck muscle strength and electromyographic activity of individuals with migraine: A cross-sectional study. Eur. Spine J. 2019, 28, 2311–2318. [Google Scholar] [CrossRef]
- Zabihhosseinian, M.; Holmes, M.W.; Ferguson, B.; Murphy, B. Neck muscle fatigue alters the cervical flexion relaxation ratio in sub-clinical neck pain patients. Clin. Biomech. 2015, 30, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Mousavi-Khatir, R.; Talebian, S.; Maroufi, N.; Olyaei, G.R. Effect of static neck flexion in cervical flexion-relaxation phenomenon in healthy males and females. J. Bodyw. Mov. 2016, 20, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Salahzadeh, Z.; Maroufi, N.; Ahmadi, A.; Behtash, H.; Razmjoo, A.; Gohari, M.; Parnianpour, M. Assessment of forward head posture in females: Observational and photogrammetry methods. J. Back Musculoskelet Rehabil. 2014, 27, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Shaghayegh Fard, B.; Ahmadi, A.; Maroufi, N.; Sarrafzadeh, J. Evaluation of forward head posture in sitting and standing positions. Eur. Spine J. 2016, 25, 3577–3582. [Google Scholar] [CrossRef] [PubMed]
- Wickham, J.; Pizzari, T.; Stansfeld, K.; Burnside, A.; Watson, L. Quantifying ‘normal’ shoulder muscle activity during abduction. J. Electromyogr Kinesiol. 2010, 20, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Semciw, A.I.; Green, R.A.; Murley, G.S.; Pizzari, T. Gluteus minimus: An intramuscular EMG investigation of anterior and posterior segments during gait. Gait Posture. 2014, 39, 822–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semciw, A.I.; Freeman, M.; Kunstler, B.E.; Mendis, M.D.; Pizzari, T. Quadratus femoris: An EMG investigation during walking and running. J. Biomech. 2015, 48, 3433–3439. [Google Scholar] [CrossRef] [Green Version]
- Kiesel, K.B.; Uhl, T.L.; Underwood, F.B.; Rodd, D.W.; Nitz, A.J. Measurement of lumbar multifidus muscle contraction with rehabilitative ultrasound imaging. Man. Ther. 2007, 12, 161–166. [Google Scholar] [CrossRef]
- Farahpour, N.; Ghasemi, S.; Allard, P.; Saba, M.S. Electromyographic responses of erector spinae and lower limb's muscles to dynamic postural perturbations in patients with adolescent idiopathic scoliosis. J. Electromyogr. Kinesiol. 2014, 24, 645–651. [Google Scholar] [CrossRef]
- Fong, S.S.; Tam, Y.T.; Macfarlane, D.J.; Ng, S.S.; Bae, Y.H.; Chan, E.W.; Guo, X. Core muscle activity during TRX suspension exercises with and without kinesiology taping in adults with chronic low back pain: Implications for rehabilitation. Evid. Based Complement Altern. Med. 2015, 2015, 910168. [Google Scholar] [CrossRef]
- Yip, C.H.; Chiu, T.T.; Poon, A.T. The relationship between head posture and severity and disability of patients with neck pain. Man. Ther. 2008, 13, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Youssef, A.R. Photogrammetric quantification of forward head posture is side dependent in healthy participants and patients with mechanical neck pain. Int. J. Physiother. 2016, 3, 326–331. [Google Scholar] [CrossRef] [Green Version]
- Bokaee, F.; Rezasoltani, A.; Manshadi, F.D.; Naimi, S.S.; Baghban, A.A.; Azimi, H. Comparison of isometric force of the craniocervical flexor and extensor muscles between women with and without forward head posture. Cranio 2016, 34, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Bonilla-Barba, L.; Florencio, L.L.; Rodríguez-Jiménez, J.; Falla, D.; Fernández-de-Las-Peñas, C.; Ortega-Santiago, R. Women with mechanical neck pain exhibit increased activation of their superficial neck extensors when performing the cranio-cervical flexion test. Musculoskelet Sci. Pract. 2020, 10, 102222. [Google Scholar] [CrossRef]
- Burnett, A.F.; Cornelius, M.W.; Dankaerts, W.; O'sullivan, P.B. Spinal kinematics and trunk muscle activity in cyclists: A comparison between healthy controls and non-specific chronic low back pain subjects-a pilot investigation. Man. Ther. 2004, 9, 211–219. [Google Scholar] [CrossRef]
- Dankaerts, W.; O'Sullivan, P.; Burnett, A.; Straker, L. Differences in sitting postures are associated with nonspecific chronic low back pain disorders when patients are subclassified. Spine 2006, 31, 698–704. [Google Scholar] [CrossRef] [Green Version]
- O'Sullivan, P.B.; Mitchell, T.; Bulich, P.; Waller, R.; Holte, J. The relationship beween posture and back muscle endurance in industrial workers with flexion-related low back pain. Man. Ther. 2006, 11, 264–271. [Google Scholar] [CrossRef]
- Falla, D.; O'Leary, S.; Fagan, A.; Jull, G. Recruitment of the deep cervical flexor muscles during a postural-correction exercise performed in sitting. Man. Ther. 2007, 12, 139–143. [Google Scholar] [CrossRef]
- Falla, D.; Jull, G.; Russell, T.; Vicenzino, B.; Hodges, P. Effect of neck exercise on sitting posture in patients with chronic neck pain. Phys. Ther. 2007, 87, 408–417. [Google Scholar] [CrossRef] [Green Version]
- Jull, G.; Falla, D. Does increased superficial neck flexor activity in the craniocervical flexion test reflect reduced deep flexor activity in people with neck pain? Man. Ther. 2016, 25, 43–47. [Google Scholar] [CrossRef] [Green Version]
- Falla, D.L.; Jull, G.A.; Hodges, P.W. Patients with neck pain demonstrate reduced electromyographic activity of the deep cervical flexor muscles during performance of the craniocervical flexion test. Spine 2004, 29, 2108–2114. [Google Scholar] [CrossRef] [PubMed]
- Granata, K.P.; Marras, W.S. Cost-benefit of muscle cocontraction in protecting against spinal instability. Spine 2000, 25, 1398–1404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danna-Dos-Santos, A.; Degani, A.M.; Latash, M.L. Anticipatory control of head posture. Clin Neurophysiol. 2007, 118, 1802–1814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, C.H.; Lin, K.H.; Wang, J.L. Co-contraction of cervical muscles during sagittal and coronal neck motions at different movement speeds. Eur. J. Appl. Physiol. 2008, 103, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Lindstrøm, R.; Schomacher, J.; Farina, D.; Rechter, L.; Falla, D. Association between neck muscle coactivation, pain, and strength in women with neck pain. Man. Ther. 2011, 16, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Tsirakos, D.; Baltzopoulos, V.; Bartlett, R. Inverse optimization: Functional and physiological considerations related to the force-sharing problem. Crit Rev Biomed Eng. 1997, 25, 371–407. [Google Scholar] [CrossRef]
- Sverdlova, N.S.; Witzel, U. Principles of determination and verification of muscle forces in the human musculoskeletal system: Muscle forces to minimise bending stress. J. Biomech. 2010, 43, 387–396. [Google Scholar] [CrossRef]
- Choi, H. Quantitative assessment of co-contraction in cervical musculature. Med. Eng. Phys. 2003, 25, 133–140. [Google Scholar] [CrossRef]
- Falla, D.; Rainoldi, A.; Merletti, R.; Jull, G. Myoelectric manifestations of sternocleidomastoid and anterior scalene muscle fatigue in chronic neck pain patients. Clin. Neurophysiol. 2003, 114, 488–495. [Google Scholar] [CrossRef]
- Panjabi, M.M. The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. J. Spinal Disord. 1992, 5, 383–389. [Google Scholar] [CrossRef]
- Cholewicki, J.; McGill, S.M. Mechanical stability of the in vivo lumbar spine: Implications for injury and chronic low back pain. Clin. Biomech. 1996, 11, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Hoshino, Y.; Nakamura, K.; Kariya, Y.; Saita, K.; Ito, K. Trunk muscle weakness as a risk factor for low back pain. A 5-year prospective study. Spine 1999, 24, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Reeves, N.P.; Cholewicki, J.; Silfies, S.P. Muscle activation imbalance and low-back injury in varsity athletes. J Electromyogr Kinesiol. 2006, 16, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Hogg-Johnson, S.; van der Velde, G.; Carroll, L.J.; Holm, L.W.; Cassidy, J.D.; Guzman, J.; Côté, P.; Haldeman, S.; Ammendolia, C.; Carragee, E.; et al. The burden and determinants of neck pain in the general population: Results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. Spine 2008, 33, S39–S51. [Google Scholar] [CrossRef] [PubMed]
- Borman, P.; Keskin, D.; Ekici, B.; Bodur, H. The efficacy of intermittent cervical traction in patients with chronic neck pain. Clin. Rheumatol. 2008, 27, 1249–1253. [Google Scholar] [CrossRef] [PubMed]
- Koyuncu, E.; Ökmen, B.M.; Özkuk, K.; Taşoğlu, Ö.; Özgirgin, N. The effectiveness of balneotherapy in chronic neck pain. Clin. Rheumatol. 2016, 35, 2549–2555. [Google Scholar] [CrossRef]
- He, D.; Bo Veiersted, K.; Høstmark, A.T.; Ingulf Medbø, J. Effect of acupuncture treatment on chronic neck and shoulder pain in sedentary female workers: A 6-month and 3-year follow-up study. Pain 2004, 109, 299–307. [Google Scholar] [CrossRef]
- Vas, J.; Perea-Milla, E.; Méndez, C.; Sánchez Navarro, C.; León Rubio, J.M.; Brioso, M.; García Obrero, I. Efficacy and safety of acupuncture for chronic uncomplicated neck pain: A randomised controlled study. Pain 2006, 126, 245–255. [Google Scholar] [CrossRef]
- Witt, C.M.; Jena, S.; Brinkhaus, B.; Liecker, B.; Wegscheider, K.; Willich, S.N. Acupuncture for patients with chronic neck pain. Pain 2006, 125, 98–106. [Google Scholar] [CrossRef]
- Hróbjartsson, A.; Gøtzsche, P.C. Is the placebo powerless? An analysis of clinical trials comparing placebo with no treatment. N. Engl. J. Med. 2001, 344, 1594–1602. [Google Scholar] [CrossRef]
- Fregni, F.; Boggio, P.S.; Bermpohl, F.; Bermpohl, F.; Rigonatti, S.P.; Barbosa, E.R.; Pascual-Leone, A. Immediate placebo effect in Parkinson’s disease-is the subjective relief accompanied by objective improvement? Eur. Neurol. 2006, 36, 222–229. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NSNP 1 Group (n = 24) | Control Group (n = 24) | p-Value | ||
|---|---|---|---|---|
| Age (years) | mean ± SD | 47.5 ± 15.5 | 20.5 ± 1.4 | <0.001 |
| 95% CI | 21.2–43.8 | 20.2–20.8 | ||
| Height (cm) | mean ± SD | 160.8 ± 7.9 | 165.5 ± 8.1 | 0.040 |
| 95% CI | 158.9–162.7 | 163.6–167.4 | ||
| Weight (kg) | mean ± SD | 54.4 ± 10.4 | 61.9 ± 9.5 | 0.005 |
| 95% CI | 52.0–56.9 | 59.7–64.2 | ||
| BMI 2 (kg/m2) | mean ± SD | 20.9 ± 2.8 | 22.5 ± 2.6 | 0.020 |
| 95% CI | 20.3–21.6 | 21.9–23.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nobe, R.; Yajima, H.; Takayama, M.; Takakura, N. Characteristics of Surface Electromyograph Activity of Cervical Extensors and Flexors in Nonspecific Neck Pain Patients: A Cross-Sectional Study. Medicina 2022, 58, 1770. https://doi.org/10.3390/medicina58121770
Nobe R, Yajima H, Takayama M, Takakura N. Characteristics of Surface Electromyograph Activity of Cervical Extensors and Flexors in Nonspecific Neck Pain Patients: A Cross-Sectional Study. Medicina. 2022; 58(12):1770. https://doi.org/10.3390/medicina58121770
Chicago/Turabian StyleNobe, Ruka, Hiroyoshi Yajima, Miho Takayama, and Nobuari Takakura. 2022. "Characteristics of Surface Electromyograph Activity of Cervical Extensors and Flexors in Nonspecific Neck Pain Patients: A Cross-Sectional Study" Medicina 58, no. 12: 1770. https://doi.org/10.3390/medicina58121770