
The Expression and Prognostic Value of Cancer Stem Cell Markers, NRF2, and Its Target Genes in TAE/TACE-Treated Hepatocellular Carcinoma

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Source of RNA Samples
2.3. Reverse Transcription–Quantitative Real-Time PCR (RT-qPCR) Analysis
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Patients
3.2. Association of mRNA Expression with Clinicopathologic Characteristics
3.3. Expression of CSC Markers Associated with NQO1 Expression in Post-TAE/TACE HCCs
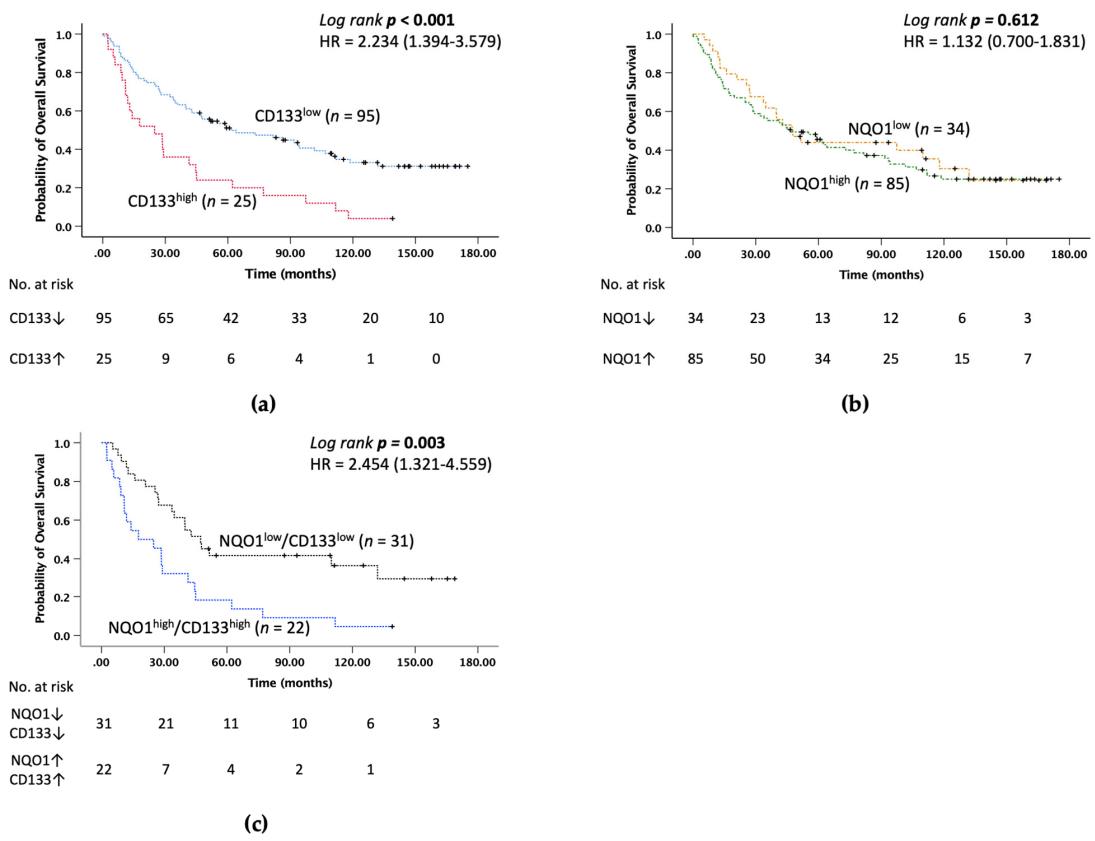
3.4. Expression of CD133 Is an Independent Prognostic Factor in HCC Patients after TAE/TACE
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Ferrarese, A.; Sciarrone, S.S.; Pellone, M.; Shalaby, S.; Battistella, S.; Zanetto, A.; Germani, G.; Russo, F.P.; Senzolo, M.; Burra, P.; et al. Current and future perspective on targeted agents and immunotherapies in hepatocellular carcinoma. Minerva Gastroenterol. 2021, 67, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Guan, Y.S.; He, Q.; Wang, M.Q. Transcatheter arterial chemoembolization: History for more than 30 years. ISRN Gastroenterol. 2012, 2012, 480650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziv, E.; Zhang, Y.; Kelly, L.; Nikolovski, I.; Boas, F.E.; Erinjeri, J.P.; Cai, L.; Petre, E.N.; Brody, L.A.; Covey, A.M.; et al. NRF2 Dysregulation in Hepatocellular Carcinoma and Ischemia: A Cohort Study and Laboratory Investigation. Radiology 2020, 297, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Tsurusaki, M.; Murakami, T. Surgical and Locoregional Therapy of HCC: TACE. Liver Cancer 2015, 4, 165–175. [Google Scholar] [CrossRef]
- Zeng, Z.; Ren, J.; O’Neil, M.; Zhao, J.; Bridges, B.; Cox, J.; Abdulkarim, B.; Schmitt, T.M.; Kumer, S.C.; Weinman, S.A. Impact of stem cell marker expression on recurrence of TACE-treated hepatocellular carcinoma post liver transplantation. BMC Cancer 2012, 12, 584. [Google Scholar] [CrossRef] [Green Version]
- Tian, W.; Rojo de la Vega, M.; Schmidlin, C.J.; Ooi, A.; Zhang, D.D. Kelch-like ECH-associated protein 1 (KEAP1) differentially regulates nuclear factor erythroid-2-related factors 1 and 2 (NRF1 and NRF2). J. Biol. Chem. 2018, 293, 2029–2040. [Google Scholar] [CrossRef] [Green Version]
- Leinonen, H.M.; Kansanen, E.; Polonen, P.; Heinaniemi, M.; Levonen, A.L. Role of the Keap1-Nrf2 pathway in cancer. Adv. Cancer Res. 2014, 122, 281–320. [Google Scholar] [CrossRef]
- Lee, K.; Kim, S.; Lee, Y.; Lee, H.; Lee, Y.; Park, H.; Nahm, J.H.; Ahn, S.; Yu, S.J.; Lee, K.; et al. The Clinicopathological and Prognostic Significance of Nrf2 and Keap1 Expression in Hepatocellular Carcinoma. Cancers 2020, 12, 2128. [Google Scholar] [CrossRef]
- Raghunath, A.; Sundarraj, K.; Arfuso, F.; Sethi, G.; Perumal, E. Dysregulation of Nrf2 in Hepatocellular Carcinoma: Role in Cancer Progression and Chemoresistance. Cancers 2018, 10, 481. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Liu, X.; Long, M.; Huang, Y.; Zhang, L.; Zhang, R.; Zheng, Y.; Liao, X.; Wang, Y.; Liao, Q.; et al. NRF2 activation by antioxidant antidiabetic agents accelerates tumor metastasis. Sci. Transl. Med. 2016, 8, 334ra351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, L.; Sun, J.; Tan, Y.; Li, Z.; Kong, F.; Shen, Y.; Liu, C.; Chen, L. Prognostic implication of NQO1 overexpression in hepatocellular carcinoma. Hum. Pathol. 2017, 69, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zheng, J.; Wang, M.; Zhang, J.; Tian, T.; Wang, Z.; Yuan, S.; Liu, L.; Zhu, P.; Gu, F.; et al. NQO1 promotes an aggressive phenotype in hepatocellular carcinoma via amplifying ERK-NRF2 signaling. Cancer Sci. 2021, 112, 641–654. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Zhou, C.; Ma, Q.; Chen, W.; Atyah, M.; Yin, Y.; Fu, P.; Liu, S.; Hu, B.; Ren, N.; et al. High GCLC level in tumor tissues is associated with poor prognosis of hepatocellular carcinoma after curative resection. J. Cancer 2019, 10, 3333–3343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perfahl, H.; Jain, H.V.; Joshi, T.; Horger, M.; Malek, N.; Bitzer, M.; Reuss, M. Hybrid Modelling of Transarterial Chemoembolisation Therapies (TACE) for Hepatocellular Carcinoma (HCC). Sci. Rep. 2020, 10, 10571. [Google Scholar] [CrossRef]
- Syu, J.P.; Chi, J.T.; Kung, H.N. Nrf2 is the key to chemotherapy resistance in MCF7 breast cancer cells under hypoxia. Oncotarget 2016, 7, 14659–14672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walcher, L.; Kistenmacher, A.K.; Suo, H.; Kitte, R.; Dluczek, S.; Strauss, A.; Blaudszun, A.R.; Yevsa, T.; Fricke, S.; Kossatz-Boehlert, U. Cancer Stem Cells-Origins and Biomarkers: Perspectives for Targeted Personalized Therapies. Front. Immunol. 2020, 11, 1280. [Google Scholar] [CrossRef]
- Zhou, H.M.; Zhang, J.G.; Zhang, X.; Li, Q. Targeting cancer stem cells for reversing therapy resistance: Mechanism, signaling, and prospective agents. Signal Transduct. Target Ther. 2021, 6, 62. [Google Scholar] [CrossRef]
- Lee, T.K.; Guan, X.Y.; Ma, S. Cancer stem cells in hepatocellular carcinoma—From origin to clinical implications. Nat. Rev. Gastroenterol. Hepatol. 2022, 19, 26–44. [Google Scholar] [CrossRef]
- Guo, Z.; Li, L.Q.; Jiang, J.H.; Ou, C.; Zeng, L.X.; Xiang, B.D. Cancer stem cell markers correlate with early recurrence and survival in hepatocellular carcinoma. World J. Gastroenterol. 2014, 20, 2098–2106. [Google Scholar] [CrossRef]
- Nahm, J.H.; Rhee, H.; Kim, H.; Yoo, J.E.; San Lee, J.; Jeon, Y.; Choi, G.H.; Park, Y.N. Increased expression of stemness markers and altered tumor stroma in hepatocellular carcinoma under TACE-induced hypoxia: A biopsy and resection matched study. Oncotarget 2017, 8, 99359–99371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhee, H.; Nahm, J.H.; Kim, H.; Choi, G.H.; Yoo, J.E.; Lee, H.S.; Koh, M.J.; Park, Y.N. Poor outcome of hepatocellular carcinoma with stemness marker under hypoxia: Resistance to transarterial chemoembolization. Mod. Pathol. 2016, 29, 1038–1049. [Google Scholar] [CrossRef] [PubMed]
- Leung, H.W.; Lau, E.Y.T.; Leung, C.O.N.; Lei, M.M.L.; Mok, E.H.K.; Ma, V.W.S.; Cho, W.C.S.; Ng, I.O.L.; Yun, J.P.; Cai, S.H.; et al. NRF2/SHH signaling cascade promotes tumor-initiating cell lineage and drug resistance in hepatocellular carcinoma. Cancer Lett. 2020, 476, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Morine, Y.; Yamada, S.; Saito, Y.; Ikemoto, T.; Tokuda, K.; Takasu, C.; Miyazaki, K.; Shimada, M. Nrf2 signaling promotes cancer stemness, migration, and expression of ABC transporter genes in sorafenib-resistant hepatocellular carcinoma cells. PLoS ONE 2021, 16, e0256755. [Google Scholar] [CrossRef] [PubMed]
- Kuper, A.; Baumann, J.; Gopelt, K.; Baumann, M.; Sanger, C.; Metzen, E.; Kranz, P.; Brockmeier, U. Overcoming hypoxia-induced resistance of pancreatic and lung tumor cells by disrupting the PERK-NRF2-HIF-axis. Cell Death Dis. 2021, 12, 82. [Google Scholar] [CrossRef] [PubMed]
- Iida, H.; Suzuki, M.; Goitsuka, R.; Ueno, H. Hypoxia induces CD133 expression in human lung cancer cells by up-regulation of OCT3/4 and SOX2. Int. J. Oncol. 2012, 40, 71–79. [Google Scholar] [CrossRef]
- Zhou, C.; Yao, Q.; Zhang, H.; Guo, X.; Liu, J.; Shi, Q.; Huang, S.; Xiong, B. Combining transcatheter arterial embolization with iodized oil containing Apatinib inhibits HCC growth and metastasis. Sci. Rep. 2020, 10, 2964. [Google Scholar] [CrossRef] [Green Version]
- Yu, G.F.; Lin, X.; Luo, R.C.; Fang, W.Y. Nuclear CD133 expression predicts poor prognosis for hepatocellular carcinoma. Int. J. Clin. Exp. Pathol. 2018, 11, 2092–2099. [Google Scholar]
- Zhang, J.; Qi, Y.P.; Ma, N.; Lu, F.; Gong, W.F.; Chen, B.; Ma, L.; Zhong, J.H.; Xiang, B.D.; Li, L.Q. Overexpression of Epcam and CD133 Correlates with Poor Prognosis in Dual-phenotype Hepatocellular Carcinoma. J. Cancer 2020, 11, 3400–3406. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.; Shen, L. Overexpression of NRF2 is correlated with prognoses of patients with malignancies: A meta-analysis. Thorac. Cancer 2017, 8, 558–564. [Google Scholar] [CrossRef]
- Wang, L.; Zhang, C.; Qin, L.; Xu, J.; Li, X.; Wang, W.; Kong, L.; Zhou, T.; Li, X. The prognostic value of NRF2 in solid tumor patients: A meta-analysis. Oncotarget 2018, 9, 1257–1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.; Zhang, C.; Zhang, L.; Yang, Q.; Zhou, S.; Wen, Q.; Wang, J. Nrf2 is a potential prognostic marker and promotes proliferation and invasion in human hepatocellular carcinoma. BMC Cancer 2015, 15, 531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, C.S.; Eom, D.W.; Ahn, Y.; Jang, H.J.; Hwang, S.; Lee, S.G. Can heme oxygenase-1 be a prognostic factor in patients with hepatocellular carcinoma? Medicine 2019, 98, e16084. [Google Scholar] [CrossRef] [PubMed]
- Yeh, C.N.; Wu, R.C.; Cheng, C.T.; Tsai, C.Y.; Chang, Y.R.; Yeh, T.S.; Wu, T.H.; Lee, W.C.; Chiang, K.C. HO-1 is a favorable prognostic factor for HBV-HCC patients who underwent hepatectomy. Cancer Manag. Res. 2018, 10, 6049–6059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goossens-Beumer, I.J.; Zeestraten, E.C.; Benard, A.; Christen, T.; Reimers, M.S.; Keijzer, R.; Sier, C.F.; Liefers, G.J.; Morreau, H.; Putter, H.; et al. Clinical prognostic value of combined analysis of Aldh1, Survivin, and EpCAM expression in colorectal cancer. Br. J. Cancer 2014, 110, 2935–2944. [Google Scholar] [CrossRef] [PubMed]
- Ryu, H.S.; Park, D.J.; Kim, H.H.; Kim, W.H.; Lee, H.S. Combination of epithelial-mesenchymal transition and cancer stem cell-like phenotypes has independent prognostic value in gastric cancer. Hum. Pathol. 2012, 43, 520–528. [Google Scholar] [CrossRef] [PubMed]
- Granito, A.; Facciorusso, A.; Sacco, R.; Bartalena, L.; Mosconi, C.; Cea, U.V.; Cappelli, A.; Antonino, M.; Modestino, F.; Brandi, N.; et al. TRANS-TACE: Prognostic Role of the Transient Hypertransaminasemia after Conventional Chemoembolization for Hepatocellular Carcinoma. J. Pers. Med. 2021, 11, 1041. [Google Scholar] [CrossRef]

{kind=link}
| Gene | Forward (5′→3′) | Reverse (5′→3′) |
|---|---|---|
| NRF2 | AGACGGTATGCAACAGGACA | ACCATGGTAGTCTCAACCAGC |
| NQO1 | TGCAGCGGCTTTGAAGAAGAAAGG | TCGGCAGGATACTGAAAGTTCGCA |
| HO-1 | GCCAGCAACAAAGTGCAAG | GAGTGTAAGGACCCATCGGA |
| GCLC | CTGGGGAGTGATTTCTGCAT | AGGAGGGGGCTTAAATCTCA |
| GCLM | AGTGGGCACAGGTAAAACCA | CTCGTGCGCTTGAATGTCAG |
| EpCAM | CAGAACAATGATGGGCTTTATG | GCAGTCCGCAAACTTTTAC |
| CD133 | TGGATGCAGAACTTGACAACGT | ATACCTGCTACGACAGTCGTGGT |
| TBP | CAGAAGTTGGGTTTTCCAGCTAA | ACATCACAGCTCCCCACCAT |
| Parameters | Value |
|---|---|
| Total cases, n | 120 |
| Age (year, mean, median) | |
| Mean ± SD Median, IQR | 58.24 ± 12.09 58 (52–68) |
| Age (years) | |
| <60 ≥60 | 65 (54.2%) 55 (45.8%) |
| Gender, n (%) | |
| Male Female | 97 (80.8%) 23 (19.2%) |
| Smoking, n (%) a | |
| No Yes | 59 (49.2%) 60 (50.0%) |
| Alcohol consumption, n (%) a | |
| No Yes-low Yes-high | 70 (58.3%) 18 (15.0%) 31 (25.8%) |
| AFP (ng/mL) b | |
| Mean ± SD Median, IQR | 9109.35 ± 50,338.77 34.01 (8.10–733.25) |
| AFP (ng/mL) b | |
| <400 ≥400 | 86 (71.7%) 32 (26.7%) |
| Tumor size (cm) | |
| Mean ± SD Median, IQR | 5.80 ± 4.29 4.15 (2.70–8.45) |
| Size, n (%) | |
| <5 cm ≥5 cm | 69 (57.5%) 51 (42.5%) |
| Edmondson–Steiner (ES) grade, n (%) | |
| Well (I and II) Poor (III and IV) | 79 (65.8%) 41 (34.2%) |
| Number of tumors, n (%) | |
| Solitary Multiple | 70 (58.3%) 50 (41.7%) |
| Vascular invasion, n (%) | |
| Absent Vascular Invasion | 46 (38.3%) 74 (61.7%) |
| Pathology stage, n (%) | |
| Early (I) Late (II, III and IV) | 33 (27.5%) 87 (72.5%) |
| Cirrhosis, n (%) | |
| No Yes | 54 (45.0%) 66 (55.0%) |
| Viral status, n (%) | |
| NBNC HBV HCV HBV + HCV | 9 (7.5%) 77 (64.2%) 26 (21.7%) 8 (6.7%) |
| Metastasis a, n (%) | |
| No Yes | 109 (90.8%) 10 (8.3%) |
| Follow-up duration (months) | |
| Median, IQR | 47.01 (15.08–108.68) |
| Parameters (n) | EpCAM c | p Value | CD133 | p Value | ||
|---|---|---|---|---|---|---|
| High-Expression n, (%) | Low Expression n, (%) | High-Expression n, (%) | Low Expression n, (%) | |||
| Age (years) | 0.001 | 0.367 | ||||
| <60 (65) ≥60 (55) | 35 (55.6%) 13 (24.5%) | 28 (44.4%) 40 (75.5%) | 16 (24.6%) 9 (16.4%) | 49 (75.4%) 46 (83.6%) | ||
| Gender | 0.106 | 0.155 | ||||
| Male (97) Female (23) | 42 (45.2%) 6 (26.1%) | 51 (54.8%) 17 (73.9%) | 23 (23.7%) 2 (8.7%) | 74 (76.3%) 21 (91.3%) | ||
| Smoking, n (%) a | >0.999 | >0.999 | ||||
| No (59) Yes (60) | 23 (41.1%) 24 (40.7%) | 33 (58.9%) 35 (59.3%) | 12 (20.3%) 13 (21.7%) | 47 (79.7%) 47 (78.3%) | ||
| Alcohol consumption, n (%) a | 0.148 | 0.904 | ||||
| No (70) Yes-low (18) Yes-high (31) | 32 (47.8%) 7 (38.9%) 8 (26.7%) | 35 (52.2%) 11 (61.1%) 22 (73.3%) | 15 (21.4%) 3 (16.7%) 7 (22.6%) | 55 (78.6%) 15 (83.3%) 24 (77.4%) | ||
| AFP (ng/mL) b | 0.007 | 0.043 | ||||
| <400 (86) ≥400 (32) | 28 (34.1%) 20 (65.5%) | 54 (65.9%) 12 (37.5%) | 14 (16.3%) 11 (34.4%) | 72 (83.7%) 21 (65.6%) | ||
| Tumor size (cm) | 0.129 | 0.172 | ||||
| <5 cm (69) ≥5 cm (51) | 24 (35.3%) 24 (50.0%) | 44 (64.7%) 24 (50.0%) | 11 (15.9%) 14 (27.5%) | 58 (84.1%) 37 (72.5%) | ||
| ES grade | 0.330 | 0.819 | ||||
| Well (I and II) (79) Poor (III and IV) (41) | 34 (44.7%) 14 (35/0%) | 42 (55.3%) 26 (65.0%) | 17 (21.5%) 8 (19.5%) | 62 (78.5%) 33 (80.5%) | ||
| Number of tumors | 0.036 | 0.013 | ||||
| Solitary (70) Multiple (50) | 22 (32.8%) 26 (53.1%) | 45 (67.2%) 23 (46.9%) | 9 (12.9%) 16 (32.0%) | 61 (87.1%) 34 (68.0%) | ||
| Vascular invasion | 0.449 | 0.039 | ||||
| Absent (46) Vascular invasion (74) | 17 (37.0%) 31 (44.3%) | 29 (63.0%) 39 (55.7%) | 5 (10.9%) 20 (27.0%) | 41 (89.1%) 54 (73.0%) | ||
| Pathology stage | 0.302 | 0.076 | ||||
| Early (I) (33) Late (II, III and IV) (87) | 11 (33.3%) 37 (44.6%) | 22 (66.7%) 46 (55.4%) | 3 (9.1%) 22 (25.3%) | 30 (90.9%) 65 (74.7%) | ||
| Cirrhosis | 0.091 | 0.013 | ||||
| No (54) Yes (66) | 27 (50.0%) 21 (33.9%) | 27 (50.0%) 41 (66.1%) | 17 (31.5%) 8 (12.1%) | 37 (68.5%) 58 (87.9%) | ||
| Viral status | 0.015d | 0.590 | ||||
| NBNC (9) HBV (77) HCV (26) HBV + HCV (8) | 1 (11.1%) 38 (51.4%) 6 (23.1%) 3 (42.9%) | 8 (88.9%) 36 (48.6%) 20 (76.9%) 4 (57.1%) | 2 (22.2%) 17 (22.1%) 6 (23.1%) 0 (0.0%) | 7 (77.8%) 60 (77.9%) 20 (76.9%) 8 (100%) | ||
| Metastasis a | 0.313 | 0.215 | ||||
| No (109) Yes (10) | 41 (39.0%) 6 (60.0%) | 64 (61.0%) 4 (40.0%) | 21 (19.3%) 4 (40.0%) | 88 (80.7%) 6 (60.0%) | ||
| EpCAM b | p Value | CD133 | p Value | |||
|---|---|---|---|---|---|---|
| Low (68) | High (48) | Low (95) | High (25) | |||
| NRF2 (n, %) | 0.294 | 0.126 | ||||
| Low High | 52 (76.5) 16 (23.5) | 32 (66.7) 16 (33.3) | 73 (76.8) 22 (23.2) | 15 (60.0) 10 (40.0) | ||
| NQO1 (n, %) a | 0.011 | 0.047 | ||||
| Low High | 25 (36.8) 43 (63.2) | 7 (14.6) 41 (85.4) | 31 (33.0) 63 (67.0) | 3 (12.0) 22 (88.0) | ||
| HO-1 (n, %) | 0.445 | 0.057 | ||||
| Low High | 59 (86.8) 9 (13.2) | 39 (81.2) 9 (18.8) | 84 (88.4) 11 (11.6) | 18 (72.0) 7 (28.0) | ||
| GCLC (n, %) | 0.330 | 0.636 | ||||
| Low High | 42 (61.8) 26 (38.2) | 34 (70.8) 14 (29.2) | 62 (65.3) 33 (34.7) | 18 (72.0) 7 (28.0) | ||
| GCLM (n, %) | 0.344 | >0.999 | ||||
| Low High | 43 (63.2) 25 (36.8) | 26 (54.2) 22 (45.8) | 55 (57.9) 40 (42.1) | 15 (60.0) 10 (40.0) | ||
| Parameter | Overall Survival | |||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Gender (male/female) | 1.248 (0.714–2.183) | 0.437 | ||
| Age (≥60/<60) | 0.989 (0.643–1.520) | 0.958 | ||
| Smoking (Yes/No) a | 0.986 (0.641–1.516) | 0.947 | ||
| Alcohol consumption a | 1.075 (0.694–1.666) | 0.745 | ||
| No Yes-low Yes-high | 1.00 (Ref) 1.206 (0.654–2.224) 1.008 (0.604–1.681) | 0.549 0.976 | ||
| AFP (ng/mL) (≥400/<400) b | 1.829 (1.147–2.917) | 0.011 | 1.168 (0.701–1.946) | 0.552 |
| Tumor size (≥5 cm/5 cm) | 1.875 (1.221–2.880) | 0.004 | 1.419 (0.840–2.399) | 0.191 |
| ES grade (Poor/Well) | 1.412 (0.897–2.223) | 0.136 | ||
| Number of tumor (Multiple/Solitary) | 1.537 (0.998–2.369) | 0.051 | ||
| Vascular invasion (Yes/No) | 2.161 (1.363–3.426) | 0.001 | 1.821 (1.124–2.9.52) | 0.015 |
| Pathology stage (Late/Early) | 2.018 (1.208–3.370) | 0.007 | 0.965 (0.414–2.245) | 0.934 |
| Cirrhosis (Yes/No) | 0.823 (0.536–1.264) | 0.373 | ||
| Viral status | ||||
| NBNC HBV HCV HBV + HCV | 1.00 (Ref) 0.975 (0.419–2.268) 0.943 (0.376–2.363) 1.692 (0.545–5.256) | 0.952 0.901 0.363 | ||
| Metastasis (Yes/No) a | 2.229 (1.112–4.470) | 0.024 | 2.033 (1.002–4.125) | 0.049 |
| NRF2 (high/low) | 0.695 (0.433–1.117) | 0.133 | ||
| NQO1 (high/low) a | 1.126 (0.674–1.879) | 0.651 | ||
| HO-1 (high/low) | 0.788 (0.456–1.360) | 0.391 | ||
| GCLC (high/low) | 0.832 (0.537–1.290) | 0.412 | ||
| GCLM (high/low) | 0.664 (0.428–1.030) | 0.068 | ||
| EpCAM (high/low) c | 1.108 (0.711–1.726) | 0.652 | ||
| CD133 (high/low) | 2.234 (1.394–3.579) | 0.001 | 2.013 (1.223–3.314) | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tseeleesuren, D.; Hsiao, H.-H.; Kant, R.; Huang, Y.-C.; Tu, H.-P.; Lai, C.-C.; Huang, S.-F.; Yen, C.-H. The Expression and Prognostic Value of Cancer Stem Cell Markers, NRF2, and Its Target Genes in TAE/TACE-Treated Hepatocellular Carcinoma. Medicina 2022, 58, 212. https://doi.org/10.3390/medicina58020212
Tseeleesuren D, Hsiao H-H, Kant R, Huang Y-C, Tu H-P, Lai C-C, Huang S-F, Yen C-H. The Expression and Prognostic Value of Cancer Stem Cell Markers, NRF2, and Its Target Genes in TAE/TACE-Treated Hepatocellular Carcinoma. Medicina. 2022; 58(2):212. https://doi.org/10.3390/medicina58020212
Chicago/Turabian StyleTseeleesuren, Duurenjargal, Hui-Hua Hsiao, Rajni Kant, Yu-Chuen Huang, Hung-Pin Tu, Chih-Chung Lai, Shiu-Feng Huang, and Chia-Hung Yen. 2022. "The Expression and Prognostic Value of Cancer Stem Cell Markers, NRF2, and Its Target Genes in TAE/TACE-Treated Hepatocellular Carcinoma" Medicina 58, no. 2: 212. https://doi.org/10.3390/medicina58020212