
Towards an Accurate Estimation of COVID-19 Cases in Kazakhstan: Back-Casting and Capture–Recapture Approaches

 ,
,  , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Back-Casting Method
2.2. Capture–Recapture Method
2.3. Data
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. WHO Coronavirus (COVID-19) Dashboard. WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/ (accessed on 12 May 2021).
- García-Montero, C.; Fraile-Martínez, O.; Bravo, C.; Torres-Carranza, D.; Sanchez-Trujillo, L.; Gómez-Lahoz, A.M.; Guijarro, L.G.; García-Honduvilla, N.; Asúnsolo, A.; Bujan, J.; et al. An Updated Review of SARS-CoV-2 Vaccines and the Importance of Effective Vaccination Programs in Pandemic Times. Vaccines 2021, 9, 433. [Google Scholar] [CrossRef] [PubMed]
- Gil-Manso, S.; Carbonell, D.; López-Fernández, L.; Miguens, I.; Alonso, R.; Buño, I.; Muñoz, P.; Ochando, J.; Pion, M.; Correa-Rocha, R. Induction of High Levels of Specific Humoral and Cellular Responses to SARS-CoV-2 After the Administration of Covid-19 MRNA Vaccines Requires Several Days. Front. Immunol. 2021, 12, 3970. [Google Scholar] [CrossRef] [PubMed]
- Sharun, K.; Tiwari, R.; Dhama, K.; Emran, T.b.; Rabaan, A.A.; al Mutair, A. Emerging SARS-CoV-2 Variants: Impact on Vaccine Efficacy and Neutralizing Antibodies. Hum. Vaccines Immunother. 2021, 17, 3491–3494. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, L. Implication of SARS-CoV-2 Immune Escape Spike Variants on Secondary and Vaccine Breakthrough Infections. Front. Immunol. 2021, 12, 742167. [Google Scholar] [CrossRef]
- Alene, M.; Yismaw, L.; Assemie, M.A.; Ketema, D.B.; Mengist, B.; Kassie, B.; Birhan, T.Y. Magnitude of Asymptomatic COVID-19 Cases throughout the Course of Infection: A Systematic Review and Meta-Analysis. PLoS ONE 2021, 16, e0249090. [Google Scholar] [CrossRef] [PubMed]
- Hao, X.; Cheng, S.; Wu, D.; Wu, T.; Lin, X.; Wang, C. Reconstruction of the Full Transmission Dynamics of COVID-19 in Wuhan. Nature 2020, 584, 7821. [Google Scholar] [CrossRef]
- Subramanian, R.; He, Q.; Pascual, M. Quantifying Asymptomatic Infection and Transmission of COVID-19 in New York City Using Observed Cases, Serology, and Testing Capacity. Proc. Natl. Acad. Sci. USA 2021, 118, e2019716118. [Google Scholar] [CrossRef]
- Li, R.; Pei, S.; Chen, B.; Song, Y.; Zhang, T.; Yang, W.; Shaman, J. Substantial Undocumented Infection Facilitates the Rapid Dissemination of Novel Coronavirus (SARS-CoV-2). Science 2020, 368, 489–493. [Google Scholar] [CrossRef] [Green Version]
- Pollán, M.; Pérez-Gómez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernán, M.A.; Pérez-Olmeda, M.; Sanmartín, J.L.; Fernández-García, A.; Cruz, I.; Fernández de Larrea, N.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A Nationwide, Population-Based Seroepidemiological Study. Lancet 2020, 396, 535–544. [Google Scholar] [CrossRef]
- Flaxman, S.; Mishra, S.; Gandy, A.; Unwin, H.J.T.; Mellan, T.A.; Coupland, H.; Whittaker, C.; Zhu, H.; Berah, T.; Eaton, J.W.; et al. Estimating the Effects of Non-Pharmaceutical Interventions on COVID-19 in Europe. Nature 2020, 584, 257–261. [Google Scholar] [CrossRef]
- Bragin, D. Bcпoмнить Bce: Xpoнoлoгия Pacпpocтpaнeния Kopoнaвиpyca в Kaзaxcтaнe в 2020 Γoдy. КТК. Available online: https://www.ktk.kz/ru/blog/article/2021/01/02/168297/ (accessed on 12 May 2021).
- Phipps, S.J.; Grafton, R.Q.; Kompas, T. Robust Estimates of the True (Population) Infection Rate for COVID-19: A Backcasting Approach. R. Soc. Open Sci. 2020, 7, 200909. [Google Scholar] [CrossRef] [PubMed]
- Levin, A.T.; Hanage, W.P.; Owusu-Boaitey, N.; Cochran, K.B.; Walsh, S.P.; Meyerowitz-Katz, G. Assessing the Age Specificity of Infection Fatality Rates for COVID-19: Systematic Review, Meta-Analysis, and Public Policy Implications. Eur. J. Epidemiol. 2020, 35, 1123–1138. [Google Scholar] [CrossRef]
- Böhning, D.; Rocchetti, I.; Maruotti, A.; Holling, H. Estimating the Undetected Infections in the Covid-19 Outbreak by Harnessing Capture-Recapture Methods. medRxiv 2020. [Google Scholar] [CrossRef] [PubMed]
- Russell, T.W.; Golding, N.; Hellewell, J.; Abbott, S.; Wright, L.; Pearson, C.A.B.; van Zandvoort, K.; Jarvis, C.I.; Gibbs, H.; Liu, Y.; et al. Reconstructing the Early Global Dynamics of Under-Ascertained COVID-19 Cases and Infections. BMC Med. 2020, 18, 1–9. [Google Scholar] [CrossRef]
- Riou, J.; Hauser, A.; Counotte, M.J.; Althaus, C.L. Adjusted Age-Specific Case Fatality Ratio during the COVID-19 Epidemic in Hubei, China, January and February 2020. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Perkins, T.A.; Cavany, S.M.; Moore, S.M.; Oidtman, R.J.; Lerch, A.; Poterek, M. Estimating Unobserved SARS-CoV-2 Infections in the United States. Proc. Natl. Acad. Sci. USA 2020, 117, 22597–22602. [Google Scholar] [CrossRef] [PubMed]
- Menachemi, N.; Yiannoutsos, C.T.; Dixon, B.E.; Duszynski, T.J.; Fadel, W.F.; Wools-Kaloustian, K.K.; Unruh Needleman, N.; Box, K.; Caine, V.; Norwood, C.; et al. Population Point Prevalence of SARS-CoV-2 Infection Based on a Statewide Random Sample—Indiana, April 25–29, 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 960–964. [Google Scholar] [CrossRef] [PubMed]
- Irons, N.J.; Raftery, A.E. Estimating SARS-CoV-2 Infections from Deaths, Confirmed Cases, Tests, and Random Surveys. Proc. Natl. Acad. Sci. USA 2021, 118, e2103272118. [Google Scholar] [CrossRef] [PubMed]
- Noh, J.; Danuser, G. Estimation of the Fraction of COVID-19 Infected People in U.S. States and Countries Worldwide. PLoS ONE 2021, 16, e0246772. [Google Scholar] [CrossRef] [PubMed]
- Rocchetti, I.; Böhning, D.; Holling, H.; Maruotti, A. Estimating the Size of Undetected Cases of the COVID-19 Outbreak in Europe: An Upper Bound Estimator. Epidemiol. Methods 2020, 9. [Google Scholar] [CrossRef]
- Nishiura, H.; Kobayashi, T.; Miyama, T.; Suzuki, A.; Jung, S.m.; Hayashi, K.; Kinoshita, R.; Yang, Y.; Yuan, B.; Akhmetzhanov, A.R.; et al. Estimation of the Asymptomatic Ratio of Novel Coronavirus Infections (COVID-19). Int. J. Infect. Dis. 2020, 94, 154. [Google Scholar] [CrossRef]
- Johansson, M.A.; Quandelacy, T.M.; Kada, S.; Prasad, P.V.; Steele, M.; Brooks, J.T.; Slayton, R.B.; Biggerstaff, M.; Butler, J.C. SARS-CoV-2 Transmission from People without COVID-19 Symptoms. JAMA Netw. Open 2021, 4, 2035057. [Google Scholar] [CrossRef] [PubMed]
- Kazinform. The Epidemiological Situation with Coronavirus Infection in the Country. Available online: https://www.coronavirus2020.kz (accessed on 5 May 2021).
- Ibrahim, N.K. Epidemiologic Surveillance for Controlling Covid-19 Pandemic: Types, Challenges and Implications. J. Infect. Public Health 2020, 13, 1630–1638. [Google Scholar] [CrossRef] [PubMed]
- Ioannidis, J.P.A. Over- and under-Estimation of COVID-19 Deaths. Eur. J. Epidemiol. 2021, 36, 581. [Google Scholar] [CrossRef] [PubMed]
- Kung, S.; Doppen, M.; Black, M.; Braithwaite, I.; Kearns, C.; Weatherall, M.; Beasley, R.; Kearns, N. Underestimation of COVID-19 Mortality during the Pandemic. ERJ Open Res. 2021, 7, 00766–02020. [Google Scholar] [CrossRef] [PubMed]
- Sze, S.; Pan, D.; Nevill, C.R.; Gray, L.J.; Martin, C.A.; Nazareth, J.; Minhas, J.S.; Divall, P.; Khunti, K.; Abrams, K.R.; et al. Ethnicity and Clinical Outcomes in COVID-19: A Systematic Review and Meta-Analysis. EClinicalMedicine 2020, 29, 100630. [Google Scholar] [CrossRef] [PubMed]
- Yegorov, S.; Goremykina, M.; Ivanova, R.; Good, S.v.; Babenko, D.; Shevtsov, A.; MacDonald, K.S.; Zhunussov, Y. Epidemiology, Clinical Characteristics, and Virologic Features of COVID-19 Patients in Kazakhstan: A Nation-wide retro-spective cohort study. Lancet Reg. Health-Eur. 2021, 4, 100096. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
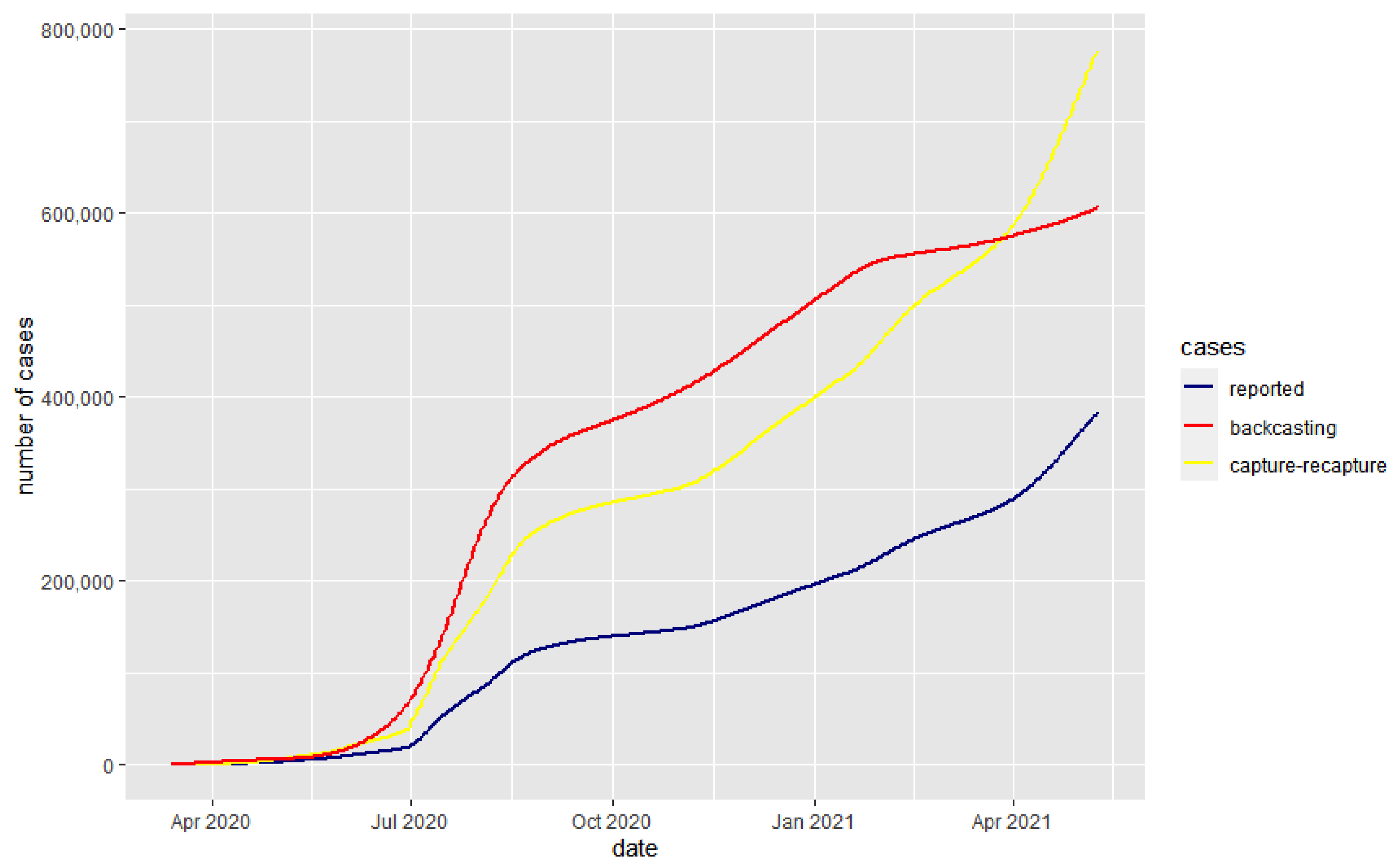
| Date (d/m/y) | Reported Cases | Capture–Recapture | Back-Casting |
|---|---|---|---|
| 1 July 2020 | 20,743 | 47,005 | 83,491 |
| 1 October 2020 | 139,337 | 285,255 | 427,513 |
| 1 January 2021 | 196,471 | 400,647 | 576,962 |
| 1 February 2021 | 227,830 | 464,231 | 626,175 |
| 1 March 2021 | 258,254 | 524,604 | 638,869 |
| 1 April 2021 | 289,046 | 586,851 | 651,518 |
| 1 May 2021 | 359,887 | 729,996 | 674,266 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarría-Santamera, A.; Abdukadyrov, N.; Glushkova, N.; Russell Peck, D.; Colet, P.; Yeskendir, A.; Asúnsolo, A.; Ortega, M.A. Towards an Accurate Estimation of COVID-19 Cases in Kazakhstan: Back-Casting and Capture–Recapture Approaches. Medicina 2022, 58, 253. https://doi.org/10.3390/medicina58020253
Sarría-Santamera A, Abdukadyrov N, Glushkova N, Russell Peck D, Colet P, Yeskendir A, Asúnsolo A, Ortega MA. Towards an Accurate Estimation of COVID-19 Cases in Kazakhstan: Back-Casting and Capture–Recapture Approaches. Medicina. 2022; 58(2):253. https://doi.org/10.3390/medicina58020253
Chicago/Turabian StyleSarría-Santamera, Antonio, Nurlan Abdukadyrov, Natalya Glushkova, David Russell Peck, Paolo Colet, Alua Yeskendir, Angel Asúnsolo, and Miguel A. Ortega. 2022. "Towards an Accurate Estimation of COVID-19 Cases in Kazakhstan: Back-Casting and Capture–Recapture Approaches" Medicina 58, no. 2: 253. https://doi.org/10.3390/medicina58020253
APA StyleSarría-Santamera, A., Abdukadyrov, N., Glushkova, N., Russell Peck, D., Colet, P., Yeskendir, A., Asúnsolo, A., & Ortega, M. A. (2022). Towards an Accurate Estimation of COVID-19 Cases in Kazakhstan: Back-Casting and Capture–Recapture Approaches. Medicina, 58(2), 253. https://doi.org/10.3390/medicina58020253