
Highlighting the Benefits of Rehabilitation Treatments in Hip Osteoarthritis

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
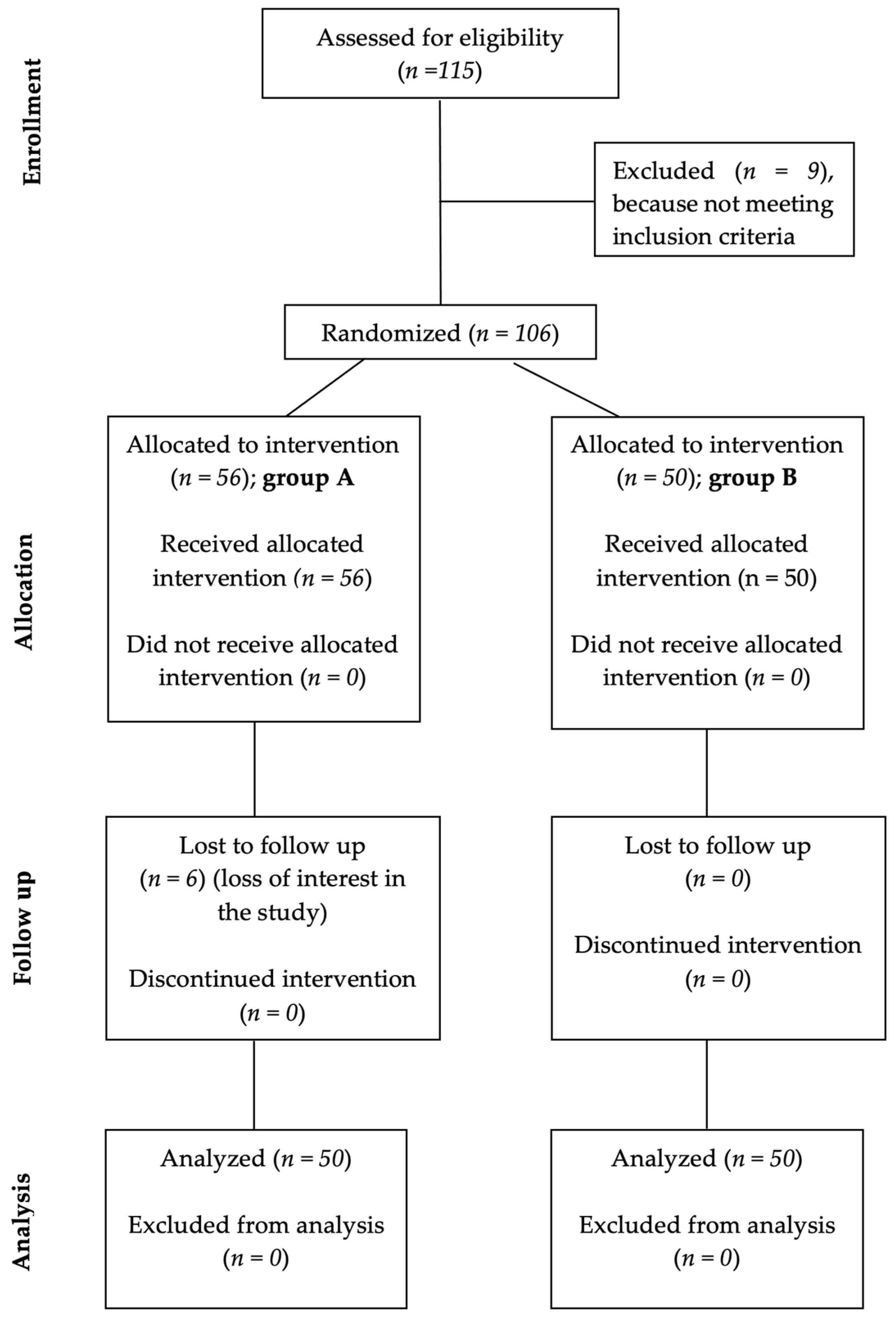
2.1. Study Design and Patients’ Selection
- group A—the study group, 50 subjects treated with DT (NSAIDs,) and RT;
- group B—the control group, 50 subjects treated only with DT (NSAIDs), according to their specific symptomatology.
2.2. Lequesne Hip Index and Tinetti Test
2.3. Statistical Analyses
- ES < 0.2—minor change;
- ES between 0.2–0.49—small change;
- ES between 0.5–0.79—moderate change and
- ES > 0.8—major change.
3. Results
- females are predominated in both groups, (1.17:1—group A vs. 1.27:1—group B);
- most cases (52.00%—group A vs. 50.00%—group B) were between the ages of 51–60;
- most subjects in both groups were from urban areas, and
- in terms of hip OA staging, most subjects in both groups were classified with grade 1.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lespasio, M.J.; Sultan, A.A.; Piuzzi, N.S.; Khlopas, A.; Husni, M.E.; Muschler, G.F.; Mont, M.A. Hip Osteoarthritis: A Primer. Perm. J. 2018, 22, 17–084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganz, R.; Leunig, M.; Leunig-Ganz, K.; Harris, W.H. The etiology of osteoarthritis of the hip: An integrated mechanical concept. Clin. Orthop. Relat. Res. 2008, 466, 264–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordan, J.M.; Helmick, C.G.; Renner, J.B.; Luta, G.; Dragomir, A.D.; Woodard, J.; Fang, F.; Schwartz, T.A.; Nelson, A.E.; Abbate, L.M.; et al. Prevalence of hip symptoms and radiographic and symptomatic hip osteoarthritis in African-Americans and Caucasians: The Johnston County Osteoarthritis Project. J. Rheumatol. 2009, 36, 809–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radu, A.F.; Bungau, S.G. Management of Rheumatoid Arthritis: An Overview. Cells 2021, 10, 2857. [Google Scholar] [CrossRef] [PubMed]
- Hochberg, M.C.; Altman, R.D.; April, K.T.; Benkhalti, M.; Guyatt, G.; McGowan, J.; Towheed, T.; Welch, V.; Wells, G.; Tugwell, P. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 2012, 64, 465–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovalenko, B.; Bremjit, P.; Fernando, N. Classifications in Brief: Tönnis Classification of Hip Osteoarthritis. Clin. Orthop. Relat. Res. 2018, 476, 1680–1684. [Google Scholar] [CrossRef]
- Poulsen, E.; Christensen, H.W.; Roos, E.M.; Vach, W.; Overgaard, S.; Hartvigsen, J. Non-surgical treatment of hip osteoarthritis. Hip school, with or without the addition of manual therapy, in comparison to a minimal control intervention: Protocol for a three-armed randomized clinical trial. BMC Musculoskelet. Disord. 2011, 12, 88. [Google Scholar] [CrossRef] [Green Version]
- Sulsky, S.I.; Carlton, L.; Bochmann, F.; Ellegast, R.; Glitsch, U.; Hartmann, B.; Pallapies, D.; Seidel, D.; Sun, Y. Epidemiological Evidence for Work Load as a Risk Factor for Osteoarthritis of the Hip: A Systematic Review. PLoS ONE 2012, 7, e31521. [Google Scholar] [CrossRef] [Green Version]
- Magni, A.; Agostoni Centro Cardiologico Monzino, P.; Carlo Parea, V.; Agostoni, I.P.; Bonezzi, C.; Massazza, G.; Menè, P.; Savarino, V.; Fornasari, D. Management of Osteoarthritis: Expert Opinion on NSAIDs. Pain Ther. 2021, 10, 783–808. [Google Scholar] [CrossRef]
- Pelletier, J.P.; Martel-Pelletier, J.; Rannou, F.; Cooper, C. Efficacy and safety of oral NSAIDs and analgesics in the management of osteoarthritis: Evidence from real-life setting trials and surveys. Semin. Arthritis Rheum. 2016, 45, S22–S27. [Google Scholar] [CrossRef] [Green Version]
- Capel, M.; Tornero, J.; Zamorano, J.L.; Oyagüez, I.; Casado, M.Á.; Sánchez-Covisa, J.; Lanas, Á. Eficiencia de la combinación naproxeno/esomeprazol para el tratamiento de la artrosis en España. Reumatol. Clínica 2014, 10, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Van Soest, E.M.; Valkhoff, V.E.; Mazzaglia, G.; Schade, R.; Molokhia, M.; Goldstein, J.L.; Hernández-Díaz, S.; Trifirò, G.; Dieleman, J.P.; Kuipers, E.J.; et al. Suboptimal gastroprotective coverage of NSAID use and the risk of upper gastrointestinal bleeding and ulcers: An observational study using three European databases. Gut 2011, 60, 1650–1659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miner, P.; Plachetka, J.; Orlemans, E.; Fort, J.G.; Sostek, M. Clinical trial: Evaluation of gastric acid suppression with three doses of immediate-release esomeprazole in the fixed-dose combination of PN 400 (naproxen/esomeprazole magnesium) compared with naproxen 500 mg and enteric-coated esomeprazole 20 mg: A randomized, open-label, Phase I study in healthy volunteers. Aliment. Pharmacol. Ther. 2010, 32, 414–424. [Google Scholar] [CrossRef] [PubMed]
- Tit, D.M.; Bungau, S.; Iovan, C.; Cseppento, D.C.N.; Endres, L.; Sava, C.; Sabau, A.M.; Furau, G.; Furau, C. Effects of the Hormone Replacement Therapy and of Soy Isoflavones on Bone Resorption in Postmenopause. J. Clin. Med. 2018, 7, 297. [Google Scholar] [CrossRef] [Green Version]
- McNair, P.J.; Simmonds, M.A.; Boocock, M.G.; Larmer, P.J. Exercise therapy for the management of osteoarthritis of the hip joint: A systematic review. Arthritis Res. Ther. 2009, 11, R98. [Google Scholar] [CrossRef] [Green Version]
- Moldovan, E.; Mindrescu, V. Kinesitherapy Intervention in Improving Degenerative Rheumatic Disorders of Hips Coxarthrosis. Sch. Bull. 2019, 5, 767–774. [Google Scholar] [CrossRef]
- Svege, I.; Nordsletten, L.; Fernandes, L.; Risberg, M.A. Exercise therapy may postpone total hip replacement surgery in patients with hip osteoarthritis: A long-term follow-up of a randomised trial. Ann. Rheum. Dis. 2015, 74, 164–169. [Google Scholar] [CrossRef] [Green Version]
- Abbott, J.H.; Robertson, M.C.; Chapple, C.; Pinto, D.; Wright, A.A.; Leon de la Barra, S.; Baxter, G.D.; Theis, J.C.; Campbell, A.J. Manual therapy, exercise therapy, or both, in addition to usual care, for osteoarthritis of the hip or knee: A randomized controlled trial. 1: Clinical effectiveness. Osteoarthr. Cartil. 2013, 21, 525–534. [Google Scholar] [CrossRef] [Green Version]
- Uusi-Rasi, K.; Patil, R.; Karinkanta, S.; Tokola, K.; Kannus, P.; Sievänen, H. Exercise Training in Treatment and Rehabilitation of Hip Osteoarthritis: A 12-Week Pilot Trial. J. Osteoporos. 2017, 2017, 3905492. [Google Scholar] [CrossRef]
- Poquet, N.; Williams, M.; Bennell, K.L. Exercise for Osteoarthritis of the Hip. Phys. Ther. 2016, 96, 1689–1694. [Google Scholar] [CrossRef]
- Teo, P.L.; Hinman, R.S.; Egerton, T.; Dziedzic, K.S.; Bennell, K.L. Identifying and Prioritizing Clinical Guideline Recommendations Most Relevant to Physical Therapy Practice for Hip and/or Knee Osteoarthritis. J. Orthop. Sports Phys. Ther. 2019, 49, 501–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Doormaal, M.C.M.; Meerhoff, G.A.; Vliet Vlieland, T.P.M.; Peter, W.F. A clinical practice guideline for physical therapy in patients with hip or knee osteoarthritis. Musculoskelet. Care 2020, 18, 575–595. [Google Scholar] [CrossRef] [PubMed]
- Cibulka, M.T.; Bloom, N.J.; Enseki, K.R.; Macdonald, C.W.; Woehrle, J.; McDonough, C.M. Hip Pain and Mobility Deficits-Hip Osteoarthritis: Revision 2017. J. Orthop. Sports Phys. Ther. 2017, 47, A1–A37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacDonald, C.W.; Whitman, J.M.; Cleland, J.A.; Smith, M.; Hoeksma, H.L. Clinical Outcomes Following Manual Physical Therapy and Exercise for Hip Osteoarthritis: A Case Series. J. Orthop. Sports Phys. Ther. 2006, 36, 588–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernández-Molina, G.; Reichenbach, S.; Bin, Z.; Lavalley, M.; Felson, D.T. Effect of therapeutic exercise for hip osteoarthritis pain: Results of a meta-analysis. Arthritis Rheum. 2008, 59, 1221–1228. [Google Scholar] [CrossRef] [Green Version]
- Kawa, M.; Kowza-Dzwonkowska, M.; Schenk, A. The role of physical activity in supporting treatment of coxarthrosis symptoms in elderly patients. Balt. J. Health Phys. Act. 2016, 8, 41–48. [Google Scholar] [CrossRef]
- Fendrick, A.M.; Greenberg, B.P. A review of the benefits and risks of nonsteroidal anti-inflammatory drugs in the management of mild-to-moderate osteoarthritis. Osteopath. Med. Prim. Care 2009, 3, 1. [Google Scholar] [CrossRef] [Green Version]
- WMA Declaration of Helsinki-Ethical Principles for Medical Research Involving Human Subjects. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 23 February 2022).
- Hamre, H.J.; Glockmann, A.; Kienle, G.S.; Kiene, H. Combined bias suppression in single-arm therapy studies. J. Eval. Clin. Pract. 2008, 14, 923–929. [Google Scholar] [CrossRef] [Green Version]
- Grässel, S.; Muschter, D. Recent advances in the treatment of osteoarthritis. F1000Research 2020, 9, 325. [Google Scholar] [CrossRef]
- Lequesne, M.G. The algofunctional indices for hip and knee osteoarthritis-PubMed. J. Rheumatol. 1997, 24, 779–781. [Google Scholar]
- Lequesne, M.G.; Mery, C.; Samson, M.; Gerard, P. Indexes of severity for osteoarthritis of the hip and knee. Validation--value in comparison with other assessment tests. Scand. J. Rheumatol. 1987, 65, 85–89. [Google Scholar] [CrossRef]
- Lequesne, M. Indices of severity and disease activity for osteoarthritis. Semin. Arthritis Rheum. 1991, 20, 48–54. [Google Scholar] [CrossRef]
- Tinetti, M.E. Performance-oriented assessment of mobility problems in elderly patients. J. Am. Geriatr. Soc. 1986, 34, 119–126. [Google Scholar] [CrossRef]
- Wilson, J.J.; Furukawa, M. Evaluation of the Patient with Hip Pain-American Family Physician. Am. Fam. Physician 2014, 89, 27–34. [Google Scholar]
- Fransen, M.; Mcconnell, S.; Hernandez-Molina, G.; Reichenbach, S. Exercise for osteoarthritis of the hip. Cochrane Database Syst. Rev. 2014, 4, CD007912. [Google Scholar] [CrossRef] [Green Version]
- Murphy, S.L.; Robinson-Lane, S.G.; Niemiec, S.L.S. Knee and Hip Osteoarthritis Management: A Review of Current and Emerging Non-Pharmacological Approaches. Curr. Treat. Options Rheumatol. 2016, 2, 296–311. [Google Scholar] [CrossRef] [Green Version]
- Kopke, S.; Meyer, G. The Tinetti test. Z Gerontol Geriatr 2006, 39, 288–291. [Google Scholar] [CrossRef]
- Musumeci, G.; Aiello, F.C.; Szychlinska, M.A.; Di Rosa, M.; Castrogiovanni, P.; Mobasheri, A. Osteoarthritis in the XXIst Century: Risk Factors and Behaviours that Influence Disease Onset and Progression. Int. J. Mol. Sci. 2015, 16, 6093–6112. [Google Scholar] [CrossRef]
- Macovei, L.; Brujbu, I.; Murariu, R.V. Coxarthrosis--disease of multifactorial etiology methods of prevention and treatment. The role of kinesitherapy in coxarthrosis. Rev. Med. Chir. Soc. Med. Nat. Iasi 2013, 117, 351–357. [Google Scholar]
- Coggon, D.; Kellingray, S.; Inskip, H.; Croft, P.; Campbell, L.; Cooper, C. Osteoarthritis of the Hip and Occupational Lifting. Am. J. Epidemiol. 1998, 147, 523–528. [Google Scholar] [CrossRef] [Green Version]
- Becheva, M.; Petrova, G.; Kirkova, A.; Atanasov, P. Kinesitherapeutic behaviour in conservative treatment of coxarthrosis-case report. Pharmacia 2019, 66, 75–77. [Google Scholar] [CrossRef]
- Jotanovic, Z.; Mihelic, R.; Gulan, G.; Sestan, B.; Dembic, Z. Osteoarthritis of the hip: An overview. Period. Biol. 2015, 57, 95–108. [Google Scholar]
- Jankowski, D.; Kuryliszyn-Moskal, A. Assessment of the impact of the rehabilitation procedure on functional and clinical condition of patients with coxarthrosis. Reumatologia 2014, 52, 57–61. [Google Scholar] [CrossRef]
- Divjak, A.; Aleksic, D.; Ilic, K. Impact of Rehabilitation on Health Related Quality of Life in Patients with Hip Osteoarthritis. Ser. J. Exp. Clin. Res. 2017, 18, 139–144. [Google Scholar] [CrossRef] [Green Version]
- Kasnakova, P.; Ivanova, S.; Ivanov, K.; Petkova-Gueorguieva, E.; Gueorguiev, S.; Madzharov, V.; Mihaylova, A.; Petleshkova, P. Conservative therapy options for the treatment of coxarthrosis in the early stage of the condition. Biomed. Res. 2018, 29, 2997–3001. [Google Scholar] [CrossRef] [Green Version]
- Giemza, C.; Ostrowska, B.; Matczak-Giemza, M. The effect of physiotherapy training programme on postural stability in men with hip osteoarthritis. Aging Male 2007, 10, 67–70. [Google Scholar] [CrossRef]
- Jahantabi-Nejad, S.; Azad, A. Predictive accuracy of performance oriented mobility assessment for falls in older adults: A systematic review. Med. J. Islam. Repub. Iran 2019, 33, 38. [Google Scholar] [CrossRef]
- Ly, T.V.; Swiontkowski, M.F. Management of femoral neck fractures in young adults. Indian J. Orthop. 2008, 42, 3–12. [Google Scholar] [CrossRef]
- Cibulka, M.T.; White, D.M.; Woehrle, J.; Harris-Hayes, M.; Enseki, K.; Fagerson, T.L.; Slover, J.; Godges, J.J. Hip Pain and Mobility Deficits–Hip Osteoarthritis. J. Orthop. Sports Phys. Ther. 2009, 39, A1–A25. [Google Scholar] [CrossRef] [Green Version]
- Bennell, K.L.; Egerton, T.; Martin, J.; Abbott, J.H.; Metcalf, B.; McManus, F.; Sims, K.; Pua, Y.H.; Wrigley, T.V.; Forbes, A.; et al. Effect of physical therapy on pain and function in patients with hip osteoarthritis: A randomized clinical trial. JAMA 2014, 311, 1987–1997. [Google Scholar] [CrossRef]
- Carr, A. Barriers to the effectiveness of any intervention in OA. Best Pract. Res. Clin. Rheumatol. 2001, 15, 645–656. [Google Scholar] [CrossRef]
- Aresti, N.; Kassam, J.; Nicholas, N.; Achan, P. Hip osteoarthritis. BMJ 2016, 354, i3405. [Google Scholar] [CrossRef]
- Ryan, D.H.; Yockey, S.R. Weight Loss and Improvement in Comorbidity: Differences at 5%, 10%, 15%, and Over. Curr. Obes. Rep. 2017, 6, 187–194. [Google Scholar] [CrossRef]
- Booth, F.W.; Roberts, C.K.; Thyfault, J.P.; Ruegsegger, G.N.; Toedebusch, R.G. Role of Inactivity in Chronic Diseases: Evolutionary Insight and Pathophysiological Mechanisms. Physiol. Rev. 2017, 97, 1351–1402. [Google Scholar] [CrossRef]
- Swift, D.L.; Johannsen, N.M.; Lavie, C.J.; Earnest, C.P.; Church, T.S. The role of exercise and physical activity in weight loss and maintenance. Prog. Cardiovasc. Dis. 2014, 56, 441–447. [Google Scholar] [CrossRef] [Green Version]
- Bennell, K. Physiotherapy management of hip osteoarthritis. J. Physiother. 2013, 59, 145–157. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups’ Characteristics | a.v. ± St. Dev. % | p | |
|---|---|---|---|
| Age (years) | A | 55.92 ± 6.63 | 0.083 |
| B | 57.28 ± 5.32 | ||
| Gender: F/M | A | 54/46 | 0.842 |
| B | 56/44 | ||
| Environmental origin: U/R | A | 70/30 | 0.501 |
| B | 68/32 | ||
| Diagnosis: hip OA grd. 1/grd 2 | A | 70/30 | 0.830 |
| B | 68/32 | ||
| BMI (kg/m2) | A | 29.40 ± 4.05 | 0.900 |
| B | 29.30 ± 3.86 | ||
| Studied Parameters | Group A | Group B | p |
|---|---|---|---|
| LHI | 6.70 ± 1.02 | 6.80 ± 0.86 | 0.596 |
| TT | 20.70 ± 1.18 | 19.84 ± 1.52 | 0.200 |
| FH | 58.40 ± 5.75 | 58.60 ± 5.29 | 0.107 |
| AH | 27.80 ± 2.70 | 27.40 ± 3.19 | 0.150 |
| Modifiable Parameters | T0 | T1 | p | ES | |
|---|---|---|---|---|---|
| LHI | A | 6.70 ± 1.02 | 5.92 ± 1.03 | 0.023 | 0.764 |
| B | 6.80 ± 0.86 | 6.96 ± 1.49 | 0.650 | 0.131 | |
| TT | A | 20.70 ± 1.18 | 21.78 ± 3.34 | 0.011 | 0.431 |
| B | 19.84 ± 1.52 | 18.52 ± 3.64 | <0.001 | 0.473 | |
| FH | A | 58.40 ± 5.75 | 67.20 ± 5.29 | 0.001 | 1.592 |
| B | 58.60 ± 5.29 | 56.80 ± 6.76 | 0.025 | 0.296 | |
| AH | A | 27.80 ± 2.70 | 31.80 ± 4.38 | 0.001 | 1.099 |
| B | 27.40 ± 3.19 | 25.80 ± 4.38 | <0.001 | 0.417 | |
| BMI | A | 29.40 ± 4.05 | 28.30 ± 3.41 | 0.223 | 0.293 |
| B | 29.30 ± 3.86 | 29.80 ± 3.75 | 0.513 | 0.131 | |
| Groups’ Characteristics | a.v. ± St. Dev. % | p | |
|---|---|---|---|
| Gender: Female/Male | 41–50 | 57/43 | 0.594 |
| 51–60 | 50/50 | ||
| 61–70 | 62/38 | ||
| Environmental origin: Urban/Rural | 41–50 | 57/43 | 0.852 |
| 51–60 | 65/43 | ||
| 61–70 | 62/38 | ||
| Diagnosis: hip OA grd. 1/grd. 2 | 41–50 | 69/31 | 0.876 |
| 51–60 | 70/31 | ||
| 61–70 | 44/56 | ||
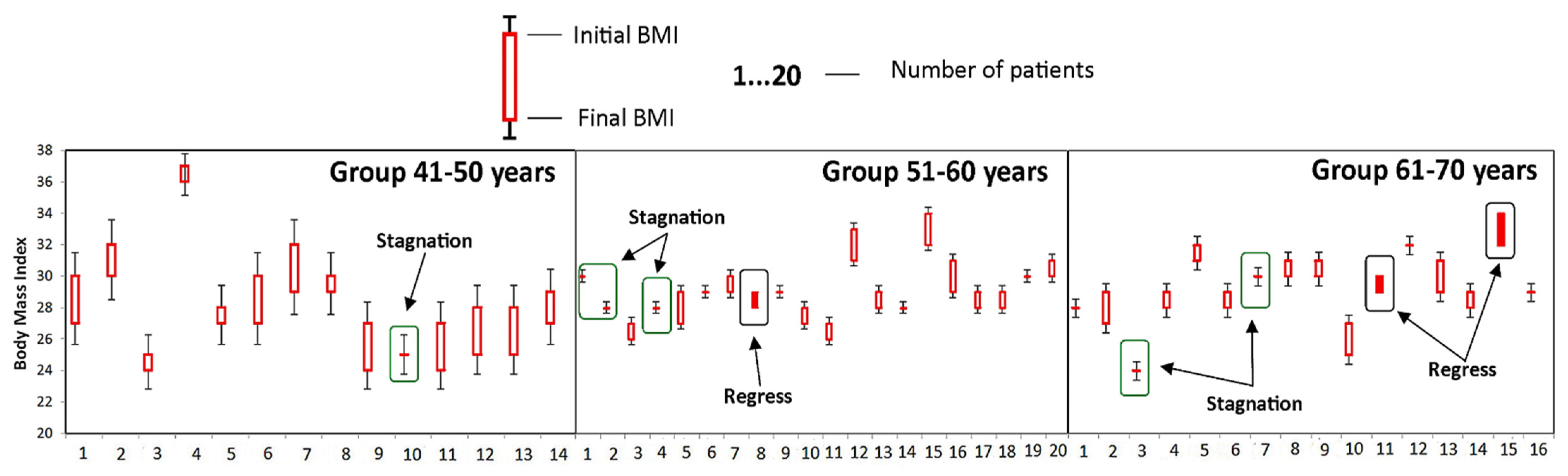
| Body mass index (kg/m2) | 41–50 | 29.07 ± 2.95 | 0.355 |
| 51–60 | 29.35 ± 1.81 | ||
| 61–70 | 29.50 ± 2.10 | ||
| Age (Years) | T0 | T1 | p | ES |
|---|---|---|---|---|
| BMI | ||||
| 41–50 | 29.07 ± 2.95 | 27.07 ± 3.25 | 0.100 | 0.644 |
| 51–60 | 29.35 ± 1.81 | 28.60 ± 1.54 | 0.167 | 0.466 |
| 61–70 | 29.50 ± 2.10 | 28.94 ± 2.46 | 0.492 | 0.244 |
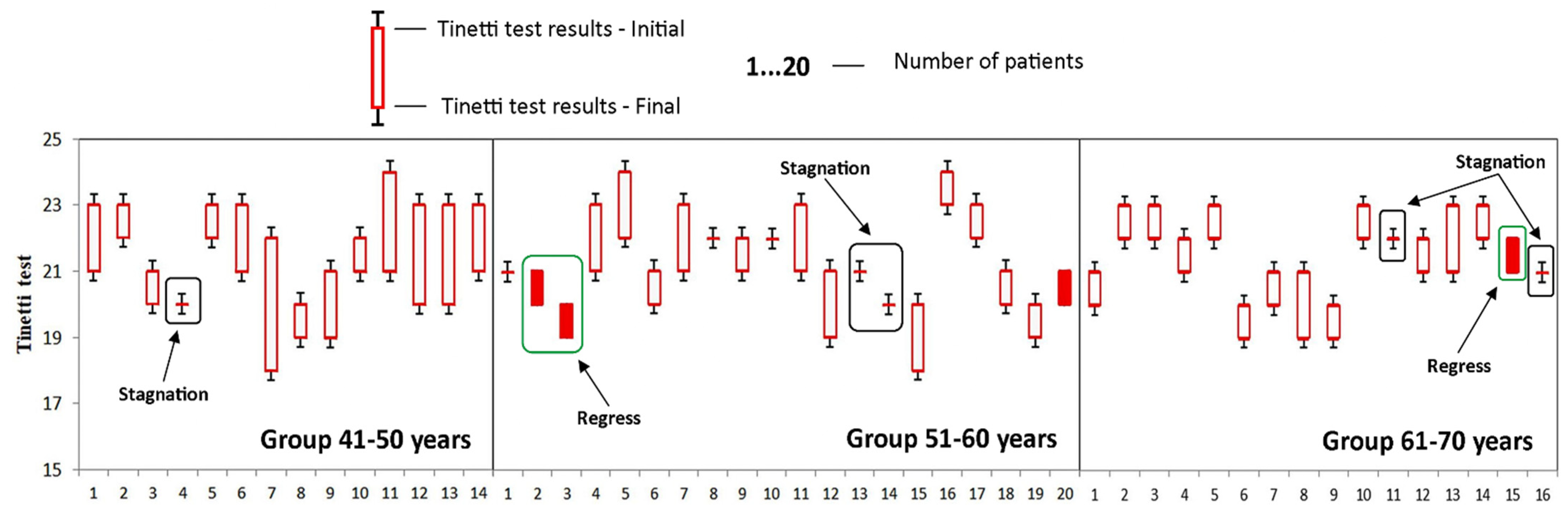
| TT | ||||
| 41–50 | 20.36 ± 1.15 | 22.21 ± 1.25 | 0.001 | 1.540 |
| 51–60 | 20.75 ± 1.21 | 21.50 ± 1.47 | 0.086 | 0.557 |
| 61–70 | 20.94 ± 1.18 | 21.81 ± 1.11 | 0.039 | 0.759 |
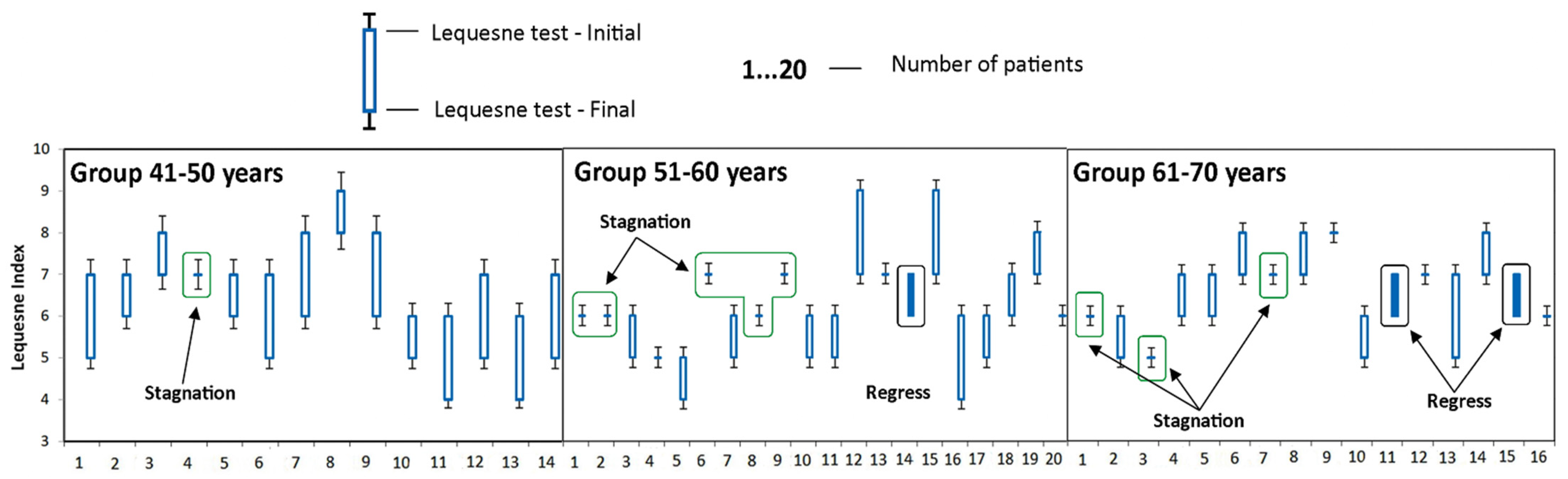
| LHI | ||||
| 41–50 | 7.14 ± 0.86 | 5.64 ± 1.15 | 0.001 | 1.477 |
| 51–60 | 6.50 ± 1.10 | 5.85 ± 1.04 | 0.062 | 0.607 |
| 61–70 | 6.75 ± 0.93 | 6.31 ± 0.95 | 0.197 | 0.468 |
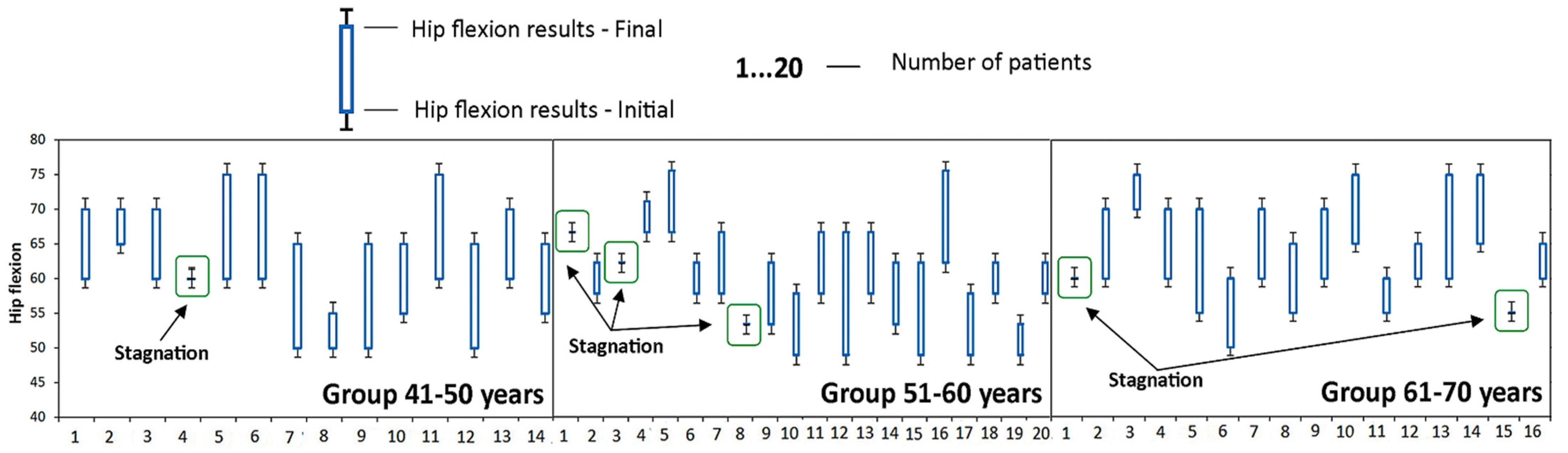
| FH | ||||
| 41–50 | 56.79 ± 5.04 | 67.50 ± 5.80 | < 0.001 | 1.971 |
| 51–60 | 58.75 ± 6.86 | 66.75 ± 6.74 | 0.001 | 1.176 |
| 61–69 | 59.38 ± 4.79 | 67.50 ± 6.32 | 0.001 | 1.448 |
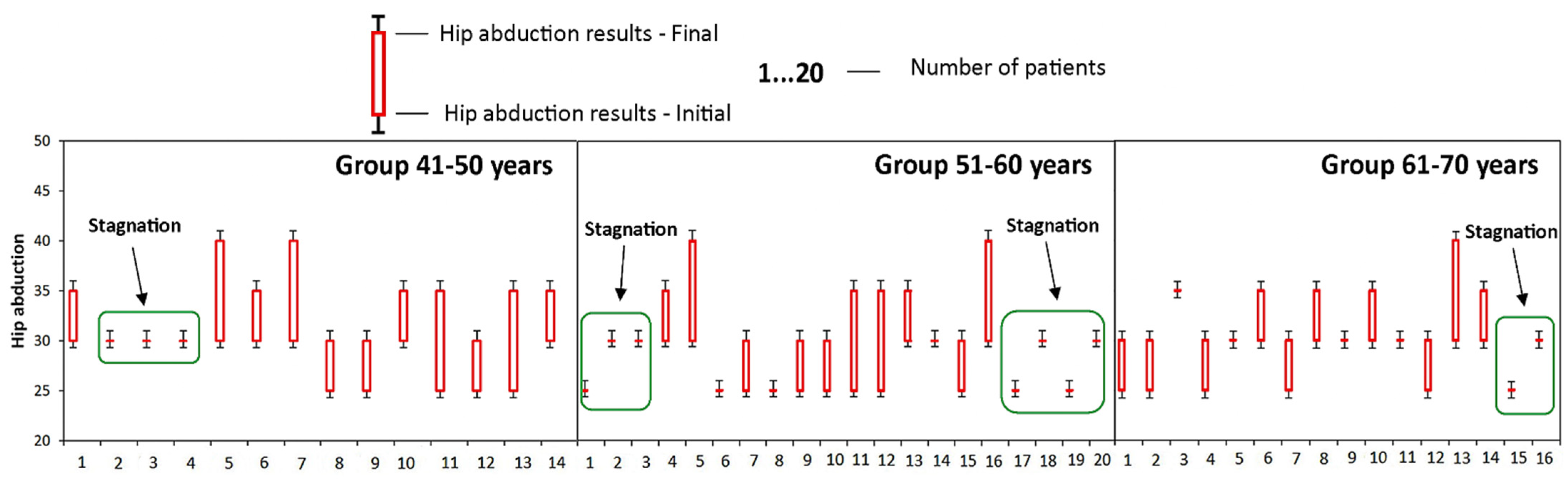
| AH | ||||
| 41–50 | 27.86 ± 2.57 | 33.57 ± 3.63 | 0.001 | 1.815 |
| 51–60 | 27.25 ± 2.55 | 30.75 ± 4.67 | 0.006 | 0.930 |
| 61–69 | 28.44 ± 3.01 | 31.88 ± 3.59 | 0.006 | 1.038 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radu, A.-F.; Bungau, S.G.; Tit, D.M.; Behl, T.; Uivaraseanu, B.; Marcu, M.F. Highlighting the Benefits of Rehabilitation Treatments in Hip Osteoarthritis. Medicina 2022, 58, 494. https://doi.org/10.3390/medicina58040494
Radu A-F, Bungau SG, Tit DM, Behl T, Uivaraseanu B, Marcu MF. Highlighting the Benefits of Rehabilitation Treatments in Hip Osteoarthritis. Medicina. 2022; 58(4):494. https://doi.org/10.3390/medicina58040494
Chicago/Turabian StyleRadu, Andrei-Flavius, Simona Gabriela Bungau, Delia Mirela Tit, Tapan Behl, Bogdan Uivaraseanu, and Mihai Florin Marcu. 2022. "Highlighting the Benefits of Rehabilitation Treatments in Hip Osteoarthritis" Medicina 58, no. 4: 494. https://doi.org/10.3390/medicina58040494