
A Spontaneous Extracranial Internal Carotid Artery Dissection with Autosomal Dominant Polycystic Kidney Disease: A Case Report and Literature Review

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
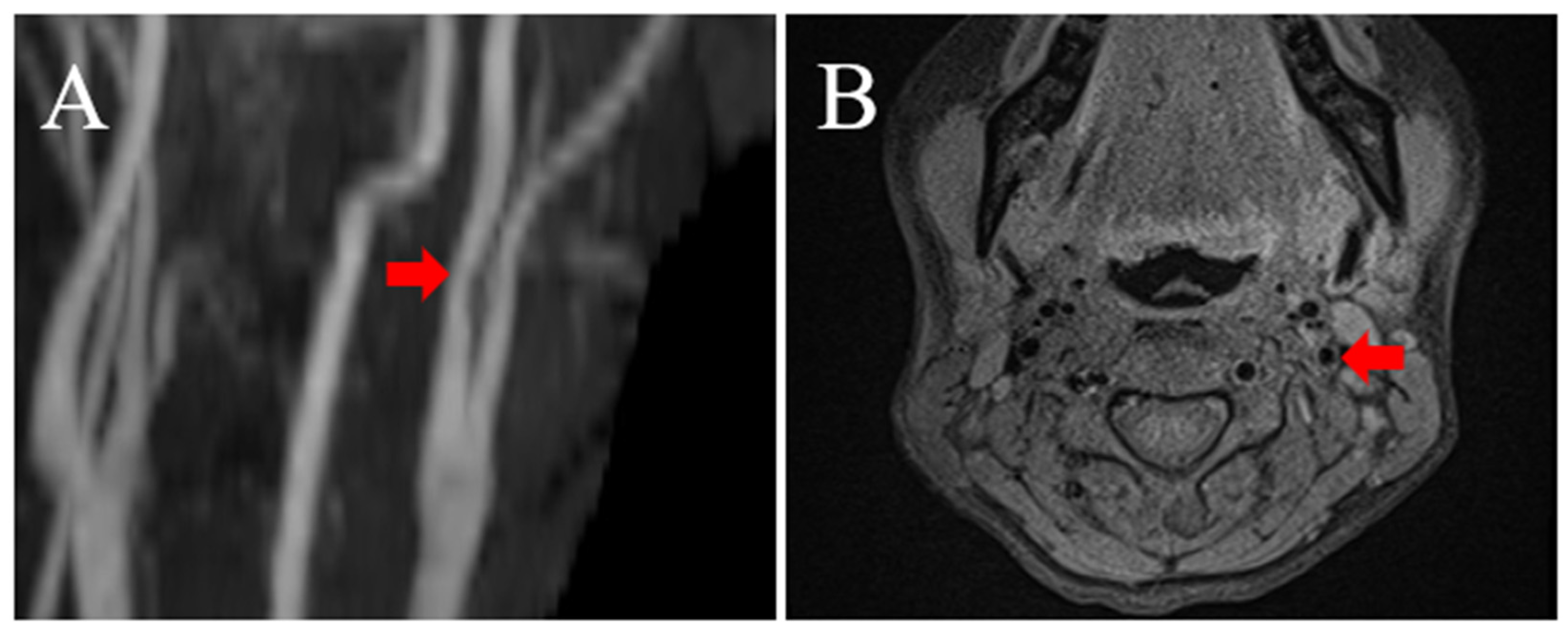
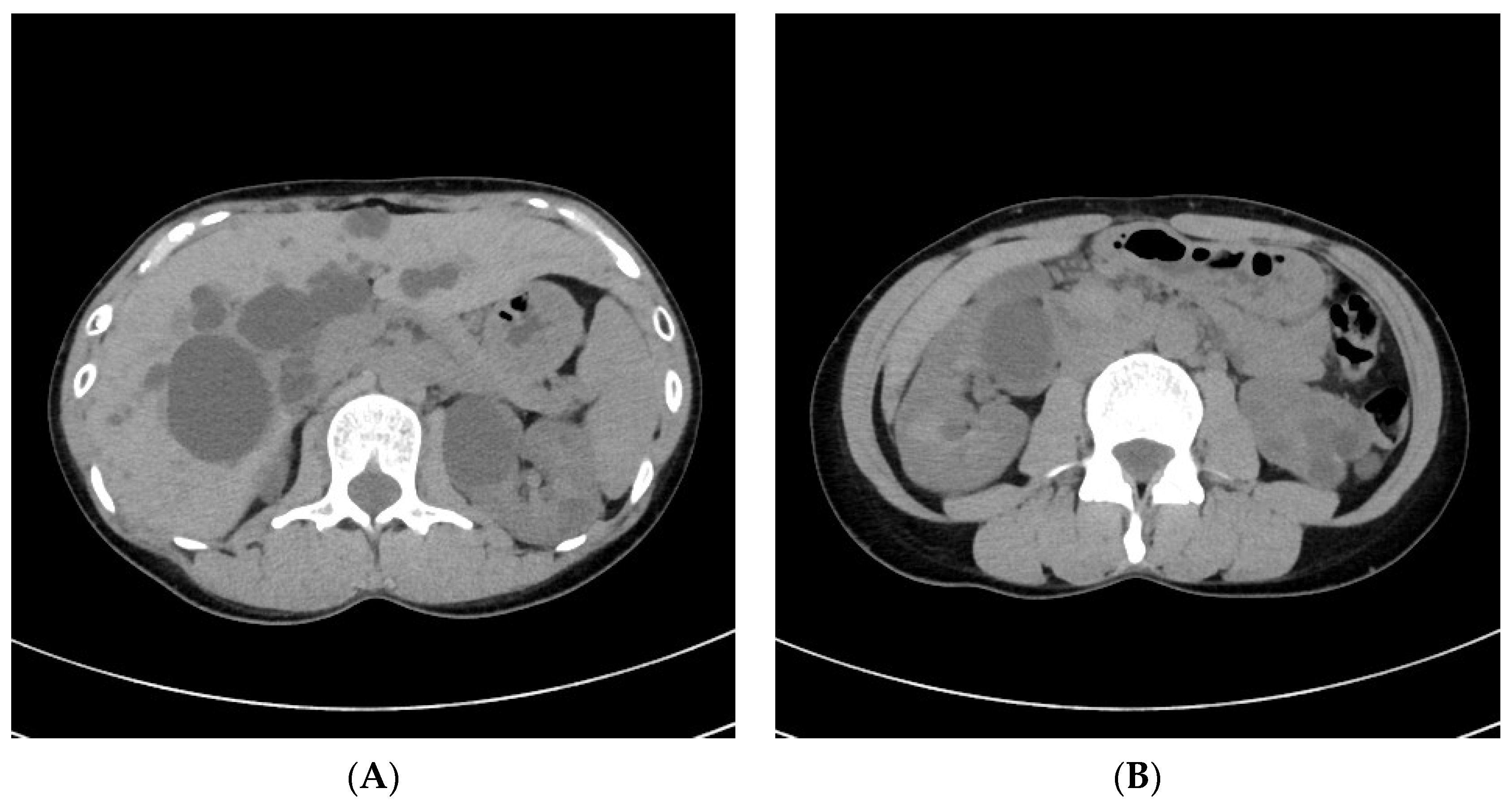
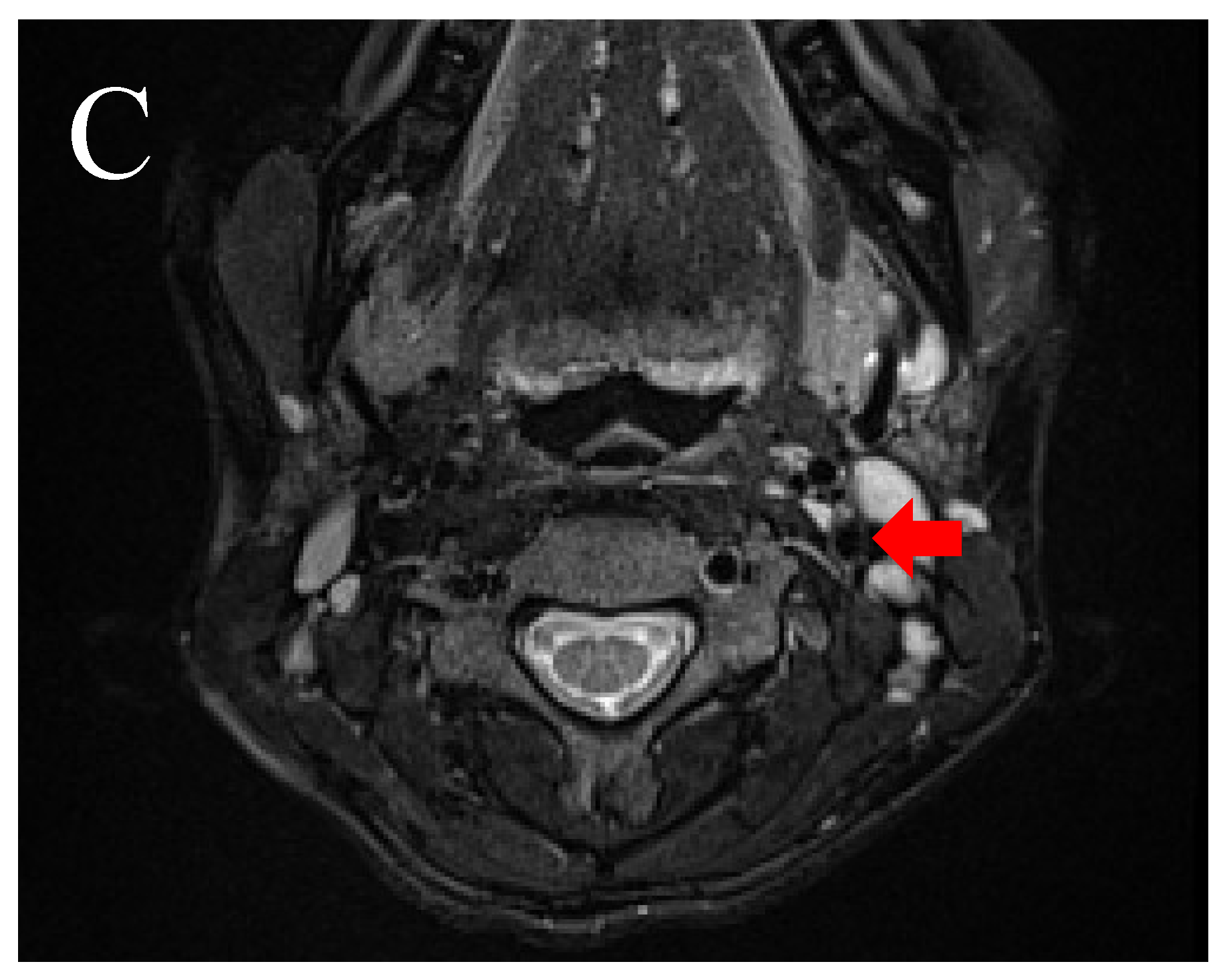
2. Illustrative Case
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harris, P.C.; Torres, V.E. Polycystic Kidney Disease, Autosomal Dominant. In GeneReviews®; Adam, M.P., Ardinger, H.H., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Gripp, K.W., Mirzaa, G.M., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 2018. [Google Scholar]
- Pirson, Y. Extrarenal Manifestations of Autosomal Dominant Polycystic Kidney Disease. Adv. Chronic Kidney Dis. 2010, 17, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Pirson, Y.; Chauveau, D.; Torres, V. Management of Cerebral Aneurysms in Autosomal Dominant Polycystic Kidney Disease. J. Am. Soc. Nephrol. 2002, 13, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Torres, V.E.; Harris, P.C.; Pirson, Y. Autosomal dominant polycystic kidney disease. Lancet 2007, 369, 1287–1301. [Google Scholar] [CrossRef]
- Bobrie, G.; Brunet-Bourgin, F.; Alamowitch, S.; Coville, P.; Kassiotis, P.; Kermarrec, A.; Chauveau, D. Spontaneous artery dissection: Is it part of the spectrum of autosomal dominant polycystic kidney disease? Nephrol. Dial. Transplant. 1998, 13, 2138–2141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roth, C.; Kleffmann, J.; Bergmann, C.; Deinsberger, W.; Ferbert, A. Ruptured Cerebral Aneurysm and Acute Bilateral Carotid Artery Dissection in a Patient with Polycystic Kidney Disease and Polycystic Liver Disease. Cerebrovasc. Dis. 2013, 35, 590–591. [Google Scholar] [CrossRef] [PubMed]
- Windpessl, M.; Stadler, K.; Lampl, R.; Wallner, M. Horner syndrome in renal clinic: A woman with polycystic kidney disease and spontaneous carotid artery dissection. Nephrology 2013, 18, 315. [Google Scholar] [CrossRef]
- Kuroki, T.; Yamashiro, K.; Tanaka, R.; Hirano, K.; Shimada, Y.; Hattori, N. Vertebral Artery Dissection in Patients with Autosomal Dominant Polycystic Kidney Disease. J. Stroke Cerebrovasc. Dis. 2014, 23, e441–e443. [Google Scholar] [CrossRef]
- Chen, Z.; Yuan, J.; Li, H.; Yuan, C.; Yin, K.; Liang, S.; Li, P.; Wu, M. Isolated hypoglossal nerve palsy from internal carotid artery dissection related to PKD-1 gene mutation. BMC Neurol. 2019, 19, 276. [Google Scholar] [CrossRef]
- Arnold, M.; Kappeler, L.; Georgiadis, D.; Berthet, K.; Keserue, B.; Bousser, M.G.; Baumgartner, R.W. Gender differences in spontaneous cervical artery dissection. Neurology 2006, 67, 1050–1052. [Google Scholar] [CrossRef]
- Touzé, E.; Gauvrit, J.-Y.; Moulin, T.; Meder, J.-F.; Bracard, S.; Mas, J.-L. Risk of stroke and recurrent dissection after a cervical artery dissection: A multicenter study. Neurology 2003, 61, 1347–1351. [Google Scholar] [CrossRef]
- Blum, C.A.; Yaghi, S. Cervical Artery Dissection: A Review of the Epidemiology, Pathophysiology, Treatment, and Outcome. Arch. Neurosci. 2015, 2, e26670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schievink, W.I. Spontaneous Dissection of the Carotid and Vertebral Arteries. N. Engl. J. Med. 2001, 344, 898–906. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Drummond, I.; Ibraghimov-Beskrovnaya, O.; Klinger, K.; Arnaout, M.A. Polycystin 1 is required for the structural integrity of blood vessels. Proc. Natl. Acad. Sci. USA 2000, 97, 1731–1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nauli, S.M.; Alenghat, F.; Luo, Y.; Williams, E.; Vassilev, P.; Li, X.; Elia, A.E.H.; Lu, W.; Brown, E.M.; Quinn, S.J.; et al. Polycystins 1 and 2 mediate mechanosensation in the primary cilium of kidney cells. Nat. Genet. 2003, 33, 129–137. [Google Scholar] [CrossRef]
- Lu, W.; Peissel, B.; Babakhanlou, H.; Pavlova, A.; Geng, L.; Fan, X.; Larson, C.; Brent, G.; Zhou, J. Perinatal lethality with kidney and pancreas defects in mice with a targetted Pkd1 mutation. Nat. Genet. 1997, 17, 179–181. [Google Scholar] [CrossRef]
- Griffin, M.D.; Torres, E.V.; Grande, J.P.; Kumar, R. Vascular expression of polycystin. J. Am. Soc. Nephrol. 1997, 8, 616–626. [Google Scholar] [CrossRef]
- Mazzon, E.; Rocha, D.; Brunser, A.; De la Barra, C.; Stecher, X.; Bernstein, T.; Zúñiga, P.; Díaz, V.; Martínez, G.; Venturelli, P.M. Cervical Artery Dissections with and without stroke, risk factors and prognosis: A Chilean prospective cohort. J. Stroke Cerebrovasc. Dis. 2020, 29, 104992. [Google Scholar] [CrossRef]
- Oppenheim, C.; Naggara, O.; Touzé, E.; Lacour, J.-C.; Schmitt, E.; Bonneville, F.; Crozier, S.; Guégan-Massardier, E.; Gerardin, E.; Leclerc, X.; et al. High-Resolution MR Imaging of the Cervical Arterial Wall: What the Radiologist Needs to Know. RadioGraphics 2009, 29, 1413–1431. [Google Scholar] [CrossRef]
- Crombag, G.; Aizaz, M.; Schreuder, F.; Benali, F.; van Dam-Nolen, D.; Liem, M.; Lucci, C.; van der Steen, A.; Daemen, M.; Mess, W.; et al. Proximal Region of Carotid Atherosclerotic Plaque Shows More Intraplaque Hemorrhage: The Plaque at Risk Study. AJNR Am. J. Neuroradiol. 2022, 43, 265–271. [Google Scholar] [CrossRef]
- Markus, H.S.; Levi, C.; King, A.; Madigan, J.; Norris, J. Antiplatelet Therapy vs Anticoagulation Therapy in Cervical Artery Dissection: The Cervical Artery Dissection in Stroke Study (CADISS) Randomized Clinical Trial Final Results. JAMA Neurol. 2019, 76, 657–664. [Google Scholar] [CrossRef]
- Larsson, S.C.; King, A.; Madigan, J.; Levi, C.; Norris, J.W.; Markus, H.S. Prognosis of carotid dissecting aneurysms: Results from CADISS and a systematic review. Neurology. 2017, 88, 646–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strunk, D.; Schwindt, W.; Wiendl, H.; Dittrich, R.; Minnerup, J. Long-Term Sonographical Follow-Up of Arterial Stenosis Due to Spontaneous Cervical Artery Dissection. Front Neurol. 2021, 12, 792321. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Publication Year) | Sex/Age | Side | Presenting Symptoms or Signs | Treatment | Outcome (Causes) | F.Hx. of ADPKD |
|---|---|---|---|---|---|---|
| Bobrie G et al. (1998) | M/48 | Lt. | Neck pain, rt. hemiparesis, aphasia | Anticoagulation | Favorable | No |
| M/53 | Rt. | Neck pain, lt. hemiplegia | N.A. | Sequelae (infarction) | No | |
| M/49 | Rt. | Neck pain, Horner syndrome, lower CN palsy | Aspirin | Favorable | No | |
| F/34 | Lt. | Asymptomatic | Aspirin | Favorable | N.A. | |
| Roth C et al. (2013) | F/39 | Bilat. | Headache, lt. hemiparesis | None | N.A. | Yes |
| Windpessl M et al. (2013) | F/35 | Rt. | Headache, Horner syndrome | Heparin | Favorable | Yes |
| Kuroki T et al. (2014) | M/32 | Lt. | Asymptomatic | N.A. | N.A. | Yes |
| Chen Z et al. (2019) | M/42 | Rt. | Neck pain, rt. hypoglossal nerve palsy | Clopidogrel | Favorable | N.A. |
| Present case | F/38 | Lt. | Neck pain | None | Favorable | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Izumo, T.; Ogawa, Y.; Matsuo, A.; Okamura, K.; Takahira, R.; Sadakata, E.; Yoshida, M.; Yamaguchi, S.; Tateishi, Y.; Baba, S.; et al. A Spontaneous Extracranial Internal Carotid Artery Dissection with Autosomal Dominant Polycystic Kidney Disease: A Case Report and Literature Review. Medicina 2022, 58, 679. https://doi.org/10.3390/medicina58050679
Izumo T, Ogawa Y, Matsuo A, Okamura K, Takahira R, Sadakata E, Yoshida M, Yamaguchi S, Tateishi Y, Baba S, et al. A Spontaneous Extracranial Internal Carotid Artery Dissection with Autosomal Dominant Polycystic Kidney Disease: A Case Report and Literature Review. Medicina. 2022; 58(5):679. https://doi.org/10.3390/medicina58050679
Chicago/Turabian StyleIzumo, Tsuyoshi, Yuka Ogawa, Ayaka Matsuo, Kazuaki Okamura, Ryotaro Takahira, Eisaku Sadakata, Michiharu Yoshida, Susumu Yamaguchi, Yohei Tateishi, Shiro Baba, and et al. 2022. "A Spontaneous Extracranial Internal Carotid Artery Dissection with Autosomal Dominant Polycystic Kidney Disease: A Case Report and Literature Review" Medicina 58, no. 5: 679. https://doi.org/10.3390/medicina58050679
APA StyleIzumo, T., Ogawa, Y., Matsuo, A., Okamura, K., Takahira, R., Sadakata, E., Yoshida, M., Yamaguchi, S., Tateishi, Y., Baba, S., Morofuji, Y., Hiu, T., Anda, T., & Matsuo, T. (2022). A Spontaneous Extracranial Internal Carotid Artery Dissection with Autosomal Dominant Polycystic Kidney Disease: A Case Report and Literature Review. Medicina, 58(5), 679. https://doi.org/10.3390/medicina58050679