Abstract
Objective: This article aims to describe a unique case of didanosine-induced retinal degeneration that was discovered 11 years after the drug withdrawal. Case report: The patient is a 42-year-old woman with a medical history of HIV and hepatitis C virus since 2004. She has been prescribed antiretroviral therapy since then. For the first seven years (2004–2011), the patient was prescribed a combination therapy consisting of didanosine, efavirenz, and lamivudine. The protocol was changed to atripla (efavirenz, emtricitabine, and tenofovir) from 2011 to 2021. Recently (October 2021–January 2021), the patient was prescribed eviplera (rilpivirin, emtricitabine, and tenofovir). In addition, her past medical history revealed Gougerot-Sjogren syndrome and rheumatoid arthritis. She was prescribed hydroxychloroquine (HCQ) (2009–2021) at a dose of 400 mg daily. She had no vision complaint. Results: During her routine HCQ screening at the eye clinic, University Hospital Bretonneau, Tours, France, the widefield colour fundus photograph showed well-defined symmetric mid-peripheral areas of chorioretinal atrophy sparing the posterior pole of both eyes. Furthermore, the widefield fundus autofluorescence illustrated mid-peripheral round well-demarcation hypoautofluorescent areas of chorioretinal atrophy of both eyes. Conversely, the macular optical coherence tomography (OCT) was normal. Many of her drugs are known to be associated with retinopathy such as HCQ, tenofovir, efavirenz, and didanosine. Because our data corroborate peripheral retinal damage rather than posterior pole damage, this case report is compatible with didanosine-induced retinopathy rather than HCQ, efavirenz, or tenofovir retinal toxicity. Conclusions: All HIV patients who are presently or were previously on didanosine therapy should have their fundus examined utilising widefield fundus autofluorescence and photography.
1. Introduction
According to the World Health Organization (WHO), the global prevalence of human immunodeficiency virus (HIV) infection is estimated to be 0.7 percent [1]. At the end of 2020, 37.7 million individuals worldwide were living with HIV [2]. Every day, 15,000 to 20,000 new cases are reported [3]. Most HIV patients require lengthy treatment with a combination of various drugs, which are known to be associated with retinopathy, such nucleoside reverse transcriptase inhibitors (NRTI) including didanosine, tenofovir, and zidovudine, non-nucleoside reverse transcriptase inhibitors (NNRTI) including efavirenz, and protease inhibitors such as ritonavir [4,5,6,7,8].
Didanosine is a synthetic purine nucleoside analogue belonging to the NRTI category of medicines. It has been licensed by the US Food and Drug Administration (FDA) for the combination therapy of HIV since October 1991. Didanosine toxicity is usually accompanied with mid-peripheral retinopathy, which might worsen long after treatment is stopped [5]. As far as we know, only 26 cases of didanosine retinopathy were recorded between 1992 and June 2021 [6].
We present a case of didanosine-associated mid-peripheral retinopathy that was identified incidentally in an HIV patient who was prescribed the drug for seven years (2004–2011).
2. Case Report
2.1. Patient Information
A 42-year-old woman was referred to our clinic for hydroxychloroquine (HCQ) maculopathy screening (Table 1 shows the demographic, medical, and drug history information). She had a medical history of HIV and hepatitis C virus since 2004. She has been prescribed antiretroviral therapy since then. The patient was prescribed a combination therapy consisting of didanosine, efavirenz, and lamivudine (2004–2011). The protocol was changed to atripla (efavirenz, emtricitabine, and tenofovir) from 2011 to 2021. Recently (October 2021–January 2021) the patient was prescribed eviplera (rilpivirin, emtricitabine, and tenofovir) (Table 2). In addition, her past medical history revealed Gougerot-Sjogren syndrome and rheumatoid arthritis since 1995. She had been prescribed hydroxychloroquine (HCQ) since 2009 at a dose of 400 mg per day. Her cumulative dose of HCQ was 1800 g.

Table 1.
The patient demographic, medical, and drug history information.
Table 2.
Antiretroviral treatment taken by the patient from 2004 to January 2022.
She was referred to the eye clinic, University Hospital Bretonneau, Tours, France, for routine HCQ retinal toxicity screening. The patient reported no visual symptoms. Her last CD4+ count was 416 copies/mL, and her HIV plasma viral load was undetectable (below 20 copies/mL). The patient neither had a personal history of cytomegalovirus (CMV) retinitis or HIV retinopathy nor a family history of eye disease.
2.2. Visual Examination
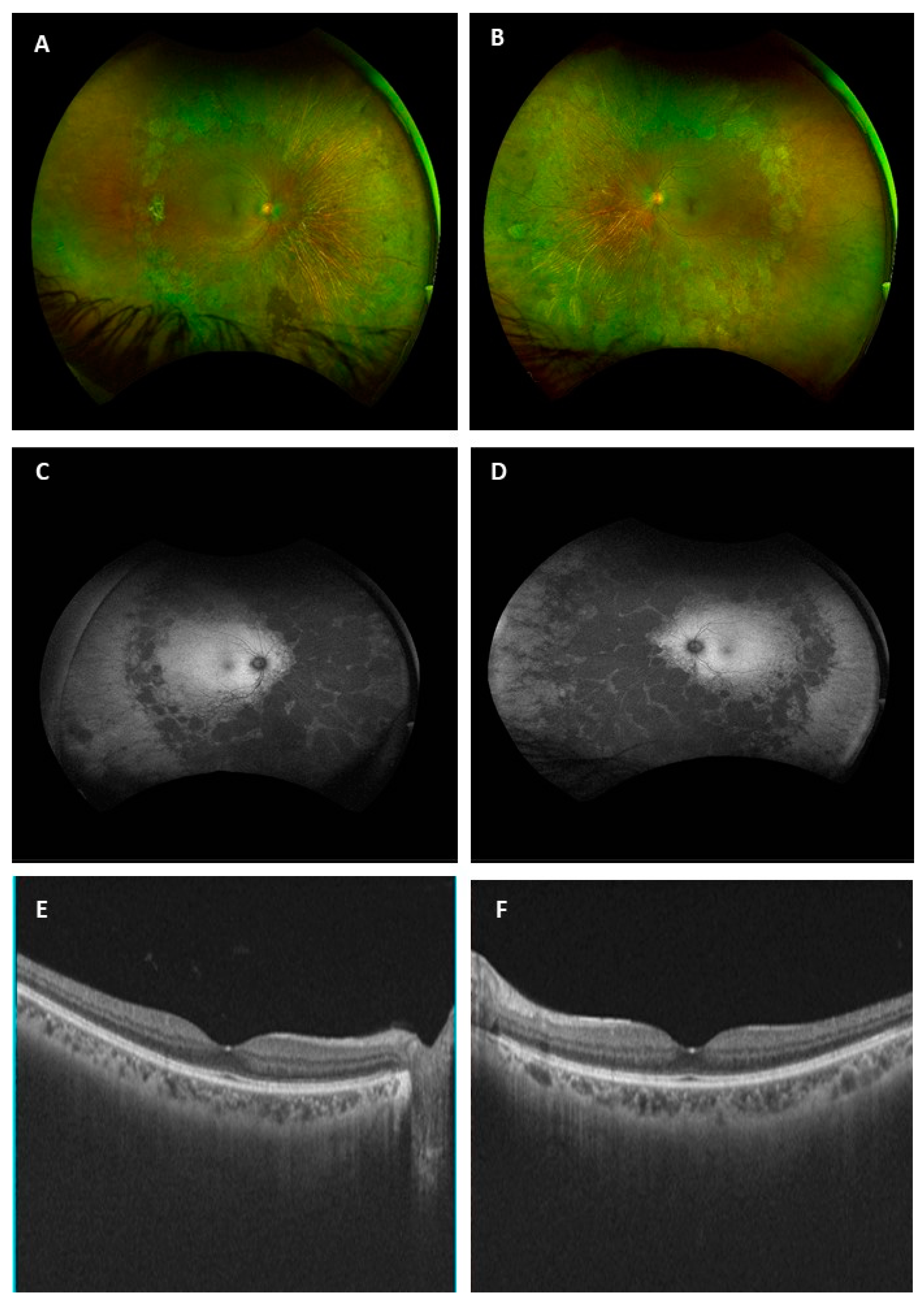
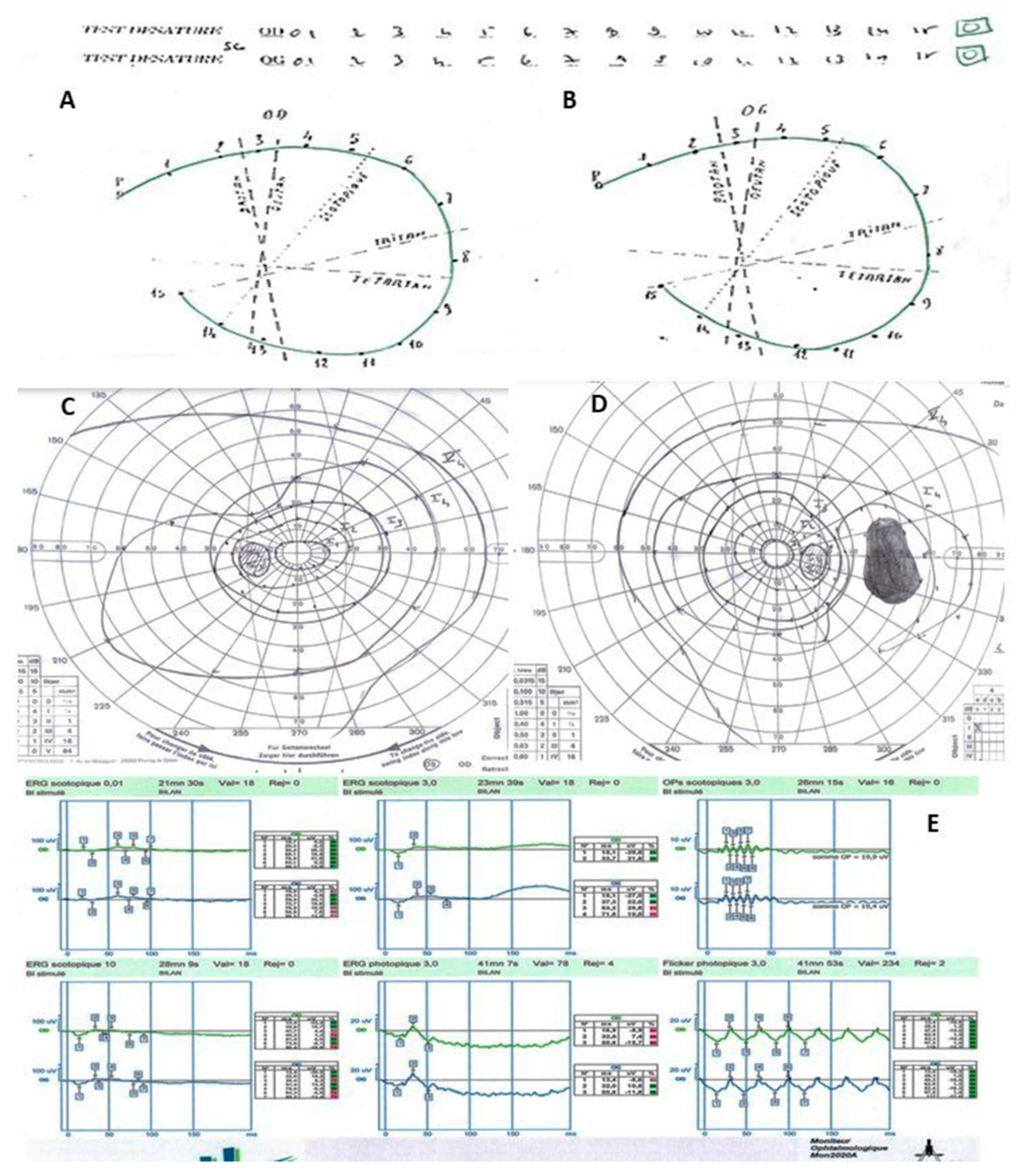
On biomicroscopic examination, the best-corrected visual acuity measured using a logMAR chart (Logarithm of the Minimum Angle of Resolution) was 0.00 logMAR in both eyes. The intraocular pressure was 11 mmHg in both eyes. The slit-lamp examination was unremarkable in both eyes. The widefield colour fundus photograph (OPTOS California Ultra-widefield non-mydriatic fundus camera) showed well-defined symmetric mid-peripheral areas of chorioretinal atrophy sparing the posterior pole of both eyes (Figure 1A,B). The widefield fundus autofluorescence (OPTOS California Ultra-widefield non-mydriatic fundus camera) illustrated mid-peripheral round well-demarcation hypoautofluorescent areas in the peripheral retina of both eyes (Figure 1C,D). Macular optical coherence tomography (TOPCON DRI Swept Source OCT) of the posterior pole was normal for both eyes (Figure 1E,F). The colour vision test (Farnsworth desaturated 15 Hue colour test) was unremarkable (Figure 2A,B). The Goldmann kinetic perimetry visual field showed a superior temporal depression with the I4e isopter in the left eye and absolute scotomas in the temporal mid-peripheral field between 30° and 60° in the right eye (Figure 2C,D). A full-field electroretinogram (ffERG, MonPackONE, METROVISION), conducted according to the International Society for the Clinical Electrophysiology of Vision (ISCEV) standards, revealed moderately generalized rod and cone dysfunction in both eyes (Figure 2E). The static semi-automated visual field with the 12 central degree was unremarkable (Figure 3).
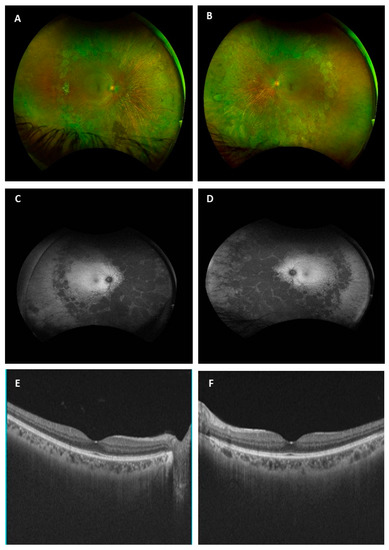
Figure 1.
Ultra-widefield fundus photographs of the right (A) and left (B) eye performed using the optos camera showed well-delineated concentrical mid peripheral patches of chorioretinal atrophy sparing the macula in both eyes. Ultra-widefield short-wavelength fundus autofluorescence illustrated mid-peripheral round well-demarcated patchy loss of autofluorescence in both eyes (C,D). Macular Optical coherence tomography (OCT) photos showed no macular abnormality in either eye (E,F).
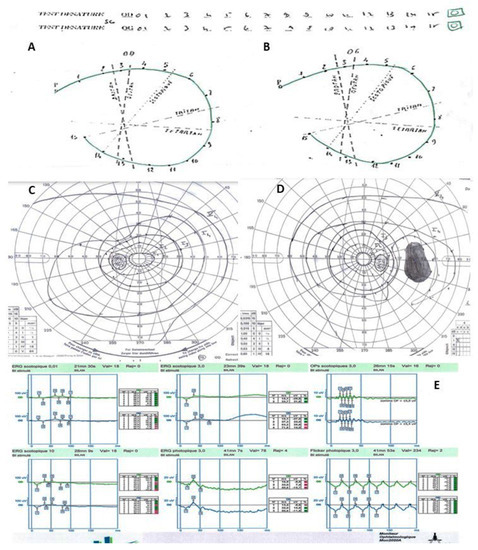
Figure 2.
Farnsworth D-15 colour vision tests showed no abnormality in either eye (A,B). Goldmann kinetic visual field revealed (C) a superior temporal depression with the I4e isopter in the left eye and (D) absolute scotomas in the temporal mid-peripheral field between 30° and 60° in the right eye. A full-field electroretinogram (ERG) revealed moderate generalized rod and cone dysfunction in both eyes (E).
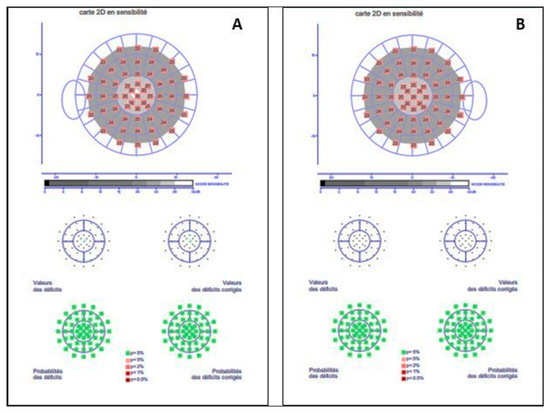
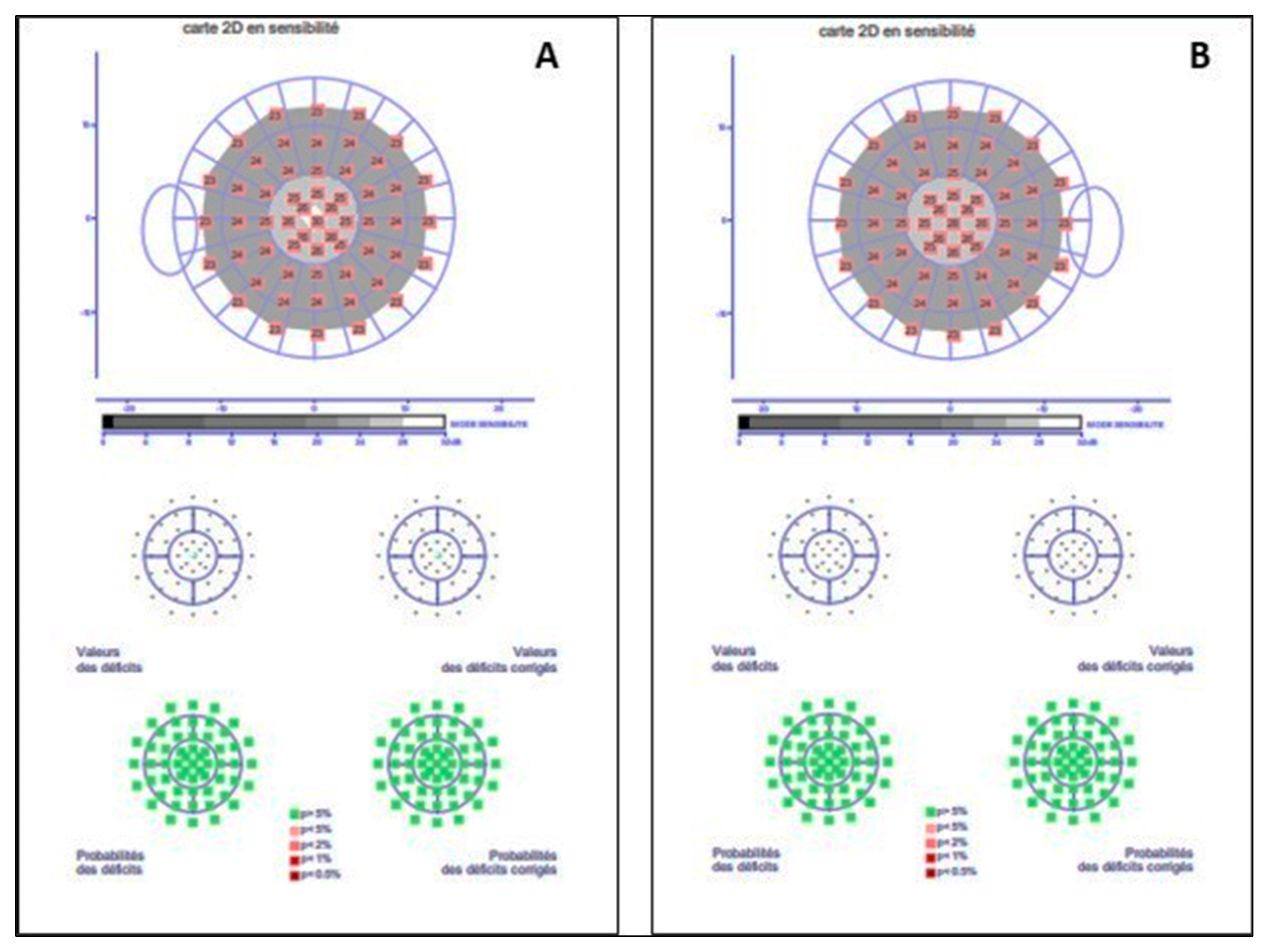
Figure 3.
Static visual field test within the 12 central degree FAST 12 perimetry Metrovision visual field test showed no central field defects in either eye (A: left eye; B: right eye).
3. Discussion
Because of the advancement of antiretroviral medications, the majority of HIV patients now enjoy long-term remission. Often, a cocktail of several drugs is required to stabilize the disease’s progress. Unfortunately, unwanted side effects might arise with long-term therapy, and determining which medicine is the cause can be difficult [6]. While HIV retinopathy, opportunistic infections, and some malignancies are the most common causes of retinal problems, toxic medication effects must also be mentioned. HIV patients are frequently subjected to many drugs, including clofazimine, zidovudine, didanosine, efavirenz, and ritonavir, all of which have been linked to retinopathies [7,8].
Here, we report a case of peripheral retinopathy that was incidentally diagnosed during regular HCQ screening at our eye clinic, University Hospital Bretonneau, Tours, France. This case involved a woman with a history of HIV, hepatitis C virus, Gougerot-Sjogren syndrome, and rheumatoid arthritis. By examining the patient’s medication history, we discovered four medications that could cause retinopathy: HCQ, tenofovir, efavirenz, and didanosine.
HCQ is an immunomodulator being used to treat malaria and autoimmune illnesses such as systemic lupus erythematosus and inflammatory arthritis [9]. Treatment with a high dose of HCQ, on the other hand, may result in toxic retinopathy [10]. Perifoveal rods and cones are classically involved in HCQ retinopathy with an initial foveal conesparing [11,12]. Efavirenz, a first-generation NNRTI, is a component of primary antiretroviral therapy [13]. One publication reported few cases of maculopathy secondary to efavirenz treatment. Despite the fact of its toxic effect on the retinal pigment epithelium, efavirenz retinopathy usually affects the parafoveal region [14]. Tenofovir, a NRTI, is another antiretroviral drug. Long-term tenofovir use has been linked to retinal pigment epitheliopathy, according to Mehrotra et al. [15]. In the absence of macular involvement, HCQ, efavirenz, or tenofovir retinal toxicity could be excluded.
Didanosine is a synthetic purine nucleoside analogue that belongs to the NRTI group of medicines. It has been licensed by the FDA since October 1991 for the combination treatment of HIV [16]. Didanosine-induced retinal toxicity was first recorded in 1992 with a report of three immunocompromised children treated with didanosine who developed symmetrical bilateral peripheral retinal atrophy that spared the macula. Numerous case reports have documented a characteristic pattern of didanosine-induced retinopathy in HIV-infected individuals, including symmetrical bilateral mid-peripheral concentric retinal atrophy anterior to the posterior pole [5,6,17,18,19,20]. Whitcup et al. demonstrated the absence of macular damage in a child taking didanosine with a histological report of a normal structure of the macular, choriocapillaris, and retinal pigment epithelium [21]. Because our data corroborate peripheral retinal damage rather than posterior pole damage, this case report is compatible with didanosine-induced retinopathy rather than HCQ, efavirenz, or tenofovir retinal toxicity.
Didanosine-related retinal toxicity is usually asymptomatic, and patients retain adequate vision [6]; nevertheless, in advanced cases, the visual field may be significantly compromised [18]. The patient in our situation had undergone treatment with didanosine for seven years (2004–2011) and then stopped 11 years ago; yet, the pathological picture is perfectly compatible with the drug’s toxicity. Furthermore, the majority of the newly identified retinal impairment cases were reported in individuals who had stopped taking didanosine. Given this, it is not unexpected that many patients continue to deteriorate even after stopping didanosine [5]. Despite the discontinuation of the drug, the explanation for the progression of didanosine-induced retinopathy is unknown. One possibility is that the retinal cells were triggered by an irreversible cell death process before treatment was discontinued and, thus, continued to degenerate even after the drug was stopped. The possibility of further toxicity from drugs used as therapeutic switches cannot be ruled out. Other NRTI, such as zidovudine, entecavir, lamivudine, and a protease inhibitor, ritonavir, have been linked to retinopathy. To address this concern, continuous retinal screening of patients taking the new generation of NRTI can be proposed [22].
Because the defects are limited to the mid-peripheral retina, and symptoms are delayed due to macular sparing, diagnosing didanosine toxicity can be difficult. As a result, a thorough fundus examination using multimodal imaging, such as widefield fundus autofluorescence and widefield fundus photography, is beneficial in detecting peripheral abnormalities and monitoring patients [19].
4. Conclusions
A case of didanosine-induced mid-peripheral chorioretinal degeneration in an HIV patient with no visual complaints was reported. The case was detected eleven years after the didanosine cessation. All HIV patients who are presently or previously on didanosine therapy should have their fundus examined utilising widefield fundus autofluorescence and widefield fundus photography.
Author Contributions
Conceptualization, M.L.L.-L. and H.J.; diagnosis, M.L.L.-L.; writing—original draft preparation, H.J.; writing—review and editing, H.J. and M.L.L.-L.; supervision, P.-J.P. and I.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and was approved (2022_045) by University Hospital Bretonneau of Tours, Francois Rabelais Medicine Faculty of Tours, Tours, France.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Jing, L.; Deng, J.; Kozak, I.; Zhang, H.; Chen, S.; Yang, Y.; Qi, X.; Tang, L.; Adelman, R.; Forster, S. Prevalence of Ocular Manifestations of HIV/AIDS in the Highly Active Antiretroviral Therapy (HAART) Era: A Different Spectrum in Central South China. Ophthalmic Epidemiol. 2013, 20, 170–175. [Google Scholar] [CrossRef]
- WHO HIV/AIDS. Available online: https://www.who.int/data/gho/data/themes/hiv-aids (accessed on 22 March 2022).
- Feroze, K.; Wang, J. Ocular Manifestations of HIV; StatPearls Publishing: Treasure Island, FL, USA, January 2022. [Google Scholar]
- Lalonde, R.G.; Deschenes, J.G.; Seamone, C. Zidovudine-Induced Macular Edema. Ann. Intern. Med. 1991, 114, 297–298. [Google Scholar] [CrossRef]
- Haug, S.; Wong, R.; Day, S.; Choudhry, N.; Sneed, S.; Prasad, P.; Read, S.; McDonald, R.; Agarwal, A.; Davis, J.; et al. Didanosine Retinal Toxicity. Retina 2016, 36, S159–S167. [Google Scholar] [CrossRef]
- Hammer, A.; Borruat, F. Case Report: Multimodal Imaging of Toxic Retinopathies Related to Human Immunodeficiency Virus Antiretroviral Therapies: Maculopathy vs. Peripheral Retinopathy. Report of Two Cases and Review of the Literature. Front. Neurol. 2021, 12, 905. [Google Scholar] [CrossRef] [PubMed]
- Bunod, R.; Miere, A.; Zambrowski, O.; Girard, P.; Surgers, L.; Souied, E. Ritonavir Associated Maculopathy– Multimodal Imaging and Electrophysiology Findings. Am. J. Ophthalmol. Case Rep. 2020, 19, 100783. [Google Scholar] [CrossRef] [PubMed]
- Sudharshan, S.; Kumar, K.; Bhende, M.; Biswas, J.; Selvamuthu, P. Efavirenz-Associated Retinal Toxicity Presenting with Night Vision Defects in Patients with Human Immunodeficiency Virus. Ocul. Immunol. Inflamm. 2020, 28, 1076–1084. [Google Scholar] [CrossRef] [PubMed]
- Liang, N.; Zhong, Y.; Zhou, J.; Liu, B.; Lu, R.; Guan, Y.; Wang, Q.; Liang, C.; He, Y.; Zhou, Y.; et al. Immunosuppressive Effects of Hydroxychloroquine and Artemisinin Combination Therapy via the Nuclear Factor-ΚB Signaling Pathway in Lupus Nephritis Mice. Exp. Ther. Med. 2018, 15, 2436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costedoat-Chalumeau, N.; Dunogué, B.; Leroux, G.; Morel, N.; Jallouli, M.; Le Guern, V.; Piette, J.; Brézin, A.; Melles, R.; Marmor, M. A Critical Review of the Effects of Hydroxychloroquine and Chloroquine on the Eye. Clin. Rev. Allergy Immunol. 2015, 49, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Çay, H.; Erol, M.; Çoban, D.; Bulut, M.; Sezer, I.; Çakir, T.; Toraman, N. Retinotoxicity of Hydroxychloroquine: Is It Possible to Demonstrate by Spectral Domain Optical Coherence Tomography Before Development? A Cross Sectional Investigation. Arch. Rheumatol. 2014, 29, 178–185. [Google Scholar] [CrossRef] [Green Version]
- Pham, B.; Marmor, M. Sequential Changes in Hydroxychloroquine Retinopathy up to 20 Years after Stopping the Drug: Implications for Mild versus Severe Toxicity. Retina 2019, 39, 492–501. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.; Aberg, J.; Hoy, J.; Telenti, A.; Benson, C.; Cahn, P.; Eron, J.; Günthard, H.; Hammer, S.; Reiss, P.; et al. Antiretroviral Treatment of Adult HIV Infection: 2012 Recommendations of the International Antiviral Society-USA Panel. JAMA 2012, 308, 387–402. [Google Scholar] [CrossRef] [PubMed]
- Sen, P.; Sudharshan, S.; Banerjee, A.; Dhami, A. Clinical and Electrophysiological Characteristics of Efavirenz-Induced Macular Toxicity. GMS Ophthalmol. Cases 2020, 10, Doc08. [Google Scholar] [CrossRef] [PubMed]
- Mehrotra, N.; Nagpal, M.; Talati, S. Presumed Tenofovir Toxicity. Retin. Today 2020, 2020, 12–14. [Google Scholar]
- Scholar, E. HIV Nucleoside Reverse Transcriptase Inhibitors. In xPharm: The Comprehensive Pharmacology Reference; Elsevier Inc.: Amsterdam, The Netherlands, 2007; pp. 1–3. ISBN 9780080552323. [Google Scholar]
- Whitcup, S.M.; Butler, K.M.; Caruso, R.; de Smet, M.D.; Rubin, B.; Husson, R.N.; Lopez, J.S.; Belfort, R.; Pizzo, P.A.; Nussenblatt, R.B. Retinal Toxicity in Human Immunodeficiency Virus-Infected Children Treated with 2′,3′-Dideoxyinosine. Am. J. Ophthalmol. 1992, 113, 1–7. [Google Scholar] [CrossRef]
- Nderitu, P.; Riga, P.; Mann, S.; Garnavou-Xirou, C.; Eleftheriadis, H. Didanosine-Associated Retinal Toxicity (DART) Amongst HIV-Positive Patients: A Case Series and Literature Review. SN Compr. Clin. Med. 2020, 2, 2939–2952. [Google Scholar] [CrossRef]
- Gabrielian, A.; MacCumber, M.; Kukuyev, A.; Mitsuyasu, R.; Holland, G.; Sarraf, D. Didanosine-Associated Retinal Toxicity in Adults Infected With Human Immunodeficiency Virus. JAMA Ophthalmol. 2013, 131, 255–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corradetti, G.; Violanti, S.; Au, A.; Sarraf, D. Wide Field Retinal Imaging and the Detection of Drug Associated Retinal Toxicity. Int. J. Retin. Vitr. 2019, 5, 26. [Google Scholar] [CrossRef] [Green Version]
- Whitcup, S.; Dastgheib, K.; Nussenblatt, R.; Walton, R.; Pizzo, P.; Chan, C. A Clinicopathologic Report of the Retinal Lesions Associated With Didanosine. Arch. Ophthalmol. 1994, 112, 1594–1598. [Google Scholar] [CrossRef] [PubMed]
- Faure, C.; Chassery, M.; Ores, R.; Audo, I. Didanosine-induced Retinopathy: New Insights with Long-term Follow-up. Ocul. Immunol. Inflamm. 2021, 13, 1–8. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).