
Management of Class III Malocclusion and Maxillary Transverse Deficiency with Microimplant-Assisted Rapid Palatal Expansion (MARPE): A Case Report

Abstract
:1. Introduction
2. Case Report
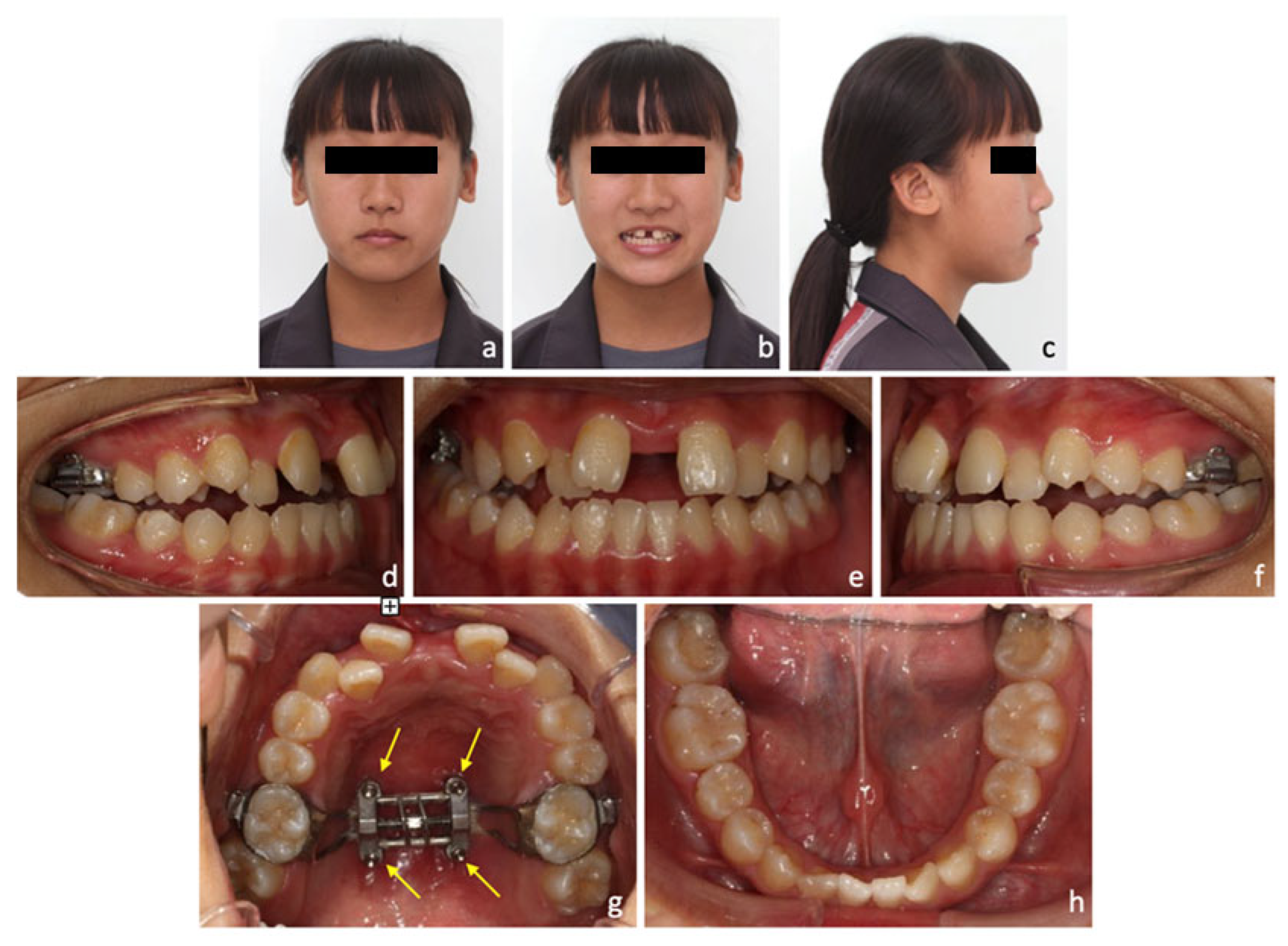
2.1. Diagnosis and Aetiology
2.2. Treatment Alternatives
2.3. Treatment Progress
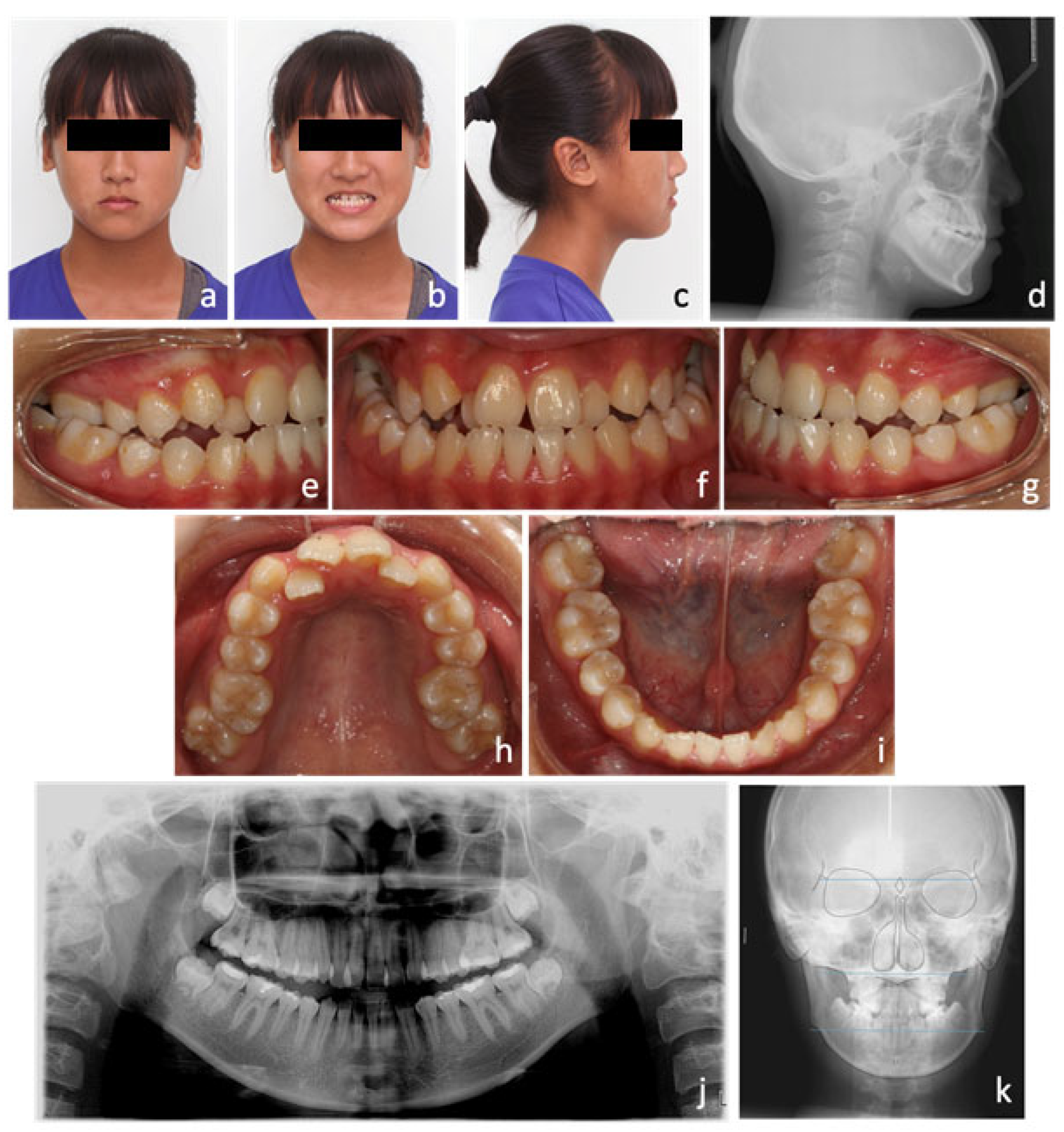
2.4. Treatment Results
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McNamara, J.A., Jr. An orthopedic approach to the treatment of Class III malocclusion in young patients. J. Clin. Orthod. 1987, 21, 598–608. [Google Scholar] [PubMed]
- Nucci, L.; Costanzo, C.; Carfora, M.; d’Apuzzo, F.; Franchi, L.; Perillo, L. Dentoskeletal effects of early class III treatment protocol based on timing of intervention in children. Prog. Orthod. 2021, 22, 49. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Xu, T.; Zou, W. Effects of rapid maxillary expansion on the midpalatal suture: A systematic review. Eur. J. Orthod. 2015, 37, 651–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bizzarro, M.; Generali, C.; Maietta, S.; Martorelli, M.; Ferrillo, M.; Flores-Mir, C.; Perillo, L. Association between 3D palatal morphology and upper arch dimensions in buccally displaced maxillary canines early in mixed dentition. Eur. J. Orthod. 2018, 40, 592–596. [Google Scholar] [CrossRef] [PubMed]
- Lagravere, M.O.; Carey, J.; Heo, G.; Toogood, R.W.; Major, P.W. Transverse, vertical, and anteroposterior changes from bone-anchored maxillary expansion vs. traditional rapid maxillary expansion: A randomized clinical trial. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 304 e1–e12; discussion 304–305. [Google Scholar] [CrossRef]
- Chuang, Y.H.; Chen, J.H.; Ho, K.H.; Wang, K.L.; Hsieh, S.C.; Chang, H.M. The role of micro-implant-assisted rapid palatal expansion (MARPE) in clinical orthodontics—A literature review. Australas. Orthod. J. 2021, 37, 206–216. [Google Scholar] [CrossRef]
- Suri, L.; Taneja, P. Surgically assisted rapid palatal expansion: A literature review. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 290–302. [Google Scholar] [CrossRef]
- Carvalho, P.H.A.; Moura, L.B.; Trento, G.S.; Holzinger, D.; Gabrielli, M.A.C.; Gabrielli, M.F.R.; Pereira Filho, V.A. Surgically assisted rapid maxillary expansion: A systematic review of complications. Int. J. Oral. Maxillofac. Surg. 2020, 49, 325–332. [Google Scholar] [CrossRef]
- Lee, K.J.; Park, Y.C.; Park, J.Y.; Hwang, W.S. Miniscrew-assisted nonsurgical palatal expansion before orthognathic surgery for a patient with severe mandibular prognathism. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 830–839. [Google Scholar] [CrossRef]
- Moon, W. An interview with Won Moon. By Andre Wilson Machado, Barry Briss, Greg J Huang, Richard Kulbersh and Sergei Godeiro Fernandes Rabelo Caldas. Dent. Press J. Orthod. 2013, 18, 12–28. [Google Scholar] [CrossRef] [Green Version]
- Kapetanovic, A.; Theodorou, C.I.; Berge, S.J.; Schols, J.; Xi, T. Efficacy of Miniscrew-Assisted Rapid Palatal Expansion (MARPE) in late adolescents and adults: A systematic review and meta-analysis. Eur. J. Orthod. 2021, 43, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Brunetto, D.P.; Sant’Anna, E.F.; Machado, A.W.; Moon, W. Non-surgical treatment of transverse deficiency in adults using Microimplant-assisted Rapid Palatal Expansion (MARPE). Dental Press J. Orthod. 2017, 22, 110–125. [Google Scholar] [CrossRef] [Green Version]
- Liao, Y.C.; Ho, K.H.; Wang, C.W.; Wang, K.L.; Hsieh, S.C.; Chang, H.M. Skeletal and dental changes after microimplant-assisted rapid palatal expansion (MARPE)—A Cephalometric and Cone-Beam Computed Tomography (CBCT) study. Clin. Investig. Orthod. 2022, 81, 84–92. [Google Scholar] [CrossRef]
- Song, K.T.; Park, J.H.; Moon, W.; Chae, J.M.; Kang, K.H. Three-dimensional changes of the zygomaticomaxillary complex after mini-implant assisted rapid maxillary expansion. Am. J. Orthod. Dentofac. Orthop. 2019, 156, 653–662. [Google Scholar] [CrossRef]
- Yilmaz, A.; Arman-Ozcirpici, A.; Erken, S.; Polat-Ozsoy, O. Comparison of short-term effects of mini-implant-supported maxillary expansion appliance with two conventional expansion protocols. Eur. J. Orthod. 2015, 37, 556–564. [Google Scholar] [CrossRef] [Green Version]
- Akkaya, S.; Lorenzon, S.; Ucem, T.T. A comparison of sagittal and vertical effects between bonded rapid and slow maxillary expansion procedures. Eur. J. Orthod. 1999, 21, 175–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wertz, R.; Dreskin, M. Midpalatal suture opening: A normative study. Am. J. Orthod. 1977, 71, 367–381. [Google Scholar] [CrossRef]
- Chung, C.H.; Font, B. Skeletal and dental changes in the sagittal, vertical, and transverse dimensions after rapid palatal expansion. Am. J. Orthod. Dentofac. Orthop. 2004, 126, 569–575. [Google Scholar] [CrossRef]
- Ricketts, R.M.; Roth, R.H.; Chaconas, S.J.; Schulhof, R.J.; Engel, G.A. Orthodontic Diagnosis and Planning: Their Roles in Preventive and Rehabilitative Dentistry; Rocky Mountain/Communicators: Kittredge, CO, USA, 1982. [Google Scholar]
- Betts, N.J.; Vanarsdall, R.L.; Barber, H.D.; Higgins-Barber, K.; Fonseca, R.J. Diagnosis and treatment of transverse maxillary deficiency. Int. J. Adult Orthodon. Orthognath. Surg. 1995, 10, 75–96. [Google Scholar]
- Melsen, B. Palatal growth studied on human autopsy material. A histologic microradiographic study. Am. J. Orthod. 1975, 68, 42–54. [Google Scholar] [CrossRef]
- Chen, C.L.; Chen, C.H.; Pan, C.Y.; Chang, H.P.; Chen, P.H.; Tseng, Y.C. Cone beam computed tomographic analysis of the spatial limitation during mandibular arch distalization. BMC Med. Imaging 2020, 20, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.J.; Choi, T.H.; Baik, H.S.; Park, Y.C.; Lee, K.J. Mandibular posterior anatomic limit for molar distalization. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.J.; Moon, W.; Hong, C. Effects of monocortical and bicortical mini-implant anchorage on bone-borne palatal expansion using finite element analysis. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 887–897. [Google Scholar] [CrossRef] [Green Version]
- Miller, S.; Neuhaus, M.T.; Zimmerer, R.; Tavassol, F.; Gellrich, N.C.; Ptok, M.; Jungheim, M. Three-dimensional analysis of the velopharyngeal region in patients with cleft palate and healthy individuals. Surg. Radiol. Anat. 2020, 42, 1033–1042. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Park, Y.C.; Lee, K.J.; Lintermann, A.; Han, S.S.; Yu, H.S.; Choi, Y.J. Assessment of changes in the nasal airway after nonsurgical miniscrew-assisted rapid maxillary expansion in young adults. Angle Orthod. 2018, 88, 435–441. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Tang, H.; Liu, X.; Luo, Q.; Jiang, Z.; Martin, D.; Guo, J. Comparison of dimensions and volume of upper airway before and after mini-implant assisted rapid maxillary expansion. Angle Orthod. 2020, 90, 432–441. [Google Scholar] [CrossRef] [Green Version]
- Angelieri, F.; Cevidanes, L.H.; Franchi, L.; Goncalves, J.R.; Benavides, E.; McNamara, J.A., Jr. Midpalatal suture maturation: Classification method for individual assessment before rapid maxillary expansion. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 759–769. [Google Scholar] [CrossRef] [Green Version]
- Almaqrami, B.S.; Ngan, P.; Alhammadi, M.S.; Al-Somairi, M.A.; Xiong, H.; Hong, H. Three-dimensional craniofacial changes with maxillary expansion in young adult patients with different craniofacial morphology. APOS Trends Orthod. 2022. [Google Scholar] [CrossRef]
- Ghoneima, A.; Abdel-Fattah, E.; Hartsfield, J.; El-Bedwehi, A.; Kamel, A.; Kula, K. Effects of rapid maxillary expansion on the cranial and circummaxillary sutures. Am. J. Orthod. Dentofac. Orthop. 2011, 140, 510–519. [Google Scholar] [CrossRef] [Green Version]
- Cantarella, D.; Dominguez-Mompell, R.; Mallya, S.M.; Moschik, C.; Pan, H.C.; Miller, J.; Moon, W. Changes in the midpalatal and pterygopalatine sutures induced by micro-implant-supported skeletal expander, analyzed with a novel 3D method based on CBCT imaging. Prog. Orthod. 2017, 18, 34. [Google Scholar] [CrossRef]
- Tsai, H.R.; Ho, K.H.; Wang, C.W.; Wang, K.L.; Hsieh, S.C.; Chang, H.M. Evaluation of Patients’ Experiences after Microimplant-Assisted Rapid Palatal Expansion (MARPE) Treatment. Taiwan. J. Orthod. 2021, 33, 11–18. [Google Scholar]
- Elshebiny, T.; Palomo, J.M.; Baumgaertel, S. Anatomic assessment of the mandibular buccal shelf for miniscrew insertion in white patients. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Nucera, R.; Lo Giudice, A.; Bellocchio, A.M.; Spinuzza, P.; Caprioglio, A.; Perillo, L.; Matarese, G.; Cordasco, G. Bone and cortical bone thickness of mandibular buccal shelf for mini-screw insertion in adults. Angle Orthod. 2017, 87, 745–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.A.; Ahn, H.W.; Oh, S.H.; Park, K.H.; Kim, S.H.; Nelson, G. Evaluation of interradicular space, soft tissue, and hard tissue of the posterior palatal alveolar process for orthodontic mini-implant, using cone-beam computed tomography. Am. J. Orthod. Dentofac. Orthop. 2021, 159, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Yun, H.S.; Park, H.D.; Kim, D.H.; Park, Y.C. Soft-tissue and cortical-bone thickness at orthodontic implant sites. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Hur, J.S.; Kim, H.H.; Choi, J.Y.; Suh, S.H.; Baek, S.H. Investigation of the effects of miniscrew-assisted rapid palatal expansion on airflow in the upper airway of an adult patient with obstructive sleep apnea syndrome using computational fluid-structure interaction analysis. Korean J. Orthod. 2017, 47, 353–364. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| JR-JL | 82.2 mm |
|---|---|
| AG-GA | 117.7 mm |
| Maxillomandibular transverse discrepancy | 35.5 mm |
| Expected transverse difference (14 y/o) | 18 mm |
| Maxillomandibular transverse differential index | 17.5 mm |
| Norm. | Initial | Post-Expansion | Final | |
|---|---|---|---|---|
| Skeletal analysis | ||||
| SNA | 82+/−2° | 83 | 84 | 83.5 |
| SNB | 80+/−2° | 83 | 82 | 82 |
| ANB | 2+/−2° | 0 | 2 | 1.5 |
| SN-MP (Go-Gn) | 32+/−5° | 34.5 | 35.5 | 35 |
| Frankfort-mandibular angle (FMA) | 25+/−5° | 29.8 | 32 | 31 |
| Dental analysis | ||||
| U1-NA (mm) | 3.18~7.34 mm | 5.8 | 6.6 | 6.1 |
| U1-SN | 102.23~115.13° | 108 | 112 | 115 |
| L1-NB (mm) | 3.18~7.34 mm | 5.8 | 5.5 | 6.1 |
| L1-MP (Go-Gn) | 90.56~103.12° | 87 | 87 | 91 |
| Facial analysis | ||||
| E-line (U) | −2.93~0.41 mm | −3.5 | −1.6 | −1.1 |
| E-line (L) | −1.86~2.1 mm | 0 | 0 | 0 |
| Facial convexity (G-Sn-Pg’) | 4.34~15.84° | 7.2 | 10.5 | 8.2 |
| Questionnaire Related to Patient’s Experiences during Microimplant-Assisted Rapid Palatal Expansion (MARPE) | ||
|---|---|---|
| Yes/No Questions: | Yes | No |
| 1. Swelling or inflammation of palatal gingiva | ■ | □ |
| 2. Soft tissue impingement while expansion | ■ | □ |
| 3. Difficult in cleaning around device | □ | ■ |
| 4. Distortions of the device | □ | ■ |
| 5. Microimplant loosening | □ | ■ |
| 6. Epistaxis | □ | ■ |
| 7. Sinusitis | □ | ■ |
| 8. Failure of mid-palatal suture opening | □ | ■ |
| Open-ended question: | ||
| Any other problem encountered during treatment | □ | ■ |
| Maximum pain score using numerical rating scale (NRS): 1 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shih, S.-N.; Ho, K.-H.; Wang, C.-W.; Wang, K.-L.; Hsieh, S.-C.; Chang, H.-M. Management of Class III Malocclusion and Maxillary Transverse Deficiency with Microimplant-Assisted Rapid Palatal Expansion (MARPE): A Case Report. Medicina 2022, 58, 1052. https://doi.org/10.3390/medicina58081052
Shih S-N, Ho K-H, Wang C-W, Wang K-L, Hsieh S-C, Chang H-M. Management of Class III Malocclusion and Maxillary Transverse Deficiency with Microimplant-Assisted Rapid Palatal Expansion (MARPE): A Case Report. Medicina. 2022; 58(8):1052. https://doi.org/10.3390/medicina58081052
Chicago/Turabian StyleShih, Sin-Ni, Kwok-Hing Ho, Chih-Wei Wang, Kai-Long Wang, Shun-Chu Hsieh, and Heng-Ming Chang. 2022. "Management of Class III Malocclusion and Maxillary Transverse Deficiency with Microimplant-Assisted Rapid Palatal Expansion (MARPE): A Case Report" Medicina 58, no. 8: 1052. https://doi.org/10.3390/medicina58081052
APA StyleShih, S.-N., Ho, K.-H., Wang, C.-W., Wang, K.-L., Hsieh, S.-C., & Chang, H.-M. (2022). Management of Class III Malocclusion and Maxillary Transverse Deficiency with Microimplant-Assisted Rapid Palatal Expansion (MARPE): A Case Report. Medicina, 58(8), 1052. https://doi.org/10.3390/medicina58081052