
Obesity Paradox among Heart Failure with Reduced Ejection Fraction Patients: A Retrospective Cohort Study
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Statistical Analyses
3. Results
3.1. Baseline Demographic, Clinical and Biochemical Parameters
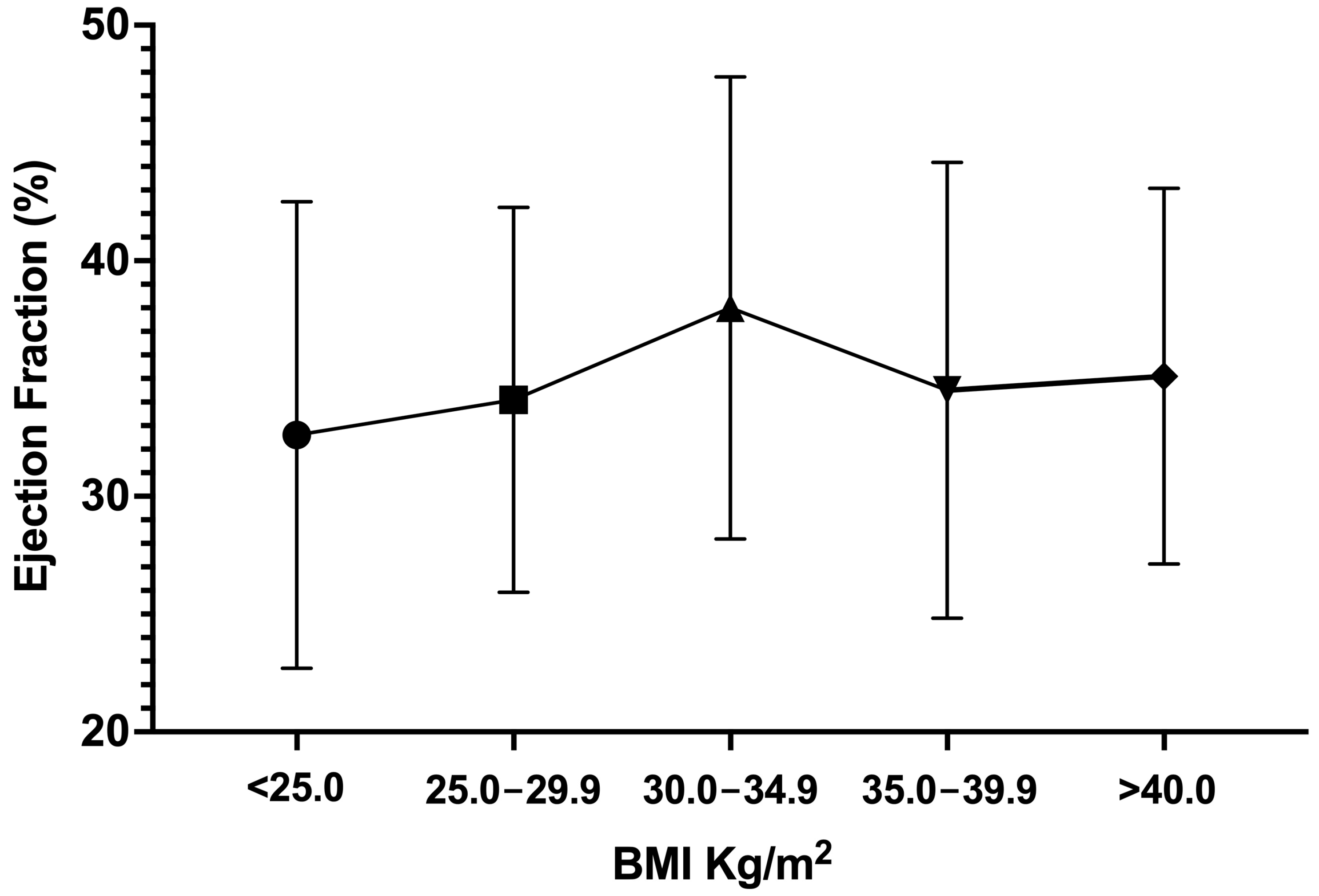
3.2. Changes in Cardiac Structure and Function after One Year
3.3. Effect of Diabetes Mellitus or Hypertension on Changes in EF
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maffetone, P.B.; Rivera-Dominguez, I.; Laursen, P.B. Overfat and Underfat: New Terms and Definitions Long Overdue. Front. Public Health 2016, 4, 279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Obesity and Overweight. Published 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 9 September 2022).
- Kenchaiah, S.; Evans, J.C.; Levy, D.; Wilson, P.W.; Benjamin, E.J.; Larson, M.G.; Kannel, W.B.; Vasan, R.S. Obesity and the Risk of Heart Failure. N. Engl. J. Med. 2002, 347, 305–313. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.; Metra, M.; Adamo, M.; Gardner, R.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Parto, P.; Lavie, C.J.; Arena, R.; Bond, S.; Popovic, D.; O Ventura, H. Body habitus in heart failure: Understanding the mechanisms and clinical significance of the obesity paradox. Futur. Cardiol. 2016, 12, 639–653. [Google Scholar] [CrossRef] [PubMed]
- Benn, M.; Marott, S.C.W.; Tybjaerg-Hansen, A.; Nordestgaard, B.G. Obesity increases heart failure incidence and mortality: Observational and Mendelian randomisation studies totalling over 1 million individuals. Cardiovasc. Res. 2021. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Prevalence of Overweight among Adults, BMI >= 25 (Age-Standardized Estimate) (%). Published 2022. Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/prevalence-of-overweight-among-adults-bmi-=-25-(age-standardized-estimate)-(-) (accessed on 9 September 2022).
- Horwich, T.B.; Fonarow, G.C.; Clark, A.L. Obesity and the Obesity Paradox in Heart Failure. Prog. Cardiovasc. Dis. 2018, 61, 151–156. [Google Scholar] [CrossRef]
- Horwich, T.B.; Fonarow, G.C.; Hamilton, M.A.; MacLellan, W.R.; Woo, M.A.; Tillisch, J.H. The relationship between obesity and mortality in patients with heart failure. J. Am. Coll. Cardiol. 2001, 38, 789–795. [Google Scholar] [CrossRef] [Green Version]
- Lavie, C.J.; Osman, A.F.; Milani, R.V.; Mehra, M.R. Body composition and prognosis in chronic systolic heart failure: The obesity paradox. Am. J. Cardiol. 2003, 91, 891–894. [Google Scholar] [CrossRef]
- Mosterd, A.; Cost, B.; Hoes, A.; De Bruijne, M.; Deckers, J.; Hofman, A.; Grobbee, D. The prognosis of heart failure in the general population. The Rotterdam Study. Eur. Hear. J. 2001, 22, 1318–1327. [Google Scholar] [CrossRef]
- Oreopoulos, A.; Padwal, R.; Kalantar-Zadeh, K.; Fonarow, G.C.; Norris, C.M.; McAlister, F.A. Body mass index and mortality in heart failure: A meta-analysis. Am. Hear. J. 2008, 156, 13–22. [Google Scholar] [CrossRef]
- Padwal, R.; A McAlister, F.; McMurray, J.J.V.; Cowie, M.R.; Rich, M.; Pocock, S.; Swedberg, K.; Maggioni, A.; Gamble, G.; Ariti, C.; et al. The obesity paradox in heart failure patients with preserved versus reduced ejection fraction: A meta-analysis of individual patient data. Int. J. Obes. 2014, 38, 1110–1114. [Google Scholar] [CrossRef] [PubMed]
- Curtis, J.P.; Selter, J.G.; Wang, Y.; Rathore, S.S.; Jovin, I.S.; Jadbabaie, F.; Kosiborod, M.; Portnay, E.L.; Sokol, S.I.; Bader, F.; et al. The obesity paradox: Body mass index and outcomes in patients with heart failure. Arch. Intern Med. 2005, 165, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Curtis, J.P.; Sokol, S.I.; Wang, Y.; Rathore, S.S.; Ko, D.T.; Jadbabaie, F.; Portnay, E.L.; Marshalko, S.J.; Radford, M.J.; Krumholz, H.M. The association of left ventricular ejection fraction, mortality, and cause of death in stable outpatients with heart failure. J. Am. Coll. Cardiol. 2003, 42, 736–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahajan, R.; Stokes, M.; Elliott, A.; A Munawar, D.; Khokhar, K.B.; Thiyagarajah, A.; Hendriks, J.; Linz, D.; Gallagher, C.; Kaye, D.; et al. Complex interaction of obesity, intentional weight loss and heart failure: A systematic review and meta-analysis. Heart 2020, 106, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Carime, N.A.; Cottenet, J.; Clerfond, G.; Eschalier, R.; Quilliot, D.; Eicher, J.; Joly, B.; Quantin, C. Correction: Impact of nutritional status on heart failure mortality: A retrospective cohort study. Nutr. J. 2022, 21, 61. [Google Scholar] [CrossRef]
- Gustafsson, F.; Kragelund, C.B.; Torp-Pedersen, C.; Seibæk, M.; Burchardt, H.; Akkan, D.; Thune, J.J.; Køber, L. Effect of obesity and being overweight on long-term mortality in congestive heart failure: Influence of left ventricular systolic function. Eur. Hear. J. 2005, 26, 58–64. [Google Scholar] [CrossRef]
- Hamzeh, N.; Ghadimi, F.; Farzaneh, R.; Hosseini, S.K. Obesity, Heart Failure, and Obesity Paradox. J. Tehran Heart Cent. 2017, 12, 1–5. [Google Scholar]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner–La Rocca, H.-P.; Choi, D.-J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Després, J.-P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. Obesity and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation 2021, 143, e984–e1010. [Google Scholar] [CrossRef]
- Elagizi, A.; Kachur, S.; Lavie, C.J.; Carbone, S.; Pandey, A.; Ortega, F.B.; Milani, R.V. An Overview and Update on Obesity and the Obesity Paradox in Cardiovascular Diseases. Prog. Cardiovasc. Dis. 2018, 61, 142–150. [Google Scholar] [CrossRef] [Green Version]
- Jamaly, S.; Carlsson, L.; Peltonen, M.; Jacobson, P.; Karason, K. Surgical obesity treatment and the risk of heart failure. Eur. Hear. J. 2019, 40, 2131–2138. [Google Scholar] [CrossRef]
- Karwi, Q.G.; Zhang, L.; Altamimi, T.R.; Wagg, C.S.; Patel, V.; Uddin, G.M.; Joerg, A.R.; Padwal, R.S.; Johnstone, D.E.; Sharma, A.; et al. Weight loss enhances cardiac energy metabolism and function in heart failure associated with obesity. Diabetes Obes. Metab. 2019, 21, 1944–1955. [Google Scholar] [CrossRef] [PubMed]
- Sankaralingam, S.; Alrob, O.A.; Zhang, L.; Jaswal, J.S.; Wagg, C.S.; Fukushima, A.; Padwal, R.S.; Johnstone, D.E.; Sharma, A.M.; Lopaschuk, G.D. Lowering Body Weight in Obese Mice With Diastolic Heart Failure Improves Cardiac Insulin Sensitivity and Function: Implications for the Obesity Paradox. Diabetes 2015, 64, 1643–1657. [Google Scholar] [CrossRef] [Green Version]
- Kenchaiah, S.; Pocock, S.J.; Wang, D.; Finn, P.; Zornoff, L.; Skali, H.; Pfeffer, M.; Yusuf, S.; Swedberg, K.; Michelson, E.; et al. Body mass index and prognosis in patients with chronic heart failure: Insights from the Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity (CHARM) program. Circulation 2007, 116, 627–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagarajan, V.; Kohan, L.; Holland, E.; Keeley, E.C.; Mazimba, S. Obesity paradox in heart failure: A heavy matter. ESC Hear. Fail. 2016, 3, 227–234. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Diabetes. Published 2022. Available online: https://www.who.int/health-topics/diabetes#tab=tab_1 (accessed on 15 September 2022).
- McMurray, J.J.V.; Gerstein, H.C.; Holman, R.R.; A Pfeffer, M. Heart failure: A cardiovascular outcome in diabetes that can no longer be ignored. Lancet Diabetes Endocrinol. 2014, 2, 843–851. [Google Scholar] [CrossRef]
- Nichols, G.A.; Hillier, T.A.; Erbey, J.R.; Brown, J.B. Congestive heart failure in type 2 diabetes: Prevalence, incidence, and risk factors. Diabetes Care 2001, 24, 1614–1619. [Google Scholar] [CrossRef] [Green Version]
- Echouffo-Tcheugui, J.B.; Xu, H.; DeVore, A.D.; Schulte, P.J.; Butler, J.; Yancy, C.W.; Bhatt, D.L.; Hernandez, A.F.; Heidenreich, P.A.; Fonarow, G.C. Temporal trends and factors associated with diabetes mellitus among patients hospitalized with heart failure: Findings from Get With The Guidelines–Heart Failure registry. Am. Hear. J. 2016, 182, 9–20. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, M.; Wang, S.; Li, N.; Zhang, S.; Tang, S.; Shi, Q.; Zhao, Y.; Li, J.; Zeng, Y.; et al. Diabetes in Patients With Heart Failure With Reduced Ejection Fraction During Hospitalization: A Retrospective Observational Study. Front. Endocrinol. 2021, 12, 727188. [Google Scholar] [CrossRef]
- Lu, Y.Y.; Wu, V.C.C.; Chu, P.-H.; Ho, C.-T.; Chang, C.-Y. Association between body mass index and survival in Taiwanese heart failure patients with and without diabetes mellitus. Medicine 2021, 100, e28114. [Google Scholar] [CrossRef]
- Lee, K.S.; Moser, D.K.; Lennie, T.A.; Pelter, M.M.; Nesbitt, T.; Southard, J.A.; Dracup, K. Obesity Paradox: Comparison of Heart Failure Patients With and Without Comorbid Diabetes. Am. J. Crit. Care 2017, 26, 140–148. [Google Scholar] [CrossRef]
- Kannel, W.B.; Hjortland, M.; Castelli, W.P. Role of diabetes in congestive heart failure: The Framingham study. Am. J. Cardiol. 1974, 34, 29–34. [Google Scholar] [CrossRef]
- Childers, D.K.; Allison, D.B. The ‘obesity paradox’: A parsimonious explanation for relations among obesity, mortality rate and aging? Int. J. Obes. 2010, 34, 1231–1238. [Google Scholar] [CrossRef] [Green Version]
- Messerli, F.H.; Rimoldi, S.F.; Bangalore, S. The Transition From Hypertension to Heart Failure: Contemporary Update. JACC Heart Fail. 2017, 5, 543–551. [Google Scholar] [CrossRef]
- Arundel, C.; Lam, P.H.; Gill, G.S.; Patel, S.; Panjrath, G.; Faselis, C.; White, M.; Morgan, C.J.; Allman, R.M.; Aronow, W.S.; et al. Systolic Blood Pressure and Outcomes in Patients With Heart Failure With Reduced Ejection Fraction. J. Am. Coll. Cardiol. 2019, 73, 3054–3063. [Google Scholar] [CrossRef]
- Lee, T.T.; Chen, J.; Cohen, D.J.; Tsao, L. The association between blood pressure and mortality in patients with heart failure. Am. Hear. J. 2006, 151, 76–83. [Google Scholar] [CrossRef]
- Rouleau, J.L.; Roecker, E.B.; Tendera, M.; Mohacsi, P.; Krum, H.; A Katus, H.; Fowler, M.B.; Coats, A.S.; Castaigne, A.; Scherhag, A.; et al. Influence of pretreatment systolic blood pressure on the effect of carvedilol in patients with severe chronic heart failure: The Carvedilol Prospective Randomized Cumulative Survival (COPERNICUS) study. J. Am. Coll. Cardiol. 2004, 43, 1423–1429. [Google Scholar] [CrossRef]
- Faselis, C.; Lam, P.H.; Zile, M.R.; Bhyan, P.; Tsimploulis, A.; Arundel, C.; Patel, S.; Kokkinos, P.; Deedwania, P.; Bhatt, D.L.; et al. Systolic Blood Pressure and Outcomes in Older Patients with HFpEF and Hypertension. Am. J. Med. 2021, 134, e252–e263. [Google Scholar] [CrossRef]
- Alpert, M.A.; Lambert, C.R.; Terry, B.E.; Cohen, M.V.; Mulekar, M.; Massey, C.V.; Hashimi, M.; Panayiotou, H.; Mukerji, V. Effect of weight loss on left ventricular diastolic filling in morbid obesity. Am. J. Cardiol. 1995, 76, 1198–1201. [Google Scholar] [CrossRef]
- Alpert, M.A.; Terry, B.E.; Mulekar, M.; Cohen, M.V.; Massey, C.V.; Fan, T.; Panayiotou, H.; Mukerji, V. Cardiac Morphology and Left Ventricular Function in Normotensive Morbidly Obese Patients with and without Congestive Heart Failure, and Effect of Weight Loss. Am. J. Cardiol. 1997, 80, 736–740. [Google Scholar] [CrossRef]
- Lauer, M.S.; Anderson, K.M.; Kannel, W.B.; Levy, D. The Impact of Obesity on Left Ventricular Mass and Geometry. JAMA 1991, 266, 231–236. [Google Scholar] [CrossRef]


{kind=link}
| Variable | All Patients | BMI Categories | p Value | |||||
|---|---|---|---|---|---|---|---|---|
| Less than 25 (n = 85, 28.6%) | 25–29.9 (n = 93, 31.3%) | 30–34.9 (n = 71, 23.9%) | 35–39.9 (n = 28, 9.4%) | ≥40 (n = 20, 6.7%) | ||||
| Gender | Male | 195 (65.7%) | 67 (34.4%) | 64 (68.8%) | 43 (22.1%) | 10 (5.1%) | 11 (5.6%) | <0.001 |
| Female | 102 (34.3%) | 18 (17.6%) | 29 (31.2%) | 28 (27.5%) | 18 (17.6%) | 9 (8.8%) | ||
| Age: mean (SD) | 64.6 (12.44) | 64.8 (13.95) | 65.1 (11.71) | 65.8 (11.6) | 66.0 (11.05) | 55.4 (10.75) | 0.015 | |
| Co-morbidities | Diabetes Miletus | 243 (81.8%) | 68 (28%) | 79 (32.5%) | 56 (23%) | 25 (10.3%) | 15 (6.2%) | 0.581 |
| Hypertension | 241 (81.1%) | 72 (29.9%) | 73 (30.3%) | 59 (24.5%) | 22 (9.1%) | 15 (6.2%) | 0.753 | |
| Ischemic Heart Disease | 87 (29.3%) | 18 (20.7%) | 33 (37.9%) | 24 (27.6%) | 8 (9.2%) | 4 (4.6%) | 0.204 | |
| Chronic Kidney Disease | 83 (27.9%) | 29 (34.9%) | 26 (31.3%) | 18 (21.7%) | 7 (8.4%) | 3 (3.6%) | 0.462 | |
| Dyslipidemia | 58 (19.5%) | 13 (22.4%) | 16 (27.6%) | 21 (36.2%) | 5 (8.6%) | 3 (5.2%) | 0.189 | |
| Lab values | Systolic Blood Pressure | 127.9 (22.59) | 125.0 (20.87) | 126.7 (19.68) | 128.8 (24.33) | 134.6 (24.17) | 132.4 (31.73) | 0.288 |
| Diastolic Blood Pressure | 76.0 (13.56) | 74.1 (11.99) | 75.6 (11.78) | 74.9 (13.26) | 80.8 (15.39) | 82.6 (21.74) | 0.015 | |
| Total Cholesterol | 3.5 (1.24) | 3.6 (1.14) | 3.3 (1.06) | 3.8 (1.47) | 3.2 (1.23) | 2.7 (0.98) | 0.244 | |
| Triglyceride | 1.6 (1.17) | 1.5 (1.08) | 1.5 (0.89) | 1.9 (1.64) | 1.4 (0.56) | 1.6 (1.09) | 0.591 | |
| Low Density Lipoprotein (LDL) | 2.2 (0.94) | 2.3 (0.91) | 2.1 (0.83) | 2.3 (1.07) | 2.0 (0.99) | 1.5 (0.68) | 0.318 | |
| High Density Lipoprotein (HDL) | 0.87 (0.32) | 0.92 (0.32) | 0.86 (0.31) | 0.90 (0.32) | 0.84 (0.38) | 0.67 (0.23) | 0.413 | |
| HbA1c | 7.8 (2.28) | 7.6 (2.19) | 7.9 (2.38) | 8.0 (2.33) | 7.2 (1.87) | 8.9 (2.45) | 0.172 | |
| Creatinine | 186.0 (142.69) | 167.7 (142.68) | 222.5 (166.43) | 160.3 (93.93) | 183.0 (133.04) | 189.5 (157.85) | 0.648 | |
| Urea | 15.9 (10.50) | 13.9 (9.82) | 16.7 (11.28) | 16.0 (9.88) | 18.4 (9.05) | 16.6 (12.90) | 0.263 | |
| EF | 34.4 (6.13) | 33.2 (6.60) | 34.6 (5.83) | 34.8 (6.35) | 35.6 (5.54) | 35.8 (5.09) | 0.595 | |
| LVWT | 1.11 (0.07) | 1.10 (0.04) | 1.10 (0.10) | 1.10 (0.07) | 1.10 (0.05) | 1.12 (0.04) | 0.995 | |
| Ejection Fraction (Time 1) Mean (SD) | Ejection Fraction (Time 2) Mean (SD) | p Value | LVWT (Time 1) Mean (SD) | LVWT (Time 2) Mean (SD) | p Value | ||
|---|---|---|---|---|---|---|---|
| All patients | 34.4 (6.13) | 34.7 (9.38) | 0.557 | 1.11 (0.08) | 1.12 (0.09) | 0.062 | |
| BMI groups | Less than 25 | 33.2 (6.60) | 32.6 (9.90) | 0.507 | 1.10 (0.04) | 1.12 (0.07) | 0.045 |
| 25–29.9 | 34.6 (5.82) | 34.1 (8.17) | 0.463 | 1.13 (0.10) | 1.12 (0.20) | 0.200 | |
| 30–34.9 | 34.8 (6.35) | 38.0 (9.81) | 0.004 | 1.11 (0.07) | 1.12 (0.07) | 0.096 | |
| 35–39.9 | 35.6 (5.54) | 34.5 (9.67) | 0.472 | 1.10 (0.05) | 1.14 (0.06) | 0.059 | |
| ≥40 | 35.8 (5.09) | 35.1 (7.97) | 0.595 | 1.12 (0.04) | 1.12 (0.05) | 1.000 | |
| Ejection Fraction Changes Across Different BMI Categories Mean (SD) | p Value | ||||||
|---|---|---|---|---|---|---|---|
| Less than 25 (n = 85, 28.6%) | 25–29.9 (n = 93, 31.3%) | 30–34.9 (n = 71, 23.9%) | 35–39.9 (n = 28, 9.4%) | ≥40 (n = 20, 6.7%) | |||
| Diabetes | Diabetic (n = 243) | −0.4 (7.66) | −1.1 (7.37) | 2.0 (8.92) | −1.2 (8.47) | −0.9 (6.08) | 0.211 |
| Non-Diabetic (n= 54) | −1.0 (7.83) | 2.4 (8.48) | 7.7 (7.89) | −0.3 (3.21) | 0 (2.74) | 0.033 | |
| Hypertension | Hypertensive (n = 241) | −0.3 (7.49) | −0.2 (7.83) | 3.7 (9.20) | −1.3 (8.60) | −0.7 (6.10) | 0.020 |
| Non-hypertensive (n = 56) | −0.2 (8.66) | −1.8 (6.76) | 0.7 (7.58) | −0.3 (6.12) | −0.6 (2.97) | 0.861 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alrob, O.A.; Sankaralingam, S.; Alazzam, S.; Nusairat, B.; Qattoum, M.; Nusair, M.B. Obesity Paradox among Heart Failure with Reduced Ejection Fraction Patients: A Retrospective Cohort Study. Medicina 2023, 59, 60. https://doi.org/10.3390/medicina59010060
Alrob OA, Sankaralingam S, Alazzam S, Nusairat B, Qattoum M, Nusair MB. Obesity Paradox among Heart Failure with Reduced Ejection Fraction Patients: A Retrospective Cohort Study. Medicina. 2023; 59(1):60. https://doi.org/10.3390/medicina59010060
Chicago/Turabian StyleAlrob, Osama Abo, Sowndramalingam Sankaralingam, Sayer Alazzam, Buthaina Nusairat, Muhammad Qattoum, and Mohammad B. Nusair. 2023. "Obesity Paradox among Heart Failure with Reduced Ejection Fraction Patients: A Retrospective Cohort Study" Medicina 59, no. 1: 60. https://doi.org/10.3390/medicina59010060
APA StyleAlrob, O. A., Sankaralingam, S., Alazzam, S., Nusairat, B., Qattoum, M., & Nusair, M. B. (2023). Obesity Paradox among Heart Failure with Reduced Ejection Fraction Patients: A Retrospective Cohort Study. Medicina, 59(1), 60. https://doi.org/10.3390/medicina59010060