Effects of Transcutaneous Electrical Nervous Stimulation (TENS) on Dysphonic Patients: A Systematic Review Study

 ,
,  ,
,
Abstract
:1. Background
2. Materials and Methods
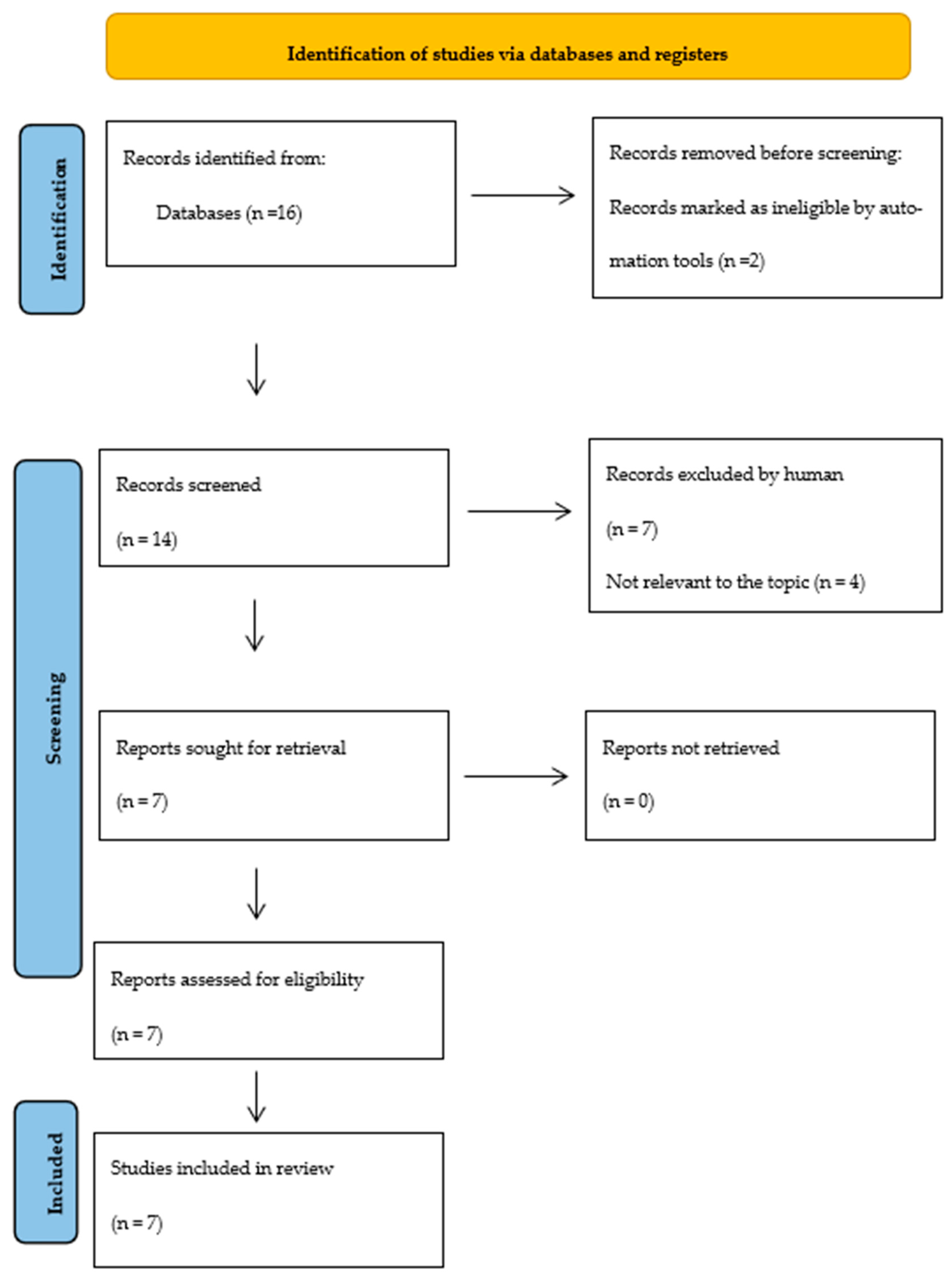
2.1. Study Design and Research Strategies
2.2. Eligibility Criteria and Data Extraction
2.3. Methodological Evaluation

{kind=link}
{kind=link}
| Study | Title | Sample | Age | Gender | Study Type |
|---|---|---|---|---|---|
| [7] | Effects of laryngeal manual therapy (LMT) and transcutaneous electrical nerve stimulation (TENS) in vocal folds diadochokinesis of dysphonic women: a randomized clinical trial | Women with bilateral vocal nodules participated | 18–45 | 20 Female | Randomized clinical trial |
| [1] | Effect of Vocal Therapy Associated with TENS in Women with Behavioral Dysphonia | Women with behavioral dysphonia | Average 46.1 (±15.1) years | 17 Female | Clinical trial |
| [17] | Effects of transcutaneous electrical nervous stimulation (TENS) associated with vocal therapy on musculoskeletal pain of women with behavioral dysphonia: A randomized, placebo-controlled double-blind clinical trial | Women with behavioral dysphonia | Average (ΕΚ) 29 and Average (ΚΓ) 31.6 | 27 Female | A randomized, placebo-controlled, double-blind clinical trial |
| [4] | Effect of Application of Transcutaneous Electrical Nerve Stimulation and Laryngeal Manual Therapy in Dysphonic Women: Clinical Trial | Women with bilateral vocal nodules participated | 18–45 | 20 Female | Clinical trial |
| [2] | Evaluation of Electrostimulation Effect in Women with Vocal Nodules | Women with an otolaryngology diagnosis of vocal fold nodules using a videolaryngostroboscopy examination | 18–55 | 60 Female | Randomized, prospective, comparative, intra-subject study |
| [18] | Transcutaneous Electrical Nerve Stimulation (TENS) and Laryngeal Manual Therapy (LMT): Immediate Effects in Women with Dysphonia | Women with behavioral dysphonia | 18–45 | 30 Female | Clinical trial |
| [8] | Application of High-Frequency Transcutaneous Electrical Nerve Stimulation in Muscle Tension Dysphonia Patients with the Pain Complaint: The Immediate Effect | Patients with muscle tension dysphonia (MTD) | Average 36.40 (±5.76 years) | 20 Female 10 male | Clinical trial |
3. Results
3.1. Application Methods of TENS
3.2. Assessment Methods
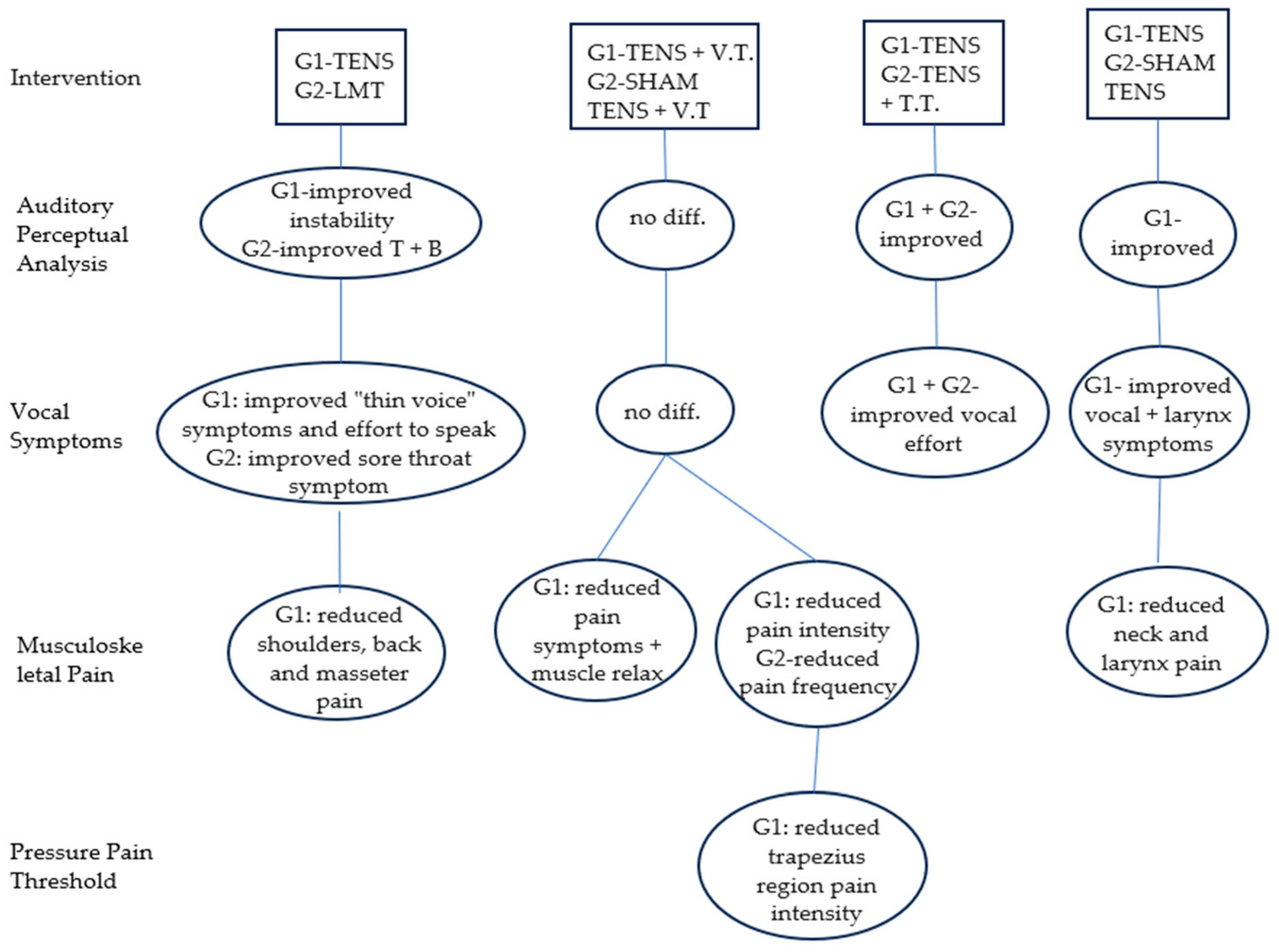
3.3. Outcome Measures
3.4. Quality of Studies
4. Discussion
5. Conclusions
6. Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Almeida, A.N.S.; da Cunha, D.A.; Duarte, B.F.; Guimarães, B.T.d.L.; Lucena, J.A.; Pernambuco, L.d.A.; Paes, M.C.N.d.M.; da Cunha, M.D.; Balata, P.M.M.; da Silva, H.J. Effect of Vocal Therapy Associated With TENS in Women With Behavioral Dysphonia. J. Voice 2022, 36, 585.e27–585.e37. [Google Scholar] [CrossRef] [PubMed]
- Santos, J.K.d.O.; Silvério, K.C.A.; Oliveira, N.F.C.D.; Gama, A.C.C. Evaluation of Electrostimulation Effect in Women with Vocal Nodules. J. Voice 2016, 30, 769.e1–769.e7. [Google Scholar] [CrossRef] [PubMed]
- Šiupšinskienė, N.; Adamonis, K.; Toohill, R.J.; Šiupšinskienė, N. Usefulness of assessment of voice capabilities in female patients with reflux-related dysphonia. Medicina 2009, 45, 978. [Google Scholar] [CrossRef] [PubMed]
- Alves Silverio, K.C.; Brasolotto, A.G.; Thaís Donalonso Siqueira, L.; Carneiro, C.G.; Fukushiro, A.P.; Roberto de Jesus Guirro, R. Effect of Application of Transcutaneous Electrical Nerve Stimulation and Laryngeal Manual Therapy in Dysphonic Women: Clinical Trial. J. Voice 2015, 29, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Stemple, J.C.; Roy, N.; Klaben, B.K. Clinical Voice Pathology: Theory and Management; Plural Publishing: San Diego, CA, USA, 2018. [Google Scholar]
- Lin, F.C.; Chien, H.Y.; Kao, Y.C.; Wang, C.T. Multi-dimensional investigation of the clinical effectiveness and prognostic factors of voice therapy for benign voice disorders. J. Formos. Med. Assoc. 2022, 121, 329–334. [Google Scholar] [CrossRef]
- Siqueira, L.T.D.; Silverio, K.C.A.; Brasolotto, A.G.; Guirro, R.R.D.J.; Carneiro, C.G.; Behlau, M. Effects of laryngeal manual therapy (LMT) and transcutaneous electrical nerve stimulation (TENS) in vocal folds diadochokinesis of dysphonic women: A randomized clinical trial. Codas 2017, 29, e20160191. [Google Scholar]
- Mansuri, B.; Torabinezhad, F.; Jamshidi, A.A.; Dabirmoghadam, P.; Vasaghi-Gharamaleki, B.; Ghelichi, L. Application of high-frequency transcutaneous electrical nerve stimulation in muscle tension dysphonia patients with the pain complaint: The immediate effect. J. Voice 2020, 34, 657–666. [Google Scholar] [CrossRef]
- Yensen, J. PICO search strategies. Online J. Nurs. Inform. 2013, 17, 2–8. Available online: http://ojni.org/issues/?p=2860 (accessed on 2 August 2023).
- Eriksen, M.B.; Frandsen, T.F. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: A systematic review. J. Med. Libr. Assoc. 2018, 106, 420–431. [Google Scholar] [CrossRef]
- Jensen, K.A. Seven Steps to the Perfect PICO Search. Evidence-Based Nursing Practice EBSCO Health-CINAHL Recuperado de. Available online: https://www.ebsco.com/blogs/health-notes/seven-steps-perfect-pico-search (accessed on 7 July 2023).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Institute for Musculoskeletal Health. Australia: School of Public Health, University of Sydney, Institute for Musculoskeletal Health. 1999 [cited 2023 Aug 2]. PEDro: Physiotherapy Evidence Database. Available online: https://www.pedro.org.au (accessed on 2 August 2023).
- De Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef]
- Verhagen, A.P.; de Vet, H.C.; de Bie, R.A.; Kessels, A.G.; Boers, M.; Bouter, L.M.; Knipschild, P.G. The Delphi List: A Criteria List for Quality Assessment of Randomized Clinical Trials for Conducting Systematic Reviews Developed by Delphi Consensus. J. Clin. Epidemiol. 1998, 51, 1235–1241. [Google Scholar] [CrossRef]
- Paci, M.; Bianchini, C.; Baccini, M. Reliability of the PEDro scale: Comparison between trials published in predatory and non-predatory journals. Arch. Physiother. 2022, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, L.T.D.; Ribeiro, V.V.; Moreira, P.A.M.; Brasolotto, A.G.; de Jesus Guirro, R.R.; Alves Silverio, K.C. Effects of transcutaneous electrical nervous stimulation (TENS) associated with vocal therapy on musculoskeletal pain of women with behavioral dysphonia: A randomized, placebo-controlled double-blind clinical trial. J. Commun. Disord. 2019, 82, 105923. [Google Scholar] [CrossRef] [PubMed]
- Conde, M.D.C.M.; Siqueira, L.T.D.; Vendramini, J.E.; Brasolotto, A.G.; de Jesus Guirro, R.R.; Silverio, K.C.A. Transcutaneous Electrical Nerve Stimulation (TENS) and Laryngeal Manual Therapy (LMT): Immediate effects in women with dysphonia. J. Voice 2018, 32, 385-e17. [Google Scholar] [CrossRef] [PubMed]
- Dejonckere, P.H. Gender Differences in the Prevalence of Occupational Voice Disorders. Occupational Voice: Care and Cure; Kugler Publications: The Hague, The Netherlands, 2001; pp. 11–20. [Google Scholar]
- Robb, M.; Gilbert, H.; Lerman, J. Influence of gender and environmental setting on voice onset time. Folia Phoniatr. Logop. 2005, 57, 125–133. [Google Scholar] [CrossRef]
- Dos Santos, A.P.; Silverio, K.C.A.; Dassie-Leite, A.P.; da Conceição Costa, C.; Siqueira, L.T.D. Relation between musculoskeletal pain and voice self-assessment in tele-operators. J. Voice 2019, 33, 948-e11. [Google Scholar] [CrossRef]
- Silverio, K.C.A.; Siqueira, L.T.D.; Lauris, J.R.P.; Brasolotto, A.G. Muscleskeletal pain in dysphonic women. In Codas; Sociedade Brasileira de Fonoaudiologia: São Paulo, Brazil, 2014; pp. 374–381. [Google Scholar]
- Rubin, J.S.; Blake, E.; Mathieson, L. Musculoskeletal patterns in patients with voice disorders. J. Voice 2007, 21, 477–484. [Google Scholar] [CrossRef]
- Rosen, C.A.; Murry, T. Nomenclature of voice disorders and vocal pathology. Otolaryngol. Clin. N. Am. 2000, 33, 1035–1045. [Google Scholar] [CrossRef]
- Won, S.J.; Kim, R.B.; Kim, J.P.; Park, J.J.; Kwon, M.S.; Woo, S.H. The prevalence and factors associate with vocal nodules in general population: Cross-sectional epidemiological study. Medicine 2016, 95, e4971. [Google Scholar] [CrossRef]
- Herrington-Hall, B.L.; Lee, L.; Stemple, J.C.; Niemi, K.R.; McHone, M.M. Description of laryngeal pathologies by age, sex, and occupation in a treatment-seeking sample. J. Speech Hear. Disord. 1988, 53, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Sluka, K.A.; Walsh, D. Transcutaneous electrical nerve stimulation: Basic science mechanisms and clinical effectiveness. J. Pain 2003, 4, 109–121. [Google Scholar] [CrossRef] [PubMed]
- Stangherlin, D.A.C.; Lemos, I.D.O.; Bello, J.Z.; Cassol, M. Transcutaneous Electrical Nerve Stimulation in Dysphonic Patients: A Systematic Review. J. Voice 2021, 35, 876–885. [Google Scholar] [CrossRef] [PubMed]
- Kuorinka, I.; Jonsson, B.; Kilbom, A.; Vinterberg, H.; Biering-Sørensen, F.; Andersson, G.; Jørgensen, K. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl. Ergon. 1987, 18, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Jensen, K.; Andersen, H.Ø.; Olesen, J.; Lindblom, U. Pressure-pain threshold in human temporal region. Evaluation of a new pressure algometer. Pain 1986, 25, 313–323. [Google Scholar] [CrossRef]
- Chaudhuri, K.R.; Martinez-Martin, P.; Schapira, A.H.V.; Stocchi, F.; Sethi, K.; Odin, P.; Brown, R.G.; Koller, W.; Barone, P.; Macphee, G.; et al. International multicenter pilot study of the first comprehensive self-completed nonmotor symptoms questionnaire for Parkinson’s disease: The NMSQuest study. Mov. Disord. 2006, 21, 916–923. [Google Scholar] [CrossRef]
- Garaycochea, O.; Navarrete, J.M.A.; Del Río, B.; Fernández, S. Muscle tension dysphonia: Which laryngoscopic features can we rely on for diagnosis? J. Voice 2019, 33, 812-e15. [Google Scholar] [CrossRef]
- Van Houtte, E.; Van Lierde, K.; Claeys, S. Pathophysiology and treatment of muscle tension dysphonia: A review of the current knowledge. J. Voice 2011, 25, 202–207. [Google Scholar] [CrossRef]
- Verdolini, K.; Rosen, C.A.; Branski, R.C. Classification Manual for Voice Disorders-I; Psychology Press: London, UK, 2014. [Google Scholar]
| Study | Device | Frequency | Pulse Width | Time | Location of the Electrodes | Types of Electrodes |
|---|---|---|---|---|---|---|
| [7] | Dualpex 961 | 10 Hz | 200 μs | 20 min | Trapezius muscle region (descending fibers) and submandibular region, bilaterally | 2 pairs (3.0 cm × 4.0 cm) |
| [1] | Ibramed Neurodyn III Amethyst Line | 15 Hz | 250 μs | 30 min | On clean skin, positioned on the upper border, at the level of the hyoid bone, and on the lower border, below the cricoid cartilage, one centimeter apart from one another | 1 pair (3 cm × 5 cm) |
| [17] | Quark Dualpex 961 | 10 Hz | 200 μs | 20 min | Trapezius muscle and submandibular area | 2 pairs (3 cm × 5 cm) |
| [4] | Dualpex 961 | 10 Hz | 200 μs | 20 min | Trapezius region—upper fibers, bilaterally, and in the submandibular region | 2 pairs (5.0 cm × 5.0 cm) |
| [2] | NEURODYN II | 10 Hz | 200 μs | 20 min | Lateral center of the larynx (thyroid cartilage) in the infrahyoid muscles, with 1 cm between them and on trapezius muscles | Rectangular and composed of silicon (30 × 50 mm) |
| [18] | Dualpex 961 | 10 Hz | 200 μs | 20 min | Trapezius muscle (on the descending fiber) and on both sides of the submandibular region | 2 pairs (5.0 cm × 4.0 cm) |
| [8] | ELPHA II 3000 | 100 Hz | 50 μs | 20 min | Lateral center of the thyroid cartilage in the infrahyoid muscles and the motor point of the trapezius muscle on the descending fiber | 2 pairs (5 cm × 5 cm) |
| [14] | [1] | [15] | [4] | [2] | [16] | [5] | |
|---|---|---|---|---|---|---|---|
| 1. Eligibility criteria | YES | YES | YES | YES | YES | YES | YES |
| 2. Randomized allocation | YES | YES | YES | YES | YES | YES | YES |
| 3. Secret allocation | YES | YES | YES | YES | YES | NO | YES |
| 4. Similarity of groups in prognosis | YES | YES | YES | YES | YES | YES | YES |
| 5. Blinding of all subjects | YES | NO | NO | YES | YES | YES | YES |
| 6. Blinding of all therapists | YES | YES | YES | YES | YES | YES | YES |
| 7. Blinding of assessors | YES | YES | YES | YES | YES | YES | YES |
| 8. Measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups | NO | NO | YES | YES | YES | YES | YES |
| 9. Analysis of “intention to treat” | NO | NO | NO | NO | NO | NO | NO |
| 10. Between-group statistical comparisons | YES | YES | YES | YES | YES | YES | YES |
| 11. Precision and variability measures | YES | YES | YES | YES | YES | YES | YES |
| Total Points | 8/10 | 8/10 | 8/10 | 9/10 | 9/10 | 8/10 | 9/10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plotas, P.; Papadopoulos, A.; Tsiamaki, E.; Apostolou, M.-D.; Chaniotaki, M.-A.; Ganiatsou, E.; Goutzeri, E.-M.; Kalogeraki, T.; Karra, E.; Malliou, M.; et al. Effects of Transcutaneous Electrical Nervous Stimulation (TENS) on Dysphonic Patients: A Systematic Review Study. Medicina 2023, 59, 1737. https://doi.org/10.3390/medicina59101737
Plotas P, Papadopoulos A, Tsiamaki E, Apostolou M-D, Chaniotaki M-A, Ganiatsou E, Goutzeri E-M, Kalogeraki T, Karra E, Malliou M, et al. Effects of Transcutaneous Electrical Nervous Stimulation (TENS) on Dysphonic Patients: A Systematic Review Study. Medicina. 2023; 59(10):1737. https://doi.org/10.3390/medicina59101737
Chicago/Turabian StylePlotas, Panagiotis, Angelos Papadopoulos, Eirini Tsiamaki, Maria-Dimitra Apostolou, Maria-Antonia Chaniotaki, Efthimia Ganiatsou, Eleni-Marianthi Goutzeri, Thalia Kalogeraki, Elpida Karra, Maria Malliou, and et al. 2023. "Effects of Transcutaneous Electrical Nervous Stimulation (TENS) on Dysphonic Patients: A Systematic Review Study" Medicina 59, no. 10: 1737. https://doi.org/10.3390/medicina59101737