
Neurosurgical Education Using Cadaver-Free Brain Models and Augmented Reality: First Experiences from a Hands-On Simulation Course for Medical Students
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
4.1. UpSurgeOn—Product Range and Costs
4.2. Previous Validation Studies Using UpSurgeOn Simulators
4.3. The Role of Medical Student Education in Neurosurgery
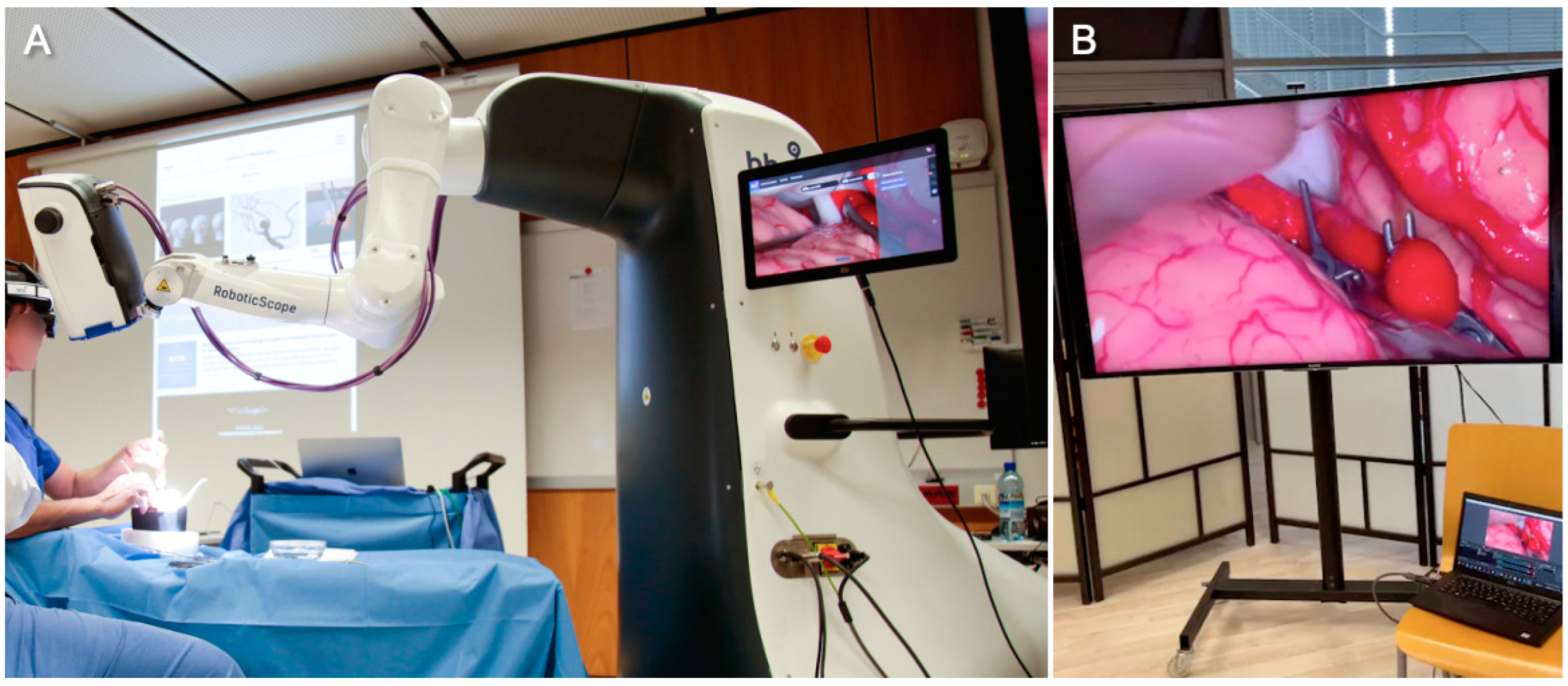
4.4. RoboticScope
4.5. Limitations of Our Study
4.6. Outlook
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stienen, M.N.; Freyschlag, C.F.; Schaller, K.; Meling, T.; For the EANS Young Neurosurgeons and EANS Training Committee. Procedures performed during neurosurgery residency in Europe. Acta Neurochir. 2020, 162, 2303–2311. [Google Scholar] [CrossRef] [PubMed]
- Rehder, R.; Abd-El-Barr, M.; Hooten, K.; Weinstock, P.; Madsen, J.R.; Cohen, A.R. The role of simulation in neurosurgery. Childs Nerv. Syst. 2016, 32, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Baby, B.; Singh, R.; Suri, A.; Dhanakshirur, R.R.; Chakraborty, A.; Kumar, S.; Kalra, P.K.; Banerjee, S. A review of virtual reality simulators for neuroendoscopy. Neurosurg. Rev. 2020, 43, 1255–1272. [Google Scholar] [CrossRef]
- Baby, B.; Singh, R.; Singh, R.; Suri, A.; Arora, C.; Kumar, S.; Kalra, P.K.; Banerjee, S. A Review of Physical Simulators for Neuroendoscopy Skills Training. World Neurosurg. 2020, 137, 398–407. [Google Scholar] [CrossRef] [PubMed]
- Farah, G.J.; Rogers, J.L.; Lopez, A.M.; Brown, N.J.; Pennington, Z.; Kuo, C.; Gold, J.; Bui, N.E.; Koester, S.W.; Gendreau, J.L.; et al. Resident Training in Spine Surgery: A Systematic Review of Simulation-Based Educational Models. World Neurosurg. 2023, 174, 81–115. [Google Scholar] [CrossRef] [PubMed]
- Harrop, J.; Lobel, D.A.; Bendok, B.; Sharan, A.; Rezai, A.R. Developing a Neurosurgical Simulation-Based Educational Curriculum: An Overview. Neurosurgery 2013, 73, S25–S29. [Google Scholar] [CrossRef] [PubMed]
- Winkler-Schwartz, A.; Bajunaid, K.; Mullah, M.A.S.; Marwa, I.; Alotaibi, F.E.; Fares, J.; Baggiani, M.; Azarnoush, H.; Zharni, G.A.; Christie, S.; et al. Bimanual Psychomotor Performance in Neurosurgical Resident Applicants Assessed Using NeuroTouch, a Virtual Reality Simulator. J. Surg. Educ. 2016, 73, 942–953. [Google Scholar] [CrossRef]
- Petrone, S.; Cofano, F.; Nicolosi, F.; Spena, G.; Moschino, M.; Di Perna, G.; Lavorato, A.; Lanotte, M.M.; Garbossa, D. Virtual-Augmented Reality and Life-Like Neurosurgical Simulator for Training: First Evaluation of a Hands-On Experience for Residents. Front. Surg. 2022, 9, 862948. [Google Scholar] [CrossRef]
- Newall, N.; Khan, D.Z.; Hanrahan, J.G.; Booker, J.; Borg, A.; Davids, J.; Nicolosi, F.; Sinha, S.; Dorward, N.; Marcus, H.J. High fidelity simulation of the endoscopic transsphenoidal approach: Validation of the UpSurgeOn TNS Box. Front. Surg. 2022, 9, 1049685. [Google Scholar] [CrossRef]
- Robertson, F.C.; Stapleton, C.J.; Coumans, J.-V.C.E.; Nicolosi, F.; Vooijs, M.; Blitz, S.; Guerrini, F.; Spena, G.; Giussani, C.; Zoia, C.; et al. Applying objective metrics to neurosurgical skill development with simulation and spaced repetition learning. J. Neurosurg. 2023, 11, 3378. [Google Scholar] [CrossRef]
- Zuckerman, S.L.; Mistry, A.M.; Hanif, R.; Chambless, L.B.; Neimat, J.S.; Wellons, J.C.; Mocco, J.; Sills, A.K.; McGirt, M.J.; Thompson, R.C. Neurosurgery Elective for Preclinical Medical Students: Early Exposure and Changing Attitudes. World Neurosurg. 2016, 86, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Efe, I.E.; Aliyeva, I.; Beyaztas, D.; Swiatek, V.M.; Esene, I.N.; Abdulrauf, S.I. Gender Differences in Perceptions and Attitudes of Medical Students toward Neurosurgery: A German Nationwide Survey. World Neurosurg. 2022, 163, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Aboud, E.; Abolfotoh, M.; Pravdenkova, S.; Gokoglu, A.; Gokden, M.; Al-Mefty, O. Giant intracranial epidermoids: Is total removal feasible? J. Neurosurg. 2015, 122, 743–756. [Google Scholar] [CrossRef] [PubMed]
- Lv, X.; Li, C.; Jiang, W. The intracranial vasculature of canines represents a model for neurovascular ischemia and training residents and fellows in endovascular neurosurgery. Neuroradiol. J. 2020, 33, 292–296. [Google Scholar] [CrossRef]
- Mashiko, T.; Kaneko, N.; Konno, T.; Otani, K.; Nagayama, R.; Watanabe, E. Training in Cerebral Aneurysm Clipping Using Self-Made 3-Dimensional Models. J. Surg. Educ. 2017, 74, 681–689. [Google Scholar] [CrossRef] [PubMed]
- Joseph, F.J.; Weber, S.; Raabe, A.; Bervini, D. Neurosurgical simulator for training aneurysm microsurgery—A user suitability study involving neurosurgeons and residents. Acta Neurochir. 2020, 162, 2313–2321. [Google Scholar] [CrossRef] [PubMed]
- Licci, M.; Thieringer, F.M.; Guzman, R.; Soleman, J. Development and validation of a synthetic 3D-printed simulator for training in neuroendoscopic ventricular lesion removal. Neurosurg. Focus 2020, 48, E18. [Google Scholar] [CrossRef]
- Ramirez, M.D.J.E.; Nurmukhametov, R.; Musa, G.; Barrientos Castillo, R.E.; Encarnacion, V.L.A.; Soriano Sanchez, J.A.; Vazquez, C.A.; Efe, I.E. Three-Dimensional Plastic Modeling on Bone Frames for Cost-Effective Neuroanatomy Teaching. Cureus 2022, 14, e27472. [Google Scholar] [CrossRef]
- UpSurgeOn Store. Available online: https://store.upsurgeon.com/product-category/neurosurgery/ (accessed on 14 July 2023).
- Simpson, J.S. An Economical Approach to Teaching Cadaver Anatomy. Am. Biol. Teach. 2014, 76, 42–46. [Google Scholar] [CrossRef]
- Ahmed, R.; Muirhead, W.; Williams, S.C.; Bagchi, B.; Datta, P.; Gupta, P.; Salvadores Fernandez, C.; Funnell, J.P.; Hanrahan, J.G.; Davids, J.D.; et al. A synthetic model simulator for intracranial aneurysm clipping: Validation of the UpSurgeOn AneurysmBox. Front. Surg. 2023, 10, 1185516. [Google Scholar] [CrossRef]
- Williams, S.C.; Ahmed, R.; Davids, J.D.; Funnell, J.P.; Hanrahan, J.G.; Layard Horsfall, H.; Muirhead, W.; Nicolosi, F.; Thorne, L.; Marcus, H.J.; et al. Benchtop simulation of the retrosigmoid approach: Validation of a surgical simulator and development of a task-specific outcome measure score. World Neurosurg. X 2023, 20, 100230. [Google Scholar] [CrossRef] [PubMed]
- Sansosti, A.A.; Jacobs, R.C.; Safonova, A.; Jani, R.H.; Schumann, J.; Friedlander, R.M.; Lunsford, L.D.; McDowell, M.M.; Sekula, R.F. Impact of a Hands-on Pre-Clinical Neurosurgery Elective Course on Second-Year Medical Student Interest and Attitudes. J. Med. Educ. Curric. Dev. 2020, 7, 238212052096485. [Google Scholar] [CrossRef] [PubMed]
- Atli, K.; Selman, W.; Ray, A. A Comprehensive Multicomponent Neurosurgical Course with use of Virtual Reality: Modernizing the Medical Classroom. J. Surg. Educ. 2021, 78, 1350–1356. [Google Scholar] [CrossRef]
- Takoutsing, B.D.; Wunde, U.N.; Zolo, Y.; Endalle, G.; Djaowé, D.A.M.; Tatsadjieu, L.S.N.; Zourmba, I.M.; Dadda, A.; Nchufor, R.N.; Nkouonlack, C.D.; et al. Assessing the impact of neurosurgery and neuroanatomy simulation using 3D non-cadaveric models amongst selected African medical students. Front. Med. Technol. 2023, 5, 1190096. [Google Scholar] [CrossRef] [PubMed]
- Nicolosi, F.; Rossini, Z.; Zaed, I.; Kolias, A.G.; Fornari, M.; Servadei, F. Neurosurgical digital teaching in low-middle income countries: Beyond the frontiers of traditional education. Neurosurg. Focus 2018, 45, E17. [Google Scholar] [CrossRef] [PubMed]
- Greuter, L.; De Rosa, A.; Cattin, P.; Croci, D.M.; Soleman, J.; Guzman, R. Randomized study comparing 3D virtual reality and conventional 2D on-screen teaching of cerebrovascular anatomy. Neurosurg. Focus 2021, 51, E18. [Google Scholar] [CrossRef] [PubMed]
- Aitzetmüller, M.M.; Klietz, M.-L.; Dermietzel, A.F.; Hirsch, T.; Kückelhaus, M. Robotic-Assisted Microsurgery and Its Future in Plastic Surgery. J. Clin. Med. 2022, 11, 3378. [Google Scholar] [CrossRef]
- Zhang, J.; Fang, Q.; Xiang, P.; Sun, D.; Xue, Y.; Jin, R.; Qiu, K.; Xiong, R.; Wang, Y.; Lu, H. A Survey on Design, Actuation, Modeling, and Control of Continuum Robot. Cyborg Bionic Syst. 2022, 2022, 9754697. [Google Scholar] [CrossRef]
- Peters, B.S.; Armijo, P.R.; Krause, C.; Choudhury, S.A.; Oleynikov, D. Review of emerging surgical robotic technology. Surg. Endosc. 2018, 32, 1636–1655. [Google Scholar] [CrossRef]
- Mo, H.; Li, X.; Ouyang, B.; Fang, G.; Jia, Y. Task Autonomy of a Flexible Endoscopic System for Laser-Assisted Surgery. Cyborg Bionic Syst. 2022, 2022, 9759504. [Google Scholar] [CrossRef]
- Boehm, F.; Schuler, P.J.; Riepl, R.; Schild, L.; Hoffmann, T.K.; Greve, J. Performance of microvascular anastomosis with a new robotic visualization system: Proof of concept. J. Robot. Surg. 2022, 16, 705–713. [Google Scholar] [CrossRef] [PubMed]
- Piloni, M.; Bailo, M.; Gagliardi, F.; Mortini, P. Resection of Intracranial Tumors with a Robotic-Assisted Digital Microscope: A Preliminary Experience with Robotic Scope. World Neurosurg. 2021, 152, e205–e211. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1. Which year of study are you in? |
| 2. How many neuroanatomical cadaver dissections have you performed in the past? |
| 3. How many craniotomies have you performed on either cadavers or patients? |
| 4. Have you worked or are you currently working in the operating room, pathology/anatomy institute or any other area dealing with patients or cadavers? If yes, please specify. |
| 5. The Neurosurgery App and the AR simulator help develop neuroanatomical orientation skills needed during a neurosurgical approach. |
| 6. After using this model, I feel more familiar in the use of neurosurgical instruments. |
| 7. After using this model, I feel more familiar in the use of the surgical microscope/exoscope. |
| 8. The sequence of mental training (app), hybrid training (augmented reality) and manual training (BrainBox) is an effective method of training to fill the gap between theoretical knowledge and practice on a real patient/cadaver. |
| 9. Using this model helps to increase familiarity and to acquire neurosurgical skills. |
| 10. This method should be part of the curriculum (during internship and residency), in addition to traditional training methods. |
| 11. This course solidified my decision to pursue neurosurgery. |
| 12. My overall learning experience was: |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Efe, I.E.; Çinkaya, E.; Kuhrt, L.D.; Bruesseler, M.M.T.; Mührer-Osmanagic, A. Neurosurgical Education Using Cadaver-Free Brain Models and Augmented Reality: First Experiences from a Hands-On Simulation Course for Medical Students. Medicina 2023, 59, 1791. https://doi.org/10.3390/medicina59101791
Efe IE, Çinkaya E, Kuhrt LD, Bruesseler MMT, Mührer-Osmanagic A. Neurosurgical Education Using Cadaver-Free Brain Models and Augmented Reality: First Experiences from a Hands-On Simulation Course for Medical Students. Medicina. 2023; 59(10):1791. https://doi.org/10.3390/medicina59101791
Chicago/Turabian StyleEfe, Ibrahim E., Emre Çinkaya, Leonard D. Kuhrt, Melanie M. T. Bruesseler, and Armin Mührer-Osmanagic. 2023. "Neurosurgical Education Using Cadaver-Free Brain Models and Augmented Reality: First Experiences from a Hands-On Simulation Course for Medical Students" Medicina 59, no. 10: 1791. https://doi.org/10.3390/medicina59101791