

A Simple Technique Using Peri-Prosthetic Irrigation Improves Implant Salvage Rates in Immediate Implant-Based Breast Reconstruction

Abstract
:1. Introduction
2. Methods
- Conventional technique:
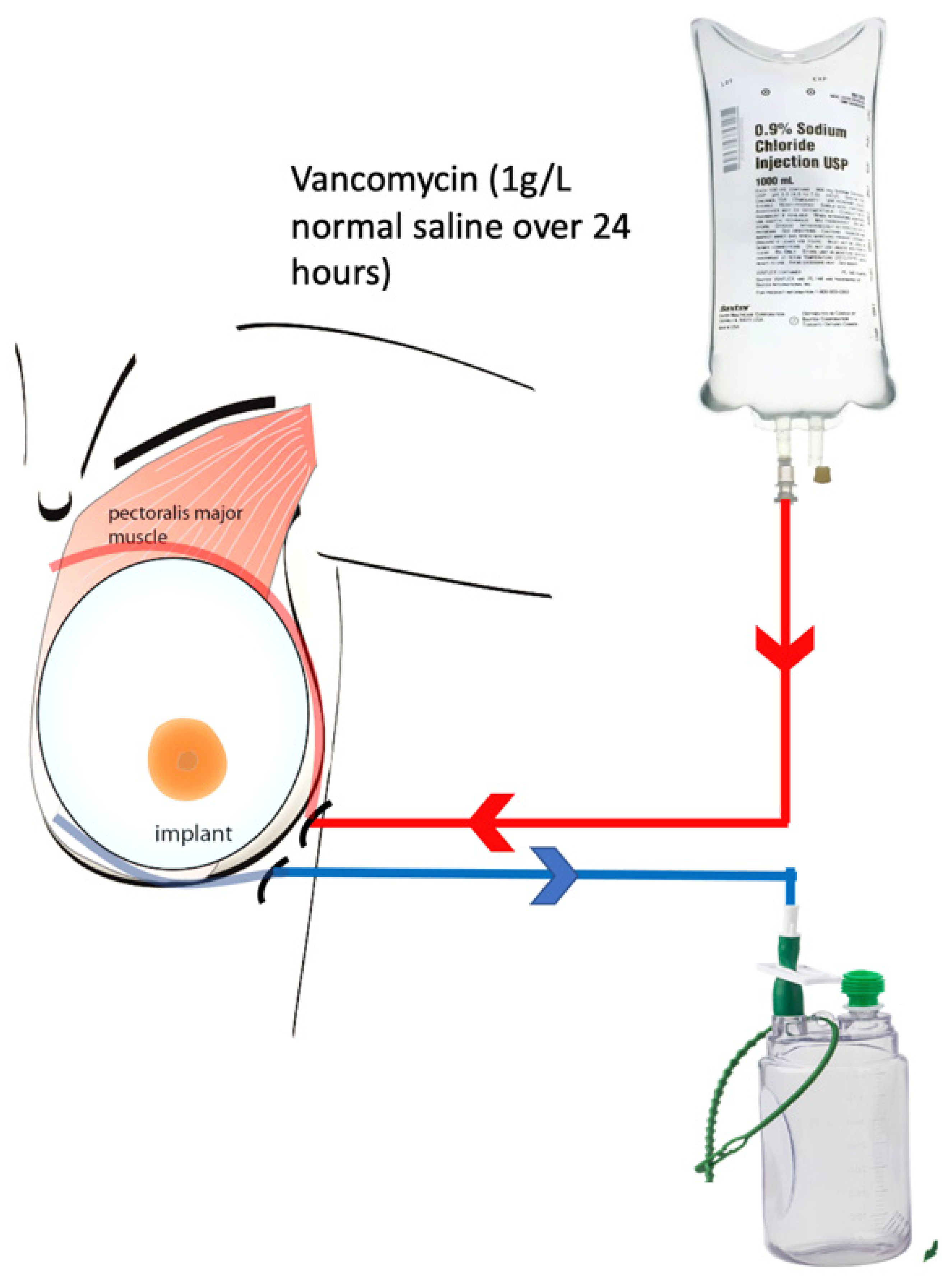
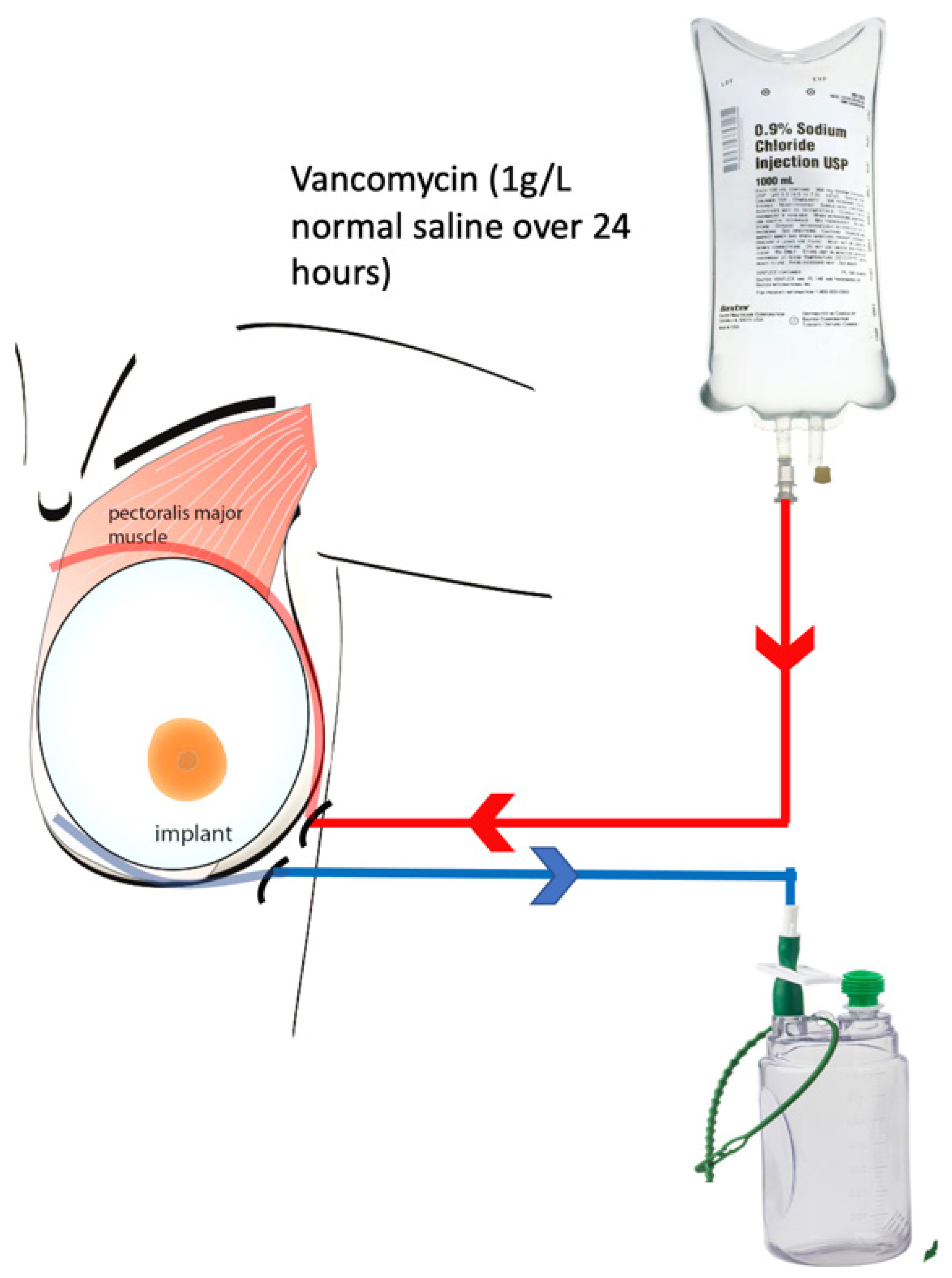
- Peri-prosthetic irrigation technique (PPI):
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arnold, M.; Morgan, E.; Rumgay, H.; Mafra, A.; Singh, D.; Laversanne, M.; Vignat, J.; Gralow, J.R.; Cardoso, F.; Siesling, S.; et al. Current and future burden of breast cancer: Global statistics for 2020 and 2040. Breast 2022, 66, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Breast Surgery. Getting It Right First Time—GIRFT. Available online: https://gettingitrightfirsttime.co.uk/surgical_specialties/breast-surgery/ (accessed on 4 July 2023).
- Ho, G.; Nguyen, T.J.; Shahabi, A.; Hwang, B.H.; Chan, L.S.; Wong, A.K. A systematic review and meta-analysis of complications associated with acellular dermal matrix-assisted breast reconstruction. Ann. Plast. Surg. 2012, 68, 346–356. [Google Scholar] [CrossRef]
- Potter, S.; Conroy, E.J.; Cutress, R.I.; Williamson, P.R.; Whisker, L.; Thrush, S.; Skillman, J.; Barnes, N.L.P.; Mylvaganam, S.; Teasdale, E.; et al. Short-term safety outcomes of mastectomy and immediate implant-based breast reconstruction with and without mesh (iBRA): A multicentre, prospective cohort study. Lancet Oncol. 2019, 20, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Jafferbhoy, S.; Chandarana, M.; Houlihan, M.; Parmeshwar, R.; Narayanan, S.; Soumian, S.; Harries, S.; Jones, L.; Clarke, D. Early multicentre experience of pre-pectoral implant based immediate breast reconstruction using Braxon®. Gland Surg. 2017, 6, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Bennett, S.; Fitoussi, A.; Berry, M.; Couturaud, B.; Salmon, R. Management of exposed, infected implant-based breast reconstruction and strategies for salvage. J. Plast. Reconstr. Aesthetic Surg. 2011, 64, 1270–1277. [Google Scholar] [CrossRef] [PubMed]
- Yii, N.-W.; Khoo, C.T.K. Salvage of infected expander prostheses in breast reconstruction. Plast. Reconstr. Surg. 2003, 111, 1087–1092. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.D.M.; Suber, J.S.M.; Aya-Ay, M.L.M.; Cone, J.D.J.M.; Greene, J.N.M.; Smith, D.J.J.M.; Smith, P.D.M. Prosthesis salvage in breast reconstruction patients with periprosthetic infection and exposure. Plast. Reconstr. Surg. 2012, 129, 42–48. [Google Scholar] [CrossRef]
- Chun, J.K.; Schulman, M.R. The infected breast prosthesis after mastectomy reconstruction: Successful salvage of nine implants in eight consecutive patients. Plast. Reconstr. Surg. 2007, 120, 581–589. [Google Scholar] [CrossRef]
- Reish, R.G.M.; Damjanovic, B.M.; Austen, W.G.J.M.; Winograd, J.M.; Liao, E.C.M.; Cetrulo, C.L.M.; Balkin, D.M.; Colwell, A.S.M. Infection following implant-based reconstruction in 1952 consecutive breast reconstructions: Salvage rates and predictors of success. Plast. Reconstr. Surg. 2013, 131, 1223–1230. [Google Scholar] [CrossRef]
- Burkhardt, B.R.; Dempsey, P.D.; Schnur, P.L.; Tofield, J.J. Capsular contracture: A prospective study of the effect of local antibacterial agents. Plast. Reconstr. Surg. 1986, 77, 919–930. [Google Scholar] [CrossRef]
- Brown, L.L.; Shelton, H.T.; Bornside, G.H.; Cohn, I. Evaluation of wound irrigation by pulsatile jet and conventional methods. Ann. Surg. 1978, 187, 170–173. [Google Scholar] [CrossRef]
- Bahrs, C.; Schnabel, M.; Frank, T.; Zapf, C.; Mutters, R.; von Garrel, T. Lavage of contaminated surfaces: An in vitro evaluation of the effectiveness of different systems. J. Surg. Res. 2003, 112, 26–30. [Google Scholar] [CrossRef]
- Sarfati, I.; Millochau, J.; Meredith, I.; Leroy, O.; Parra, R.V.; Romano, G.; Nos, C.; Clough, K.B. Salvaging the infected breast implant: Results of a retrospective series of 80 consecutive cases. J. Plast. Reconstr. Aesthetic Surg. 2020, 73, 2232–2238. [Google Scholar] [CrossRef]
- Albright, S.B.; Xue, A.S.; McKnight, A.; Wolfswinkel, E.M.; Hollier, L.H.; Brown, R.H.; Bullocks, J.M.; Izaddoost, S.A. One-Step Salvage of Infected Prosthetic Breast Reconstructions Using Antibiotic-Impregnated Polymethylmethacrylate Plates and Concurrent Tissue Expander Exchange. Ann. Plast. Surg. 2016, 77, 280–285. [Google Scholar] [CrossRef]
- Meybodi, F.M.; Sedaghat, N.B.; Elder, E.M.; French, J.M.; Adams, K.B.; Hsu, J.M.; Kanesalingam, K.M.; Brennan, M.F. Salvaging the Unsalvageable: Negative Pressure Wound Therapy for Severe Infection of Prosthetic Breast Reconstruction. Plast. Reconstr. Surg. Glob. Open 2021, 9, e3456. [Google Scholar] [CrossRef]
- Antognoli, L.E.; Singh, D.P.; Choudhry, S.; Turcotte, J.P.; Holton, L.H.I. Rinse But Don’t Repeat: Single Application V.A.C. VERAFLO Salvages Infected Breast Prostheses. Plast. Reconstr. Surg. Glob. Open 2021, 9, e3896. [Google Scholar] [CrossRef] [PubMed]
- Marcasciano, M.; Kaciulyte, J.; Di Giuli, R.; Marcasciano, F.; Torto, F.L.; Guerra, M.; Prà, G.D.; Barellini, L.; Mazzocchi, M.; Casella, D.; et al. “Just Pulse it!” Introduction of a conservative implant salvage protocol to manage infection in pre-pectoral breast reconstruction: Case series and literature review. J. Plast. Reconstr. Aesthetic Surg. 2021, 75, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Muthusami, A.; Green, M.; Brookes, P.; Kasana, I. P111: Breast implant salvage after postoperative infection—Successful new technique. Eur. J. Surg. Oncol. 2020, 46, e39. [Google Scholar] [CrossRef]
- Lapid, O. Use of gentamicin collagen sponges for the treatment of periprosthetic breast implant infection. J. Plast. Reconstr. Aesthetic Surg. 2011, 64, e313–e316. [Google Scholar] [CrossRef] [PubMed]
- Yeo, H.; Lee, D.; Kim, J.S.; Eo, P.S.; Kim, D.K.; Lee, J.S.; Kwon, K.T.; Lee, J.; Park, H.Y.; Yang, J.D. Strategy for salvaging infected breast implants: Lessons from the recovery of seven consecutive patients. Arch. Plast. Surg. 2021, 48, 165–174. [Google Scholar] [CrossRef]
- Sforza, M.; Andjelkov, K.; Husein, R.; Zaccheddu, R. Will 1-stage implant salvage after periprosthetic breast infection ever be routine? A 6-year successful experience. Aesthetic Surg. J. 2014, 34, 1172–1178. [Google Scholar] [CrossRef] [PubMed]
- De Waele, J.J.; Girardis, M.; Martin-Loeches, I. Source control in the management of sepsis and septic shock. Intensive Care Med. 2022, 48, 1799–1802. [Google Scholar] [CrossRef] [PubMed]
- Krueger, E.A.; Wilkins, E.G.; Strawderman, M.; Cederna, P.; Goldfarb, S.; Vicini, F.A.; Pierce, L.J. Complications and patient satisfaction following expander/implant breast reconstruction with and without radiotherapy. Int. J. Radiat. Oncol. 2001, 49, 713–721. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristic | Conventional Group (n = 38) | Peri-Prosthetic Irrigation Group (n = 7) | p-Value |
|---|---|---|---|
| Age | |||
| 1. Mean | 55 | 53 | 0.423 |
| 2. Median | 54 | 54 | |
| 3. Range | 37–68 | 44–62 | |
| Smoking status | |||
| 1. Yes | 2 | 1 | 0.379 |
| 2. No | 36 | 6 | |
| BMI | |||
| 1. Mean | 28 | 30 | 0.264 |
| 2. Median | 31 | 31 | |
| Indication for mastectomy | |||
| 1. Invasive cancer | 23 | 4 | 0.961 |
| 2. Ductal carcinoma in situ | 9 | 2 | |
| 3. Risk-reducing mastectomy | 6 | 1 | |
| Type of mastectomy | |||
| 1. Skin sparing mastectomy | 30 | 4 | 0.441 |
| 2. Nipple-sparing mastectomy | 6 | 2 | |
| 3. Skin reducing mastectomy | 2 | 1 | |
| Axillary surgery | |||
| 1. Sentinel lymph node biopsy | 28 | 4 | 0.431 |
| 2. Axillary nodal clearance | 4 | 2 | |
| 3. None | 6 | 1 | |
| Successful Implant salvage | 16 | 7 | 0.019 |
| Sl No. | Authors | Year | Salvage Technique | Success Rate |
|---|---|---|---|---|
| 1 | Our study | 2023 | Peri-prosthetic irrigation | 7/7 (100%) |
| 2 | Ngi-Wieh Yii [7] | 2003 | Capsule cavity scrubbed with iodine, then half-strength peroxide, followed by copious saline wash, capsulotomy, and implant exchange. Two drains, wound closed. Continuous saline and intermittent antibiotic irrigation through the drains. | 9/14 (64.28%) |
| 3 | Prince MD et al. [8] | 2012 | Broad spectrum antibiotics+ Early operation-curettage of necrotic tissue + Pulse lavage with 3L NS and 3L Antibiotics + Implant exchange | 33/43 (76.74%) |
| 4 | Jin K Chun [9] | 2007 | Intravenous antibiotics followed by drainage of fluid, manual debridement and curettage of the infected pocket, device exchange, and post-operative antibiotics. | 9/9 (100%) |
| 5 | Bennett et al. [6] | 2011 | Debridement + Capsulotomy +saline wash and either:
| 9/20 (45%) |
| 6 | Richard G Reish et al. [10] | 2013 | Intravenous antibiotics and implant exchange | 37/99 (37.3%) |
| 7 | I Sarfati et al. [14] | 2020 | Medical management with antibiotics Surgical management with wash-out and exchange of implant | 71/80 (88.8%) |
| 8 | S B Albright et al. [15] | 2016 | Debridement and antibiotic-loaded polymethylmethacrylate (PMMA) sheets and systemic antibiotics | 14/14 (100%) |
| 9 | F Meybodi et al. [16] | 2021 | Explant + negative pressure wound therapy(NPWT)/(V.A.C. VERAFLO). | 23/28 (83%) |
| 10 | Lauren E. Antognoli et al. [17] | 2021 | Explantation + debridement + wash-out of the breast pocket NPWT (V.A.C. VERAFLO) with Prontosan as an instillation solution. | 15/16 (93.75%) |
| 11 | M Marcasciano et al. [18] | 2022 | Pulse therapy using pulsavac | 8/5 (100%) |
| 12 | A Muthusami et al. [19] | 2020 | Removal of the implant and filling the cavity with a solution of gentamicin and saline. After 48 h, the cavity is explored, and a new implant is inserted. | 5/5 (100%) |
| 13 | O Lapid et al [20] | 2011 | Gentamicin collagen sponge | 4/4 (100%) |
| 14 | H Yeo et al. [21] | 2021 | Debridement + povidone-iodine/antibiotic lavage in the implant pocket + implant replacement | 7/8 (87.5%) |
| 15 | M Sforza et al. [22] | 2014 | Explant + Capsulotomy + Antibiotic scrub + Insertion of a new implant | 17/17 (100%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gowda, M.S.; Jafferbhoy, S.; Marla, S.; Narayanan, S.; Soumian, S. A Simple Technique Using Peri-Prosthetic Irrigation Improves Implant Salvage Rates in Immediate Implant-Based Breast Reconstruction. Medicina 2023, 59, 2039. https://doi.org/10.3390/medicina59112039
Gowda MS, Jafferbhoy S, Marla S, Narayanan S, Soumian S. A Simple Technique Using Peri-Prosthetic Irrigation Improves Implant Salvage Rates in Immediate Implant-Based Breast Reconstruction. Medicina. 2023; 59(11):2039. https://doi.org/10.3390/medicina59112039
Chicago/Turabian StyleGowda, Manoj Srinivas, Sadaf Jafferbhoy, Sekhar Marla, Sankaran Narayanan, and Soni Soumian. 2023. "A Simple Technique Using Peri-Prosthetic Irrigation Improves Implant Salvage Rates in Immediate Implant-Based Breast Reconstruction" Medicina 59, no. 11: 2039. https://doi.org/10.3390/medicina59112039
APA StyleGowda, M. S., Jafferbhoy, S., Marla, S., Narayanan, S., & Soumian, S. (2023). A Simple Technique Using Peri-Prosthetic Irrigation Improves Implant Salvage Rates in Immediate Implant-Based Breast Reconstruction. Medicina, 59(11), 2039. https://doi.org/10.3390/medicina59112039