

A Pilot Study of Autonomic Function Screening Tests for Differentiating Complex Regional Pain Syndrome Type II and Traumatic Neuropathic Pain


Abstract
:1. Introduction
2. Materials and Methods
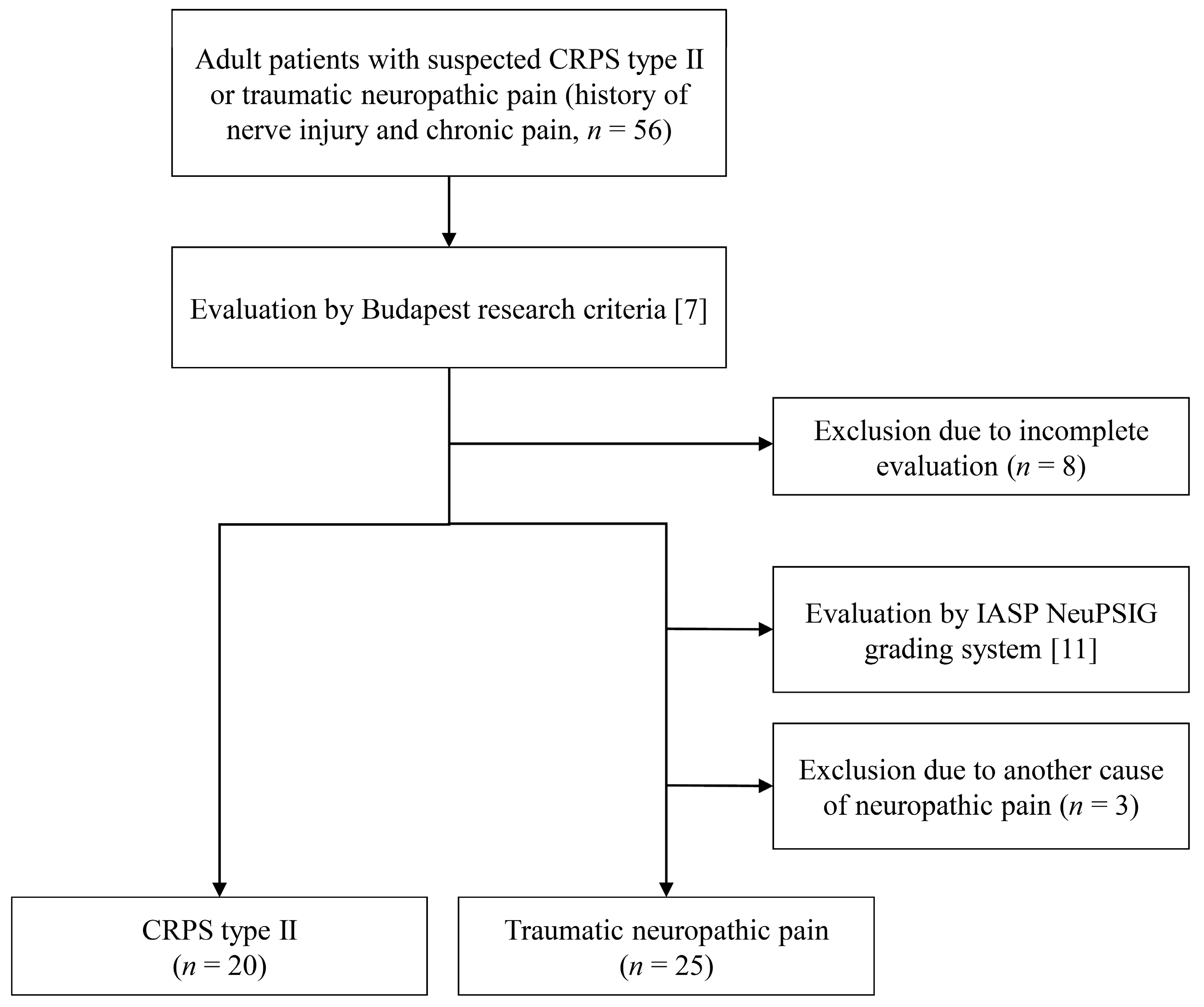
2.1. Study Design and Population
2.2. Diagnosis of CRPS Type II and Traumatic Neuropathic Pain
2.3. Autonomic Function Screening Test
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Preparation |
|
| Tests (Perform the following four tests in order) | |
| QSART |
|
| HRDB test |
|
| Valsalva maneuver |
|
| HUT test |
|
Appendix B
| Patient No. | Onset Age/Sex | Disease Duration (Months) | Affected Site | QSART | HUT Test | HRDB Test | Valsalva Maneuver | DITI | Three-Phase Bone Scan |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 43/M | 70 | Lower limb, R | Decreased on lower limb, R | N | Normal | N | N | N |
| 2 | 27/M | 91 | Upper limb, L | Decreased on upper limb, L | N | Normal | N | Hypothermia on upper limb, L | N |
| 3 | 24/M | 13 | Lower limb, R; Sacral area | Increased on whole limbs * | N | Decreased | N | Hypothermia on lower limb, R | Increased uptake on lower limb, R |
| 4 | 24/M | 11 | Lower limb, R | Decreased on lower limb, R | OH | Decreased | N | Hypothermia on lower limb, R | Increased uptake on lower limb, R |
| 5 | 28/M | 25 | Ankle, R | N | POTS | Normal | N | Hypothermia on ankle, R | ND |
| 6 | 52/M | 38 | Foot, L | Decreased on foot, L | N | N | N | Hypothermia on foot, L | Increased uptake on foot, L |
| 7 | 64/M | 15 | Upper limb, R | Decreased on upper and lower limb, R | N | N | N | Hypothermia on hand, L † | Increased uptake on upper limb, R |
| 8 | 26/F | 16 | Shoulder, L | Decreased on upper limb, L | N | Decreased | Decreased Valsalva ratio | Hypothermia on upper limb and shoulder, L * | N |
| 9 | 48/F | 50 | Foot, L | Decreased on foot, L | OH | N | N | Hypothermia on lower limb, L | N |
| 10 | 44/F | 14 | Hand, L | Decreased on lower limbs, R, L * | N | Decreased | N | Hypothermia on shoulder, L † | Increased uptake on hand, L |
| 11 | 58/F | 26 | Lower limb, R | Decreased on lower limb, R | POTS | N | N | Hypothermia on lower limb, R | Increased uptake on lower limb, R |
| 12 | 61/F | 13 | Upper limb, R | Increased on upper limbs, R, L * | N | N | N | Hypothermia on upper limb, R | Increased uptake on upper limb, R |
| 13 | 43/F | 30 | Upper limb, R | Decreased on upper limb, R | N | N | N | Hypothermia on upper limb, L † | Increased uptake on upper limb, R |
References
- Harden, R.N.; Bruehl, S.; Stanton-Hicks, M.; Wilson, P.R. Proposed New Diagnostic Criteria for Complex Regional Pain Syndrome. Pain Med. 2007, 8, 326–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harden, R.N.; Bruehl, S.; Perez, R.S.G.M.; Birklein, F.; Marinus, J.; Maihofner, C.; Lubenow, T.; Buvanendran, A.; MacKey, S.; Graciosa, J.; et al. Validation of Proposed Diagnostic Criteria (the “Budapest Criteria”) for Complex Regional Pain Syndrome. Pain 2010, 150, 268–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, A.; Yoo, M.; Calisoff, R. Complex Regional Pain Syndrome: An Updated Comprehensive Review. NeuroRehabilitation 2020, 47, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Arcidiacono, U.A.; Armocida, D.; Pesce, A.; Maiotti, M.; Proietti, L.; D’Andrea, G.; Santoro, A.; Frati, A. Complex Regional Pain Syndrome after Spine Surgery: A Rare Complication in Mini-Invasive Lumbar Spine Surgery: An Updated Comprehensive Review. J. Clin. Med. 2022, 11, 7409. [Google Scholar] [CrossRef] [PubMed]
- Birklein, F.; Dimova, V. Complex Regional Pain Syndrome–up-to-Date. Pain Rep. 2017, 2, e624. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.-S.; Noor, N.; Urits, I.; Paladini, A.; Sadhu, M.S.; Gibb, C.; Carlson, T.; Myrcik, D.; Varrassi, G.; Viswanath, O. Complex Regional Pain Syndrome: A Comprehensive Review. Pain Ther. 2021, 10, 875–892. [Google Scholar] [CrossRef] [PubMed]
- Galer, B.S.; Bruehl, S.; Harden, R.N. IASP Diagnostic Criteria for Complex Regional Pain Syndrome: A Preliminary Empirical Validation Study. Clin. J. Pain 1998, 14, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Harden, N.R.; Bruehl, S.; Galer, B.S.; Saltz, S.; Bertram, M.; Backonja, M.; Gayles, R.; Rudin, N.; Bhugra, M.K.; Stanton-Hicks, M. Complex Regional Pain Syndrome: Are the IASP Diagnostic Criteria Valid and Sufficiently Comprehensive? Pain 1999, 83, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Zygmunt, A.; Stanczyk, J. Methods of Evaluation of Autonomic Nervous System Function. Arch. Med. Sci. 2010, 1, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-J.; Kim, S.E.; Moon, J.Y.; Shin, J.-Y.; Kim, Y.-C. Analysis of Quantitative Sudomotor Axon Reflex Test Patterns in Patients with Complex Regional Pain Syndrome Diagnosed Using the Budapest Criteria. Reg. Anesth. Pain Med. 2019, 44, 1026–1032. [Google Scholar] [CrossRef] [PubMed]
- Finnerup, N.B.; Haroutounian, S.; Kamerman, P.; Baron, R.; Bennett, D.L.H.; Bouhassira, D.; Cruccu, G.; Freeman, R.; Hansson, P.; Nurmikko, T.; et al. Neuropathic Pain: An Updated Grading System for Research and Clinical Practice. Pain 2016, 157, 1599–1606. [Google Scholar] [CrossRef] [Green Version]
- Park, K.-J.; Lee, H.; Kim, H.A.; Kang, S.-Y.; Kim, B.J.; Nam, T.-S.; Sohn, E.H.; Oh, J.; Lee, T.-K. Guidelines for Autonomic Function Test. J. Pain Auton. Disord. 2013, 2, 55–65. [Google Scholar]
- Park, K.H.; Kim, B.J.; Kang, S.Y.; Oh, S.Y.; Sohn, E.H.; Song, K.J.; Shin, J.H.; Kang, K.H.; Kim, R.B.; Cho, E.B.; et al. Reference Range of Autonomic Function Test in Korean Healthy Adults. J. Pain Auton. Disord. 2017, 6, 6–10. [Google Scholar] [CrossRef] [Green Version]
- Knudsen, L.F.; Terkelsen, A.J.; Drummond, P.D.; Birklein, F. Complex Regional Pain Syndrome: A Focus on the Autonomic Nervous System. Clin. Auton. Res. 2019, 29, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Goh, E.L.; Chidambaram, S.; Ma, D. Complex Regional Pain Syndrome: A Recent Update. Burn. Trauma 2017, 5, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kortekaas, M.C.; Niehof, S.P.; Stolker, R.J.; Huygen, F.J.P.M. Pathophysiological Mechanisms Involved in Vasomotor Disturbances in Complex Regional Pain Syndrome and Implications for Therapy: A Review. Pain Pract. 2016, 16, 905–914. [Google Scholar] [CrossRef] [PubMed]
- Bartur, G.; Vatine, J.-J.; Raphaely-Beer, N.; Peleg, S.; Katz-Leurer, M. Heart Rate Autonomic Regulation System at Rest and During Paced Breathing among Patients with CRPS as Compared to Age-Matched Healthy Controls. Pain Med. 2014, 15, 1569–1574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terkelsen, A.J.; Mølgaard, H.; Hansen, J.; Finnerup, N.B.; Krøner, K.; Jensen, T.S. Heart Rate Variability in Complex Regional Pain Syndrome during Rest and Mental and Orthostatic Stress. Anesthesiology 2012, 116, 133–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.-J.; Lee, K.H.; Moon, J.Y.; Kim, Y.-C. Prevalence of Autonomic Nervous System Dysfunction in Complex Regional Pain Syndrome. Reg. Anesth. Pain Med. 2021, 46, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Thayer, J.F.; Yamamoto, S.S.; Brosschot, J.F. The Relationship of Autonomic Imbalance, Heart Rate Variability and Cardiovascular Disease Risk Factors. Int. J. Cardiol. 2010, 141, 122–131. [Google Scholar] [CrossRef] [PubMed]

| CRPS Type II (n = 20) | Traumatic Neuropathic Pain (n = 25) | p-Value | |
|---|---|---|---|
| Age * (years) | 40 ± 16.1 | 40 ± 14.0 | 0.87 |
| Sex † | 0.55 | ||
| Male | 13 (65.00) | 13 (52.00) | |
| Female | 7 (35.00) | 12 (48.00) | |
| BMI * (kg/m2) | 25.1 ± 3.00 | 24.0 ± 4.70 | 0.31 |
| Duration ‡ (years) | 3.0 (1.00–6.25) | 4.0 (3.00–6.50) | 0.27 |
| NRS * (0–10) | 7.5 ± 1.54 | 5.8 ± 1.85 | 0.001 § |
| Affected site † | |||
| Upper extremity | 8 (40.00) | 6 (24.00) | 0.34 |
| Lower extremity | 12 (60.00) | 15 (60.00) | 1.00 |
| Upper or lower | 0 (0.00) | 4 (16.00) | 0.12 |
| Bilateral symptom | 1 | 10 | 0.012 § |
| Psychiatric disorders † | 10 (50.00) | 4 (16.00) | 0.014 § |
| Etiology † | |||
| Contusion/laceration | 9 | 11 | 0.95 |
| Traffic accident | 2 | 7 | 0.26 |
| Surgery | 2 | 2 | 1.00 |
| Fracture | 2 | 1 | 0.58 |
| Combined ‖ | 5 | 4 | 0.48 |
| Medication † | |||
| Opioids | 19 (95.00) | 20 (80.00) | 0.21 |
| Anticonvulsants | 19 (95.00) | 22 (88.00) | 0.62 |
| Antidepressants | 16 (80.00) | 12 (48.00) | 0.035 § |
| CRPS Type II * (n = 20) | Traumatic Neuropathic Pain * (n = 25) | OR (95% CI) | p-Value | |
|---|---|---|---|---|
| Abnormal QSART | 12 (60.00) | 6 (24.00) | 4.750 (1.318, 17.113) | 0.017 † |
| Abnormal HRDB test | 4 (20.00) | 3 (12.00) | 1.833 (0.359, 9.353) | 0.466 |
| Abnormal Valsalva maneuver test | 1 (5.00) | 0 (0.00) | Inf (0, Inf) | 0.998 |
| Abnormal HUT test | 4 (20.00) | 0 (0.00) | Inf (0, Inf) | 0.998 |
| Univariable Model | Multivariable Model | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| CRPS type II | 4.750 (1.318, 17.113) | 0.017 * | 10.920 (1.251, 95.302) | 0.031 * |
| NRS | 1.010 (0.737, 1.385) | 0.949 | 0.738 (0.472, 1.1152) | 0.181 |
| BMI | 0.888 (0.758, 1.040) | 0.140 | 0.795 (0.638, 0.992) | 0.042 * |
| Antidepressants | 2.080 (0.578, 7.486) | 0.262 | 0.990 (0.158, 6.195) | 0.992 |
| Psychiatric disorders | 4.400 (0.059, 0.868) | 0.030 * | 3.245 (0.550, 19.141) | 0.194 |
| Bilateral symptom | 0.475 (0.107, 2.107) | 0.327 | 0.822 (0.121, 5.593) | 0.841 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.; Kim, M.J.; Kim, J.H.; Oh, J.; Choi, K. A Pilot Study of Autonomic Function Screening Tests for Differentiating Complex Regional Pain Syndrome Type II and Traumatic Neuropathic Pain. Medicina 2023, 59, 646. https://doi.org/10.3390/medicina59040646
Kim D, Kim MJ, Kim JH, Oh J, Choi K. A Pilot Study of Autonomic Function Screening Tests for Differentiating Complex Regional Pain Syndrome Type II and Traumatic Neuropathic Pain. Medicina. 2023; 59(4):646. https://doi.org/10.3390/medicina59040646
Chicago/Turabian StyleKim, Dayoung, Min Jung Kim, Jae Hun Kim, Jeeyoung Oh, and Kyomin Choi. 2023. "A Pilot Study of Autonomic Function Screening Tests for Differentiating Complex Regional Pain Syndrome Type II and Traumatic Neuropathic Pain" Medicina 59, no. 4: 646. https://doi.org/10.3390/medicina59040646
APA StyleKim, D., Kim, M. J., Kim, J. H., Oh, J., & Choi, K. (2023). A Pilot Study of Autonomic Function Screening Tests for Differentiating Complex Regional Pain Syndrome Type II and Traumatic Neuropathic Pain. Medicina, 59(4), 646. https://doi.org/10.3390/medicina59040646