
Injectable Resin Technique as a Restorative Alternative in a Cleft Lip and Palate Patient: A Case Report


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
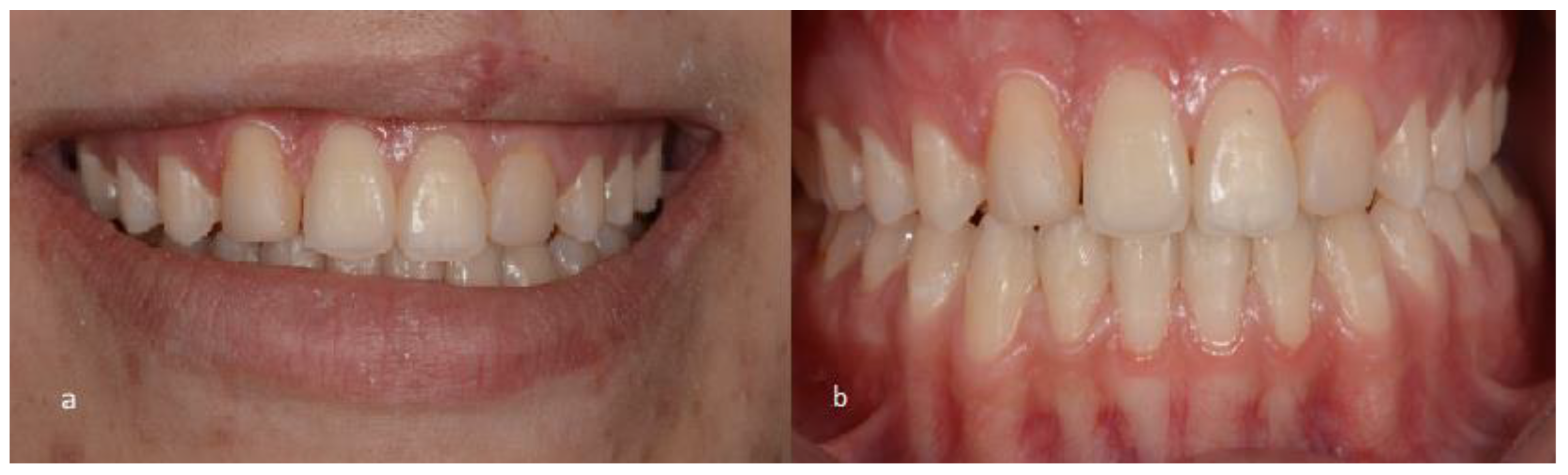
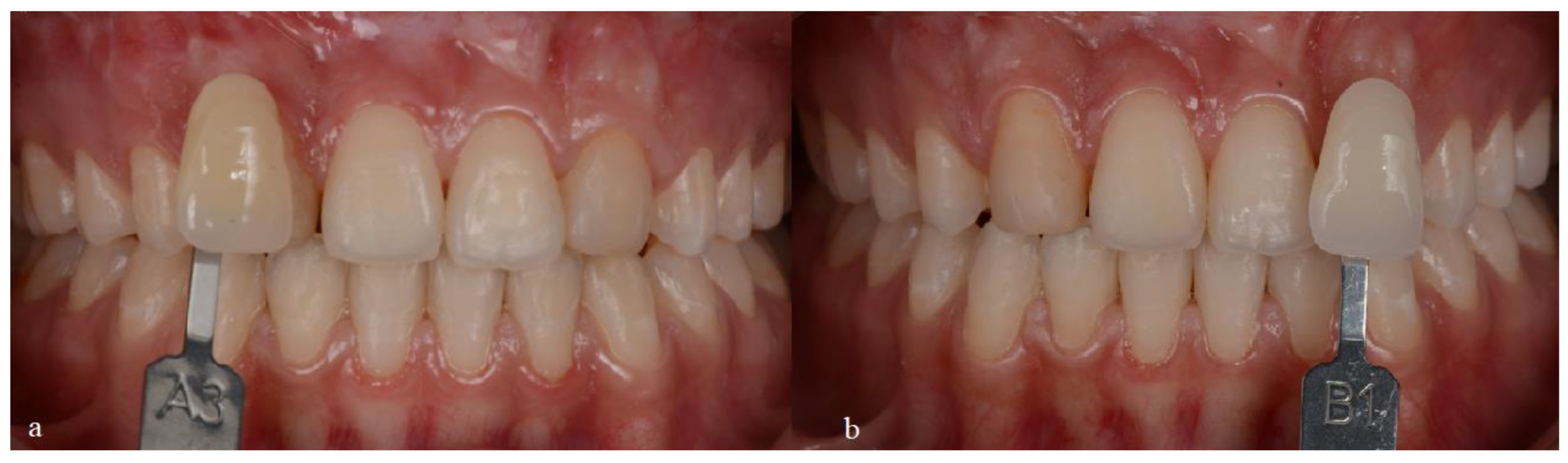
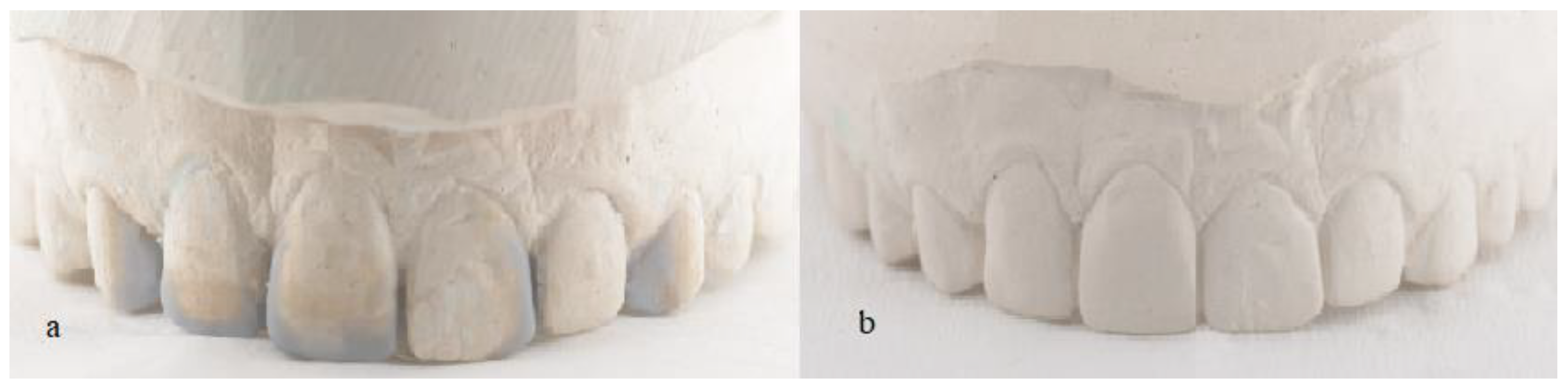
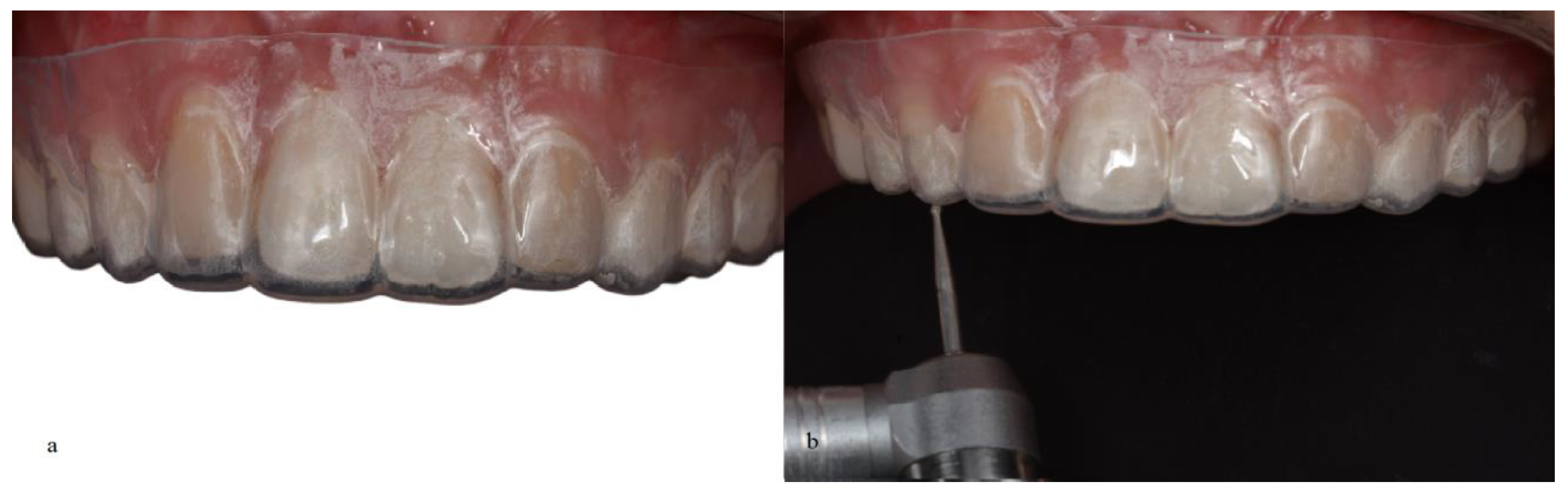
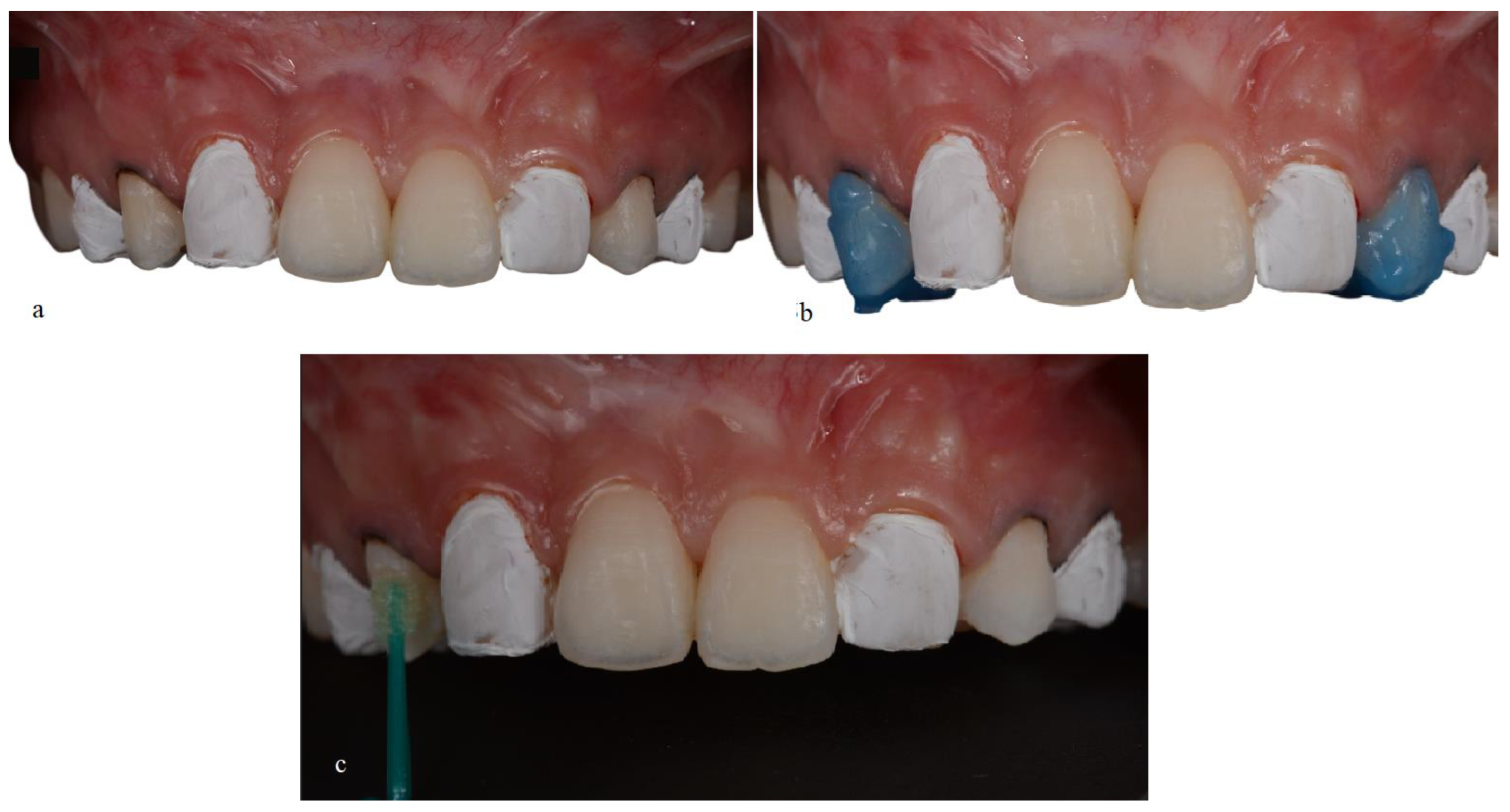
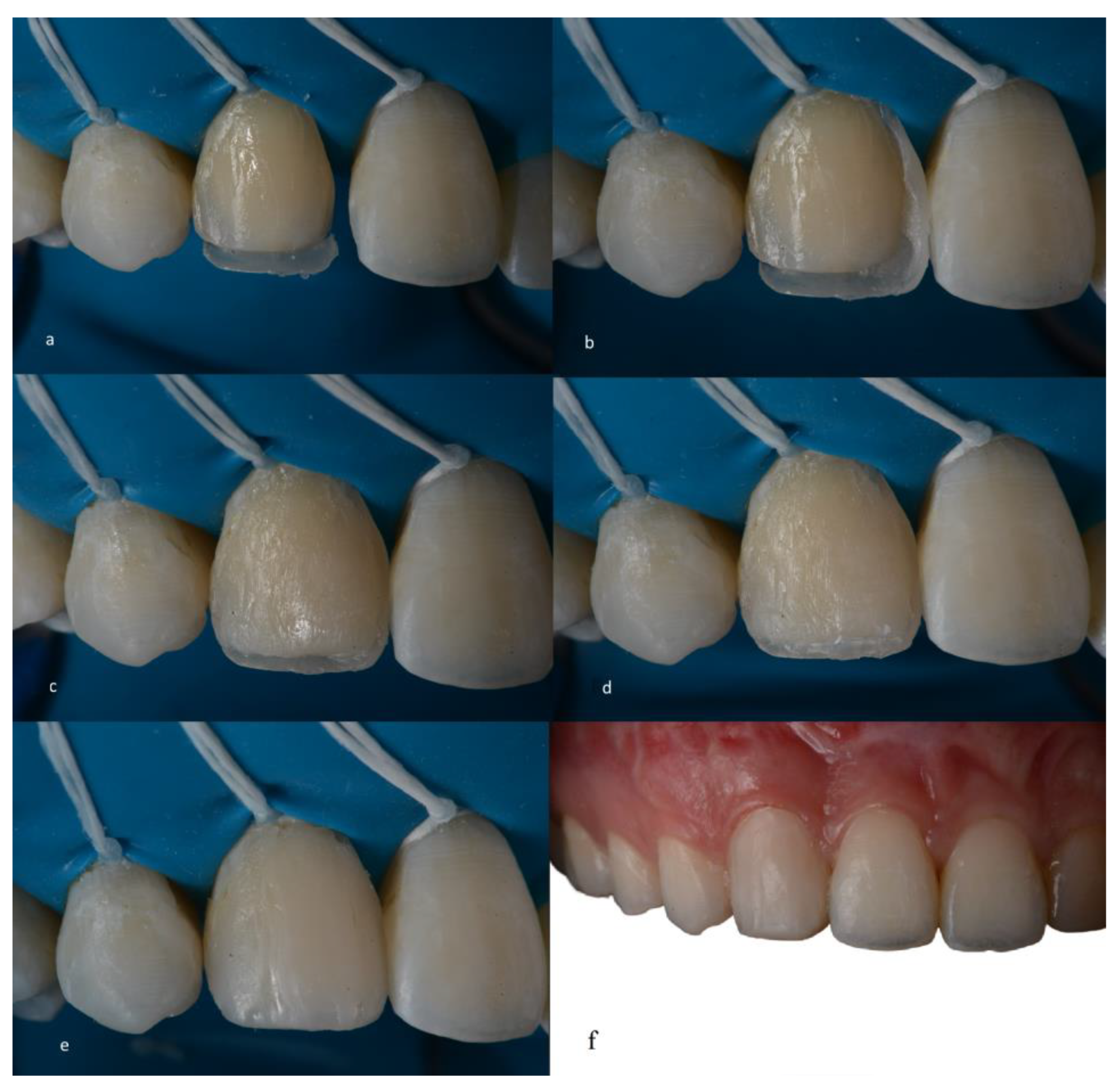
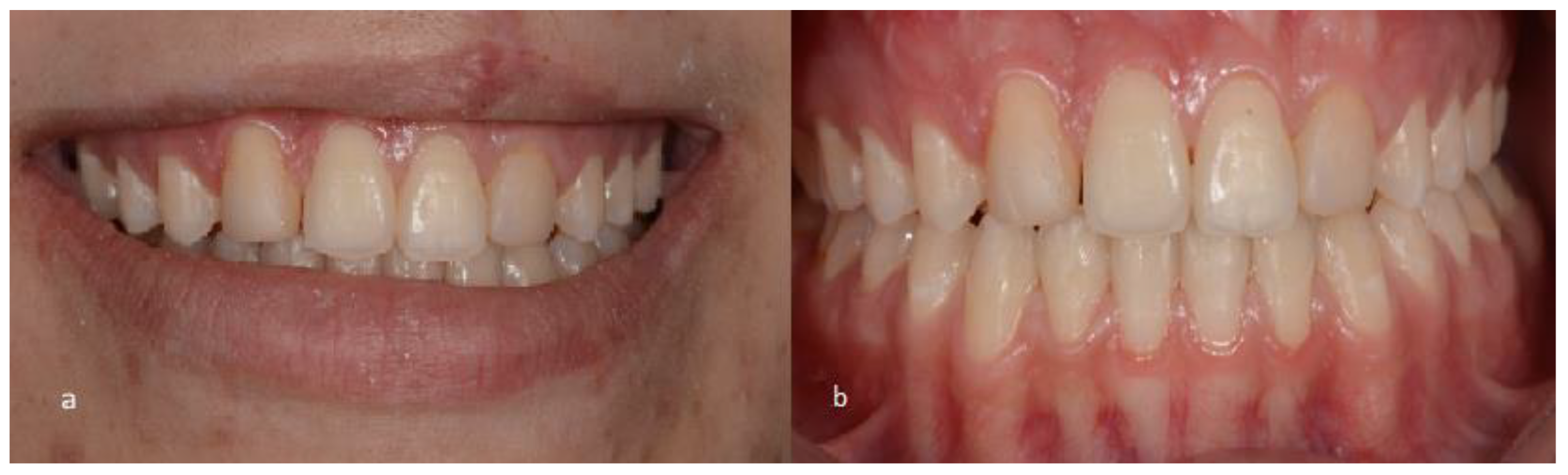
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Terry, D.A.; Powers, J.M. A predictable resin composite injection technique, Part I. Dent. Today 2014, 33, 96–101. [Google Scholar] [PubMed]
- Terry, D.; Powers, J. Using injectable resin composite: Part two. Int. Dent. Afr. 2014, 5, 64–72. [Google Scholar]
- Bayne, S.C.; Thompson, J.Y.; Swift, E.J., Jr.; Stamatiades, P.; Wilkerson, M. A characterization of first-generation flowable composites. J. Am. Dent. Assoc. 1998, 129, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Baroudi, K.; Rodrigues, J.C. Flowable Resin Composites: A Systematic Review and Clinical Considerations. J. Clin. Diagn. Res. 2015, 9, Ze18–Ze24. [Google Scholar] [CrossRef]
- Terry, D.A.; Powers, J.M.; Blatz, M.B. The Inverse Injection Layering TECHNIQUE. J. Cosmetic Dent. 2018, 34, 48–62. [Google Scholar]
- Tangutoori, T.; Devendra, C.; Ravi, N.; Atul, B.; Sharma, Y.; Eliezer, R. Flowable Resin Composites—A Systematic Review and Clinical Considerations. World J. Adv. Sci. Res. 1982, 1, 186–191. [Google Scholar]
- Lai, W.L.; Saeedipour, H.; Goh, K.L. Dataset on mechanical properties of damaged fiber composite laminates with drilled vent-holes for the resin-injection repair procedure. Data Brief 2019, 24, 103912. [Google Scholar] [CrossRef]
- Imai, A.; Takamizawa, T.; Sugimura, R.; Tsujimoto, A.; Ishii, R.; Kawazu, M.; Saito, T.; Miyazaki, M. Interrelation among the handling, mechanical, and wear properties of the newly developed flowable resin composites. J. Mech. Behav. Biomed. Mater. 2019, 89, 72–80. [Google Scholar] [CrossRef]
- Ujiie, M.; Tsujimoto, A.; Barkmeier, W.W.; Jurado, C.A.; Villalobos-Tinoco, J.; Takamizawa, T.; Latta, M.A.; Miyazaki, M. Comparison of occlusal wear between bulk-fill and conventional flowable resin composites. Am. J. Dent. 2020, 33, 74–78. [Google Scholar]
- Geštakovski, D. The injectable composite resin technique: Minimally invasive reconstruction of esthetics and function. Clinical case report with 2-year follow-up. Quintessence Int. 2019, 50, 712–719. [Google Scholar] [CrossRef]
- Geštakovski, D. The injectable composite resin technique: Biocopy of a natural tooth-advantages of digital planning. Int. J. Esthet. Dent. 2021, 16, 280–299. [Google Scholar] [PubMed]
- Ypei Gia, N.R.; Sampaio, C.S.; Higashi, C.; Sakamoto, A., Jr.; Hirata, R. The injectable resin composite restorative technique: A case report. J. Esthet. Restor. Dent. 2021, 33, 404–414. [Google Scholar] [CrossRef] [PubMed]
- Camporesi, M.; Baccetti, T.; Marinelli, A.; Defraia, E.; Franchi, L. Maxillary dental anomalies in children with cleft lip and palate: A controlled study. Int. J. Paediatr. Dent. 2010, 20, 442–450. [Google Scholar] [CrossRef] [PubMed]
- De Lima Pedro, R.; Faria, M.D.; de Castro Costa, M.; Vieira, A.R. Dental anomalies in children born with clefts: A case-control study. Cleft Palate Craniofac J. 2012, 49, e64–e68. [Google Scholar] [CrossRef] [PubMed]
- Letra, A.; Menezes, R.; Granjeiro, J.M.; Vieira, A.R. Defining subphenotypes for oral clefts based on dental development. J. Dent. Res. 2007, 86, 986–991. [Google Scholar] [CrossRef]
- Sá, J.; Mariano, L.C.; Canguçu, D.; Coutinho, T.S.; Hoshi, R.; Medrado, A.P.; Martelli-Junior, H.; Coletta, R.D.; Reis, S.R. Dental Anomalies in a Brazilian Cleft Population. Cleft Palate Craniofac. J. 2016, 53, 714–719. [Google Scholar] [CrossRef]
- Peter, J.P.; Chinsky, R.R.; Fisher, M.J. Sociological aspects of cleft palate adults: IV. Social integration. Cleft Palate J. 1975, 12, 304–310. [Google Scholar]
- Kapp-Simon, K.A.; McGuire, D.E. Observed social interaction patterns in adolescents with and without craniofacial conditions. Cleft Palate Craniofac J. 1997, 34, 380–384. [Google Scholar] [CrossRef]
- Tannure, P.N.; Oliveira, C.A.; Maia, L.C.; Vieira, A.R.; Granjeiro, J.M.; Costa Mde, C. Prevalence of dental anomalies in nonsyndromic individuals with cleft lip and palate: A systematic review and meta-analysis. Cleft Palate Craniofac. J. 2012, 49, 194–200. [Google Scholar] [CrossRef]
- Lourenço Ribeiro, L.; Teixeira Das Neves, L.; Costa, B.; Ribeiro Gomide, M. Dental anomalies of the permanent lateral incisors and prevalence of hypodontia outside the cleft area in complete unilateral cleft lip and palate. Cleft Palate Craniofac. J. 2003, 40, 172–175. [Google Scholar] [CrossRef]
- Paradowska-Stolarz, A.; Mikulewicz, M.; Duś-Ilnicka, I. Current Concepts and Challenges in the Treatment of Cleft Lip and Palate Patients—A Comprehensive Review. J. Pers. Med. 2022, 12, 2089. [Google Scholar] [CrossRef] [PubMed]
- Ariawan, D.; Vitria, E.E.; Sulistyani, L.D.; Anindya, C.S.; Adrin, N.S.R.; Aini, N.; Hak, M.S. Prevalence of Simonart’s band in cleft children at a cleft center in Indonesia: A nine-year retrospective study. Dent. Med. Probl. 2022, 59, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Yatabe, M.S.; Garib, D.G.; Janson, G.; Poletto, R.S.; Ozawa, T.O. Is the presence of Simonart’s band in patients with complete unilateral cleft lip and palate associated with the prevalence of missing maxillary lateral incisors? Am. J. Orthod. Dentofacial Orthop. 2013, 144, 649–653. [Google Scholar] [CrossRef]
- Stock, N.M.; Feragen, K.B.; Rumsey, N. “It Doesn’t All Just Stop at 18”: Psychological Adjustment and Support Needs of Adults Born With Cleft Lip and/or Palate. Cleft Palate Craniofac J. 2015, 52, 543–554. [Google Scholar] [CrossRef] [PubMed]
- Brinkmann, J.C.-B.; Albanchez-González, M.I.; Peña, D.M.L.; Gil, I.G.; García, M.J.S.; Rico, J. Improvement of aesthetics in a patient with tetracycline stains using the injectable composite resin technique: Case report with 24-month follow-up. Br. Dent. J. 2020, 229, 774–778. [Google Scholar] [CrossRef]
- Maroulakos, G.; Maroulakos, M.P.; Tsoukala, E.; Angelopoulou, M.V. Dental Reshaping Using the Composite Resin Injection Technique After Dental Trauma and Orthodontic Treatment. J. Dent. Child. 2021, 88, 144–147. [Google Scholar]
- Coachman, C.; De Arbeloa, L.; Mahn, G.; Sulaiman, T.A.; Mahn, E. An Improved Direct Injection Technique With Flowable Composites. A Digital Workflow Case Report. Oper. Dent. 2020, 45, 235–242. [Google Scholar] [CrossRef]
- Surendar, S.; Abraham, A. Diastema closure using a predictable flowable resin composite injection technique–A case report. Indian. Assoc. Conserv. Dent. Endod. 2017. [Google Scholar]
- Hosaka, K.; Tichy, A.; Motoyama, Y.; Mizutani, K.; Lai, W.J.; Kanno, Z.; Tagami, J.; Nakajima, M. Post-orthodontic recontouring of anterior teeth using composite injection technique with a digital workflow. J. Esthet. Restor. Dent. 2020, 32, 638–644. [Google Scholar] [CrossRef]
- Sumino, N.; Tsubota, K.; Takamizawa, T.; Shiratsuchi, K.; Miyazaki, M.; Latta, M.A. Comparison of the wear and flexural characteristics of flowable resin composites for posterior lesions. Acta Odontol. Scand. 2013, 71, 820–827. [Google Scholar] [CrossRef]
- Prabhakar, A.R.; Madan, M.; Raju, O.S. The marginal seal of a flowable composite, an injectable resin modified glass ionomer and a compomer in primary molars--an in vitro study. J. Indian. Soc. Pedod. Prev. Dent. 2003, 21, 45–48. [Google Scholar] [PubMed]
- Kitasako, Y.; Sadr, A.; Burrow, M.F.; Tagami, J. Thirty-six month clinical evaluation of a highly filled flowable composite for direct posterior restorations. Aust. Dent. J. 2016, 61, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Freitas, J.A.; Almeida, A.L.; Soares, S.; Neves, L.T.; Garib, D.G.; Trindade-Suedam, I.K.; Yaedú, R.Y.; Lauris Rde, C.; Oliveira, T.M.; Pinto, J.H. Rehabilitative treatment of cleft lip and palate: Experience of the Hospital for Rehabilitation of Craniofacial Anomalies/USP (HRAC/USP)—Part 4: Oral rehabilitation. J. Appl. Oral. Sci. 2013, 21, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Demarco, F.F.; Cenci, M.S.; Montagner, A.F.; de Lima, V.P.; Correa, M.B.; Moraes, R.R.; Opdam, N.J.M. Longevity of composite restorations is definitely not only about materials. Dent. Mater. 2022, 39, 1–12. [Google Scholar] [CrossRef]
- Balagopal, S.; Geethapriya, N.; Anisha, S.; Hemasathya, B.A.; Vandana, J.; Dhatshayani, C. Comparative evaluation of the degree of conversion of four different composites polymerized using ultrafast photopolymerization technique: An in vitro study. J. Conserv. Dent. 2021, 24, 77–82. [Google Scholar] [CrossRef]
- Moraes, R.R.; Cenci, M.S.; Moura, J.R.; Demarco, F.F.; Loomans, B.; Opdam, N.J.C.O.H.R. Clinical performance of resin composite restorations. Curr. Oral. Health Rep. 2022, 9, 22–31. [Google Scholar] [CrossRef]
- Da Rosa Rodolpho, P.A.; Rodolfo, B.; Collares, K.; Correa, M.B.; Demarco, F.F.; Opdam, N.J.M.; Cenci, M.S.; Moraes, R.R. Clinical performance of posterior resin composite restorations after up to 33 years. Dent. Mater. 2022, 38, 680–688. [Google Scholar] [CrossRef]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villafuerte, K.R.V.; Obeid, A.T.; de Oliveira, N.A. Injectable Resin Technique as a Restorative Alternative in a Cleft Lip and Palate Patient: A Case Report. Medicina 2023, 59, 849. https://doi.org/10.3390/medicina59050849
Villafuerte KRV, Obeid AT, de Oliveira NA. Injectable Resin Technique as a Restorative Alternative in a Cleft Lip and Palate Patient: A Case Report. Medicina. 2023; 59(5):849. https://doi.org/10.3390/medicina59050849
Chicago/Turabian StyleVillafuerte, Kelly R. V., Alyssa Teixeira Obeid, and Naiara Araújo de Oliveira. 2023. "Injectable Resin Technique as a Restorative Alternative in a Cleft Lip and Palate Patient: A Case Report" Medicina 59, no. 5: 849. https://doi.org/10.3390/medicina59050849
APA StyleVillafuerte, K. R. V., Obeid, A. T., & de Oliveira, N. A. (2023). Injectable Resin Technique as a Restorative Alternative in a Cleft Lip and Palate Patient: A Case Report. Medicina, 59(5), 849. https://doi.org/10.3390/medicina59050849