
Association of Pro-Inflammatory Cytokines with Vitamin D in Hashimoto’s Thyroid Autoimmune Disease



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Subjects’ Selection Criteria
2.2.1. Ethical Considerations
- Permission of the competent authority was obtained before the start of the study;
- Written informed consent (attached) was taken from all the participants in accordance with provisions of the Declaration of Helsinki;
- All information and data collection were kept confidential;
- Participants remained anonymous throughout the study and their privacy was protected. Their identity will not be revealed in any publication resulting from this study;
- Participation in the case-control study was considered voluntary for the study subjects and their discretion not to participate or withdraw their consent at any time was observed. They were not penalized in any way if they decided not to participate or to withdraw from the study;
- Data about the study will not be shared with anyone except for academic purposes.
2.2.2. Statement of Confidentiality
2.3. History and Medical Records
2.4. Specimen Collection, Transportation, and Analysis
2.5. Statistical Consideration
3. Results
3.1. Levels of Thyroid Hormones and Thyroid Auto Antibodies in Patients with Hashimoto’s Diseases v/s Healthy Controls
3.2. The Concentrations of Pro-Inflamatory Cytokines in Patients with Hashimoto’s Diseases v/s Healthy Controls
3.3. The Total Vitamin D Levels in Patients with Hashimoto’s Disease v/s Healthy Controls
3.4. Correlation between Anti-TPO and Total Vitamin D Levels
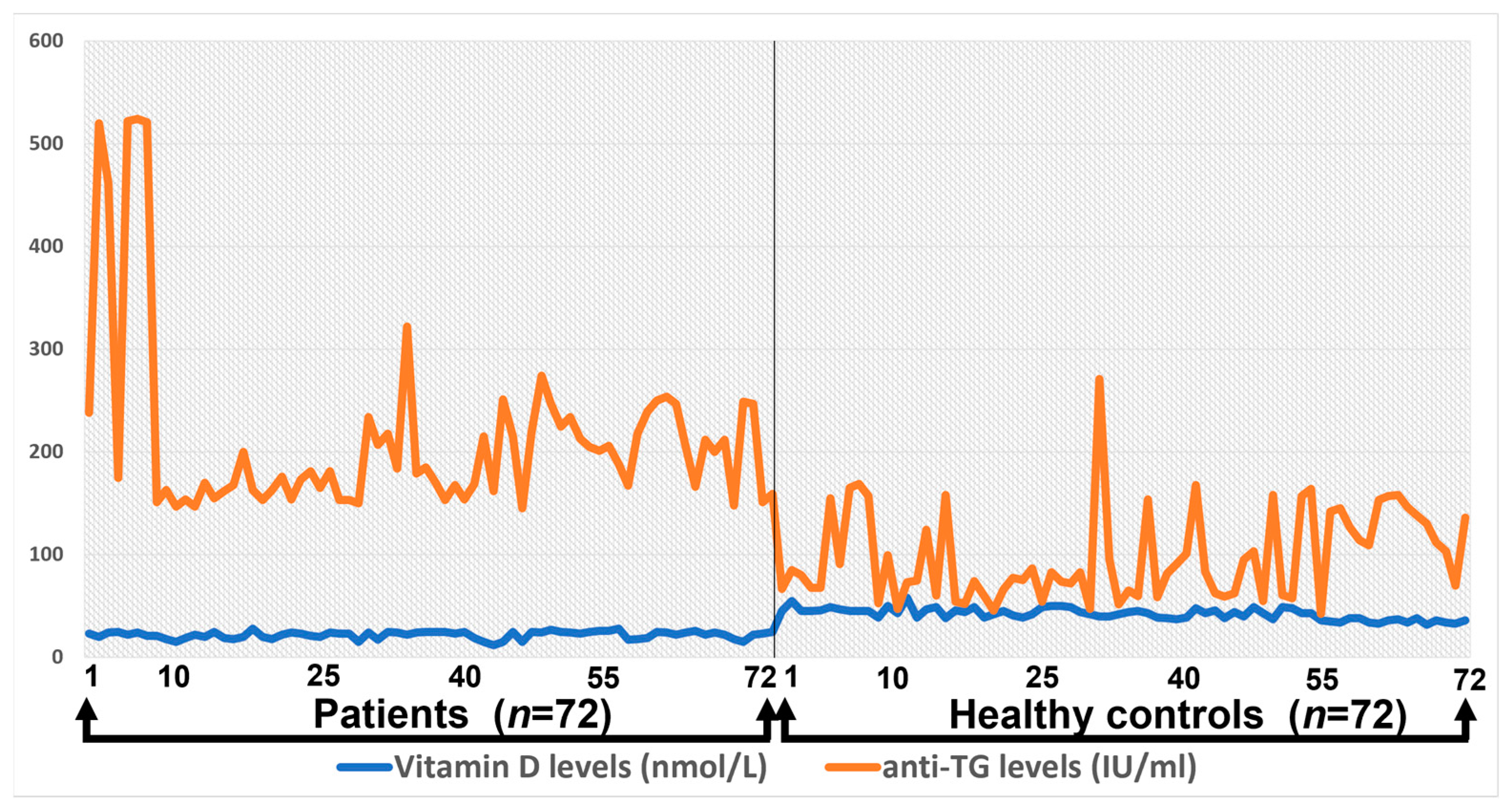
3.5. Correlation between Anti-TG and Total Vitamin D Levels
3.6. Correlation between Pro-Inflamatory Cytokines and Total Vitamin D Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rayman, M.P. Multiple nutritional factors and thyroid disease, with particular reference to autoimmune thyroid disease. Proc. Nutr. Soc. 2019, 78, 34–44. [Google Scholar] [CrossRef]
- Rotondi, M.; Carbone, A.; Coperchini, F.; Fonte, R.; Chiovato, L. Diagnosis of endocrine disease: IgG4-related thyroid autoimmune disease. Eur. J. Endocrinol. 2019, 180, R175–R183. [Google Scholar] [CrossRef]
- Farling, P. Thyroid disease. Br. J. Anaesth. 2000, 85, 15–28. [Google Scholar] [CrossRef]
- Brent, G.A. Graves’ disease. N. Engl. J. Med. 2008, 358, 2594–2605. [Google Scholar] [CrossRef]
- Vanderpump, M.P. The epidemiology of thyroid disease. Br. Med. Bull. 2011, 99, 39–51. [Google Scholar] [CrossRef]
- Ragusa, F.; Fallahi, P.; Elia, G.; Gonnella, D.; Paparo, S.R.; Giusti, C.; Churilov, L.P.; Ferrari, S.M.; Antonelli, A. Hashimotos’ thyroiditis: Epidemiology, pathogenesis, clinic and therapy. Best Pract. Res. Clin. Endocrinol. Metab. 2019, 33, 101367. [Google Scholar] [CrossRef] [PubMed]
- Jin, B.; Wang, S.; Fan, Z. Pathogenesis Markers of Hashimoto’s Disease-A Mini Review. Front. Biosci. 2022, 27, 297. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Huang, H.; Yu, X. How does Hashimoto’s thyroiditis affect bone metabolism? Rev. Endocr. Metab. Disord. 2023, 24, 191–205. [Google Scholar] [CrossRef]
- Caturegli, P.; De Remigis, A.; Rose, N. Hashimoto thyroiditis: Clinical and diagnostic criteria. Autoimmun. Rev. 2014, 13, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Zaletel, K. Determinants of thyroid autoantibody production in Hashimoto’s thyroiditis. Expert Rev. Clin. Immunol. 2007, 3, 217–223. [Google Scholar] [CrossRef]
- Thangaratinam, S.; Tan, A.; Knox, E.; Kilby, M.D.; Franklyn, J.; Coomarasamy, A. Association between thyroid autoantibodies and miscarriage and preterm birth: Meta-analysis of evidence. BMJ 2011, 342, d2616. [Google Scholar] [CrossRef] [PubMed]
- Uysal, H.B.; Ayhan, M. Autoimmunity affects health-related quality of life in patients with Hashimoto’s thyroiditis. Kaohsiung J. Med. Sci. 2016, 32, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Ban, Y.; Greenberg, D.A.; Davies, T.F.; Jacobson, E.; Concepcion, E.; Tomer, Y. Linkage analysis of thyroid antibody production: Evidence for shared susceptibility to clinical autoimmune thyroid disease. J. Clin. Endocrinol. Metab. 2008, 93, 3589–3596. [Google Scholar] [CrossRef] [PubMed]
- Mansoor, S. Trends of congenital hypothyroidism and inborn errors of metabolism in Pakistan. Orphanet J. Rare Dis. 2020, 15, 321. [Google Scholar] [CrossRef]
- Nguyen, K.G.; Vrabel, M.R.; Mantooth, S.M.; Hopkins, J.J.; Wagner, E.S.; Gabaldon, T.A.; Zaharoff, D.A. Localized interleukin-12 for cancer immunotherapy. Front. Immunol. 2020, 11, 575597. [Google Scholar]
- Lin, J.; Liu, J.; Davies, M.L.; Chen, W. Serum vitamin D level and rheumatoid arthritis disease activity: Review and meta-analysis. PLoS ONE 2016, 11, e0146351. [Google Scholar] [CrossRef]
- Zivancevic-Simonovic, S.; Mihaljevic, O.; Majstorovic, I.; Popovic, S.; Markovic, S.; Milosevic-Djordjevic, O.; Jovanovic, Z.; Mijatovic-Teodorovic, L.; Mihajlovic, D.; Colic, M. Cytokine production in patients with papillary thyroid cancer and associated autoimmune Hashimoto thyroiditis. Cancer Immunol. Immunother. 2015, 64, 1011–1019. [Google Scholar] [CrossRef]
- Gerenova, J.; Manolova, I.; Stanilova, S. Impact of IL-10 and IL-12B single nucleotide polymorphisms on circulating cytokine level in development of Hashimoto’s thyroiditis. Biotechnol. Biotechnol. Equip. 2016, 30, 713–720. [Google Scholar] [CrossRef]
- Ma, Y.; Ren, Y.; Dai, Z.-J.; Wu, C.-J.; Ji, Y.-H.; Xu, J. IL-6, IL-8 and TNF-α levels correlate with disease stage in breast cancer patients. Adv. Clin. Exp. Med. 2017, 26, 421–426. [Google Scholar] [CrossRef]
- Gaitonde, D.Y.; Rowley, K.D.; Sweeney, L.B. Hypothyroidism: An update. S. Afr. Fam. Pract. 2012, 54, 384–390. [Google Scholar] [CrossRef]
- Phenekos, C.; Vryonidou, A.; Gritzapis, A.D.; Baxevanis, C.N.; Goula, M.; Papamichail, M. Th1 and Th2 serum cytokine profiles characterize patients with Hashimoto’s thyroiditis (Th1) and Graves’ disease (Th2). Neuroimmunomodulation 2004, 11, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Wyns, H.; Croubels, S.; Demeyere, K.; Watteyn, A.; De Backer, P.; Meyer, E. Development of a cytometric bead array screening tool for the simultaneous detection of pro-inflammatory cytokines in porcine plasma. Vet. Immunol. Immunopathol. 2013, 151, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Kobawala, T.P.; Patel, G.H.; Gajjar, D.R.; Patel, K.N.; Thakor, P.B.; Parekh, U.B.; Patel, K.M.; Shukla, S.N.; Shah, P.M. Clinical utility of serum interleukin-8 and interferon-alpha in thyroid diseases. J. Thyroid. Res. 2011, 2011, 270149. [Google Scholar] [CrossRef] [PubMed]
- Mateen, S.; Moin, S.; Shahzad, S.; Khan, A.Q. Level of inflammatory cytokines in rheumatoid arthritis patients: Correlation with 25-hydroxy vitamin D and reactive oxygen species. PLoS ONE 2017, 12, e0178879. [Google Scholar] [CrossRef]
- Nozawa, K.; Fujishiro, M.; Takasaki, Y.; Sekigawa, I. Inhibition of rheumatoid arthritis by blocking connective tissue growth factor. World J. Orthop. 2014, 5, 653. [Google Scholar] [CrossRef]
- Kobawala, T.P.; Trivedi, T.I.; Gajjar, K.K.; Patel, D.H.; Patel, G.H.; Ghosh, N.R. Significance of interleukin-6 in papillary thyroid carcinoma. J. Thyroid. Res. 2016, 2016, 6178921. [Google Scholar] [CrossRef]
- Arend, W.P. Cytokine imbalance in the pathogenesis of rheumatoid arthritis: The role of interleukin-1 receptor antagonist. Semin. Arthritis Rheum. 2001, 30, 1–6. [Google Scholar] [CrossRef]
- Kobawala, T.P.; Trivedi, T.I.; Gajjar, K.K.; Patel, D.H.; Patel, G.H.; Ghosh, N.R. Significance of TNF-α and the adhesion molecules: L-selectin and VCAM-1 in papillary thyroid carcinoma. J. Thyroid. Res. 2016, 2016. [Google Scholar] [CrossRef]
- Yoshida, Y.; Tanaka, T. Interleukin 6 and rheumatoid arthritis. BioMed Res. Int. 2014, 2014. [Google Scholar] [CrossRef]
- Qian, W.; Ge, X.X.; Wu, J.; Gong, F.R.; Wu, M.Y.; Xu, M.D.; Lian, L.; Wang, W.J.; Li, W.; Tao, M. Prognostic evaluation of resectable colorectal cancer using platelet-associated indicators. Oncol. Lett. 2019, 18, 571–580. [Google Scholar] [CrossRef]
- Chao, G.; Zhu, Y.; Fang, L. Correlation Between Hashimoto’s Thyroiditis–Related Thyroid Hormone Levels and 25-Hydroxyvitamin D. Front. Endocrinol. 2020, 11, 4. [Google Scholar] [CrossRef] [PubMed]
- Lei, Y.; Yang, J.; Li, H.; Zhong, H.; Wan, Q. Changes in glucose-lipid metabolism, insulin resistance, and inflammatory factors in patients with autoimmune thyroid disease. J. Clin. Lab. Anal. 2019, 33, e22929. [Google Scholar] [CrossRef] [PubMed]
- Van Roon, J.A.; Lafeber, F.P.; Bijlsma, J. Synergistic activity of interleukin-4 and interleukin-10 in suppression of inflammation and joint destruction in rheumatoid arthritis. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 2001, 44, 3–12. [Google Scholar] [CrossRef]
- Qazi, B.S.; Tang, K.; Qazi, A. Recent advances in underlying pathologies provide insight into interleukin-8 expression-mediated inflammation and angiogenesis. Int. J. Inflamm. 2011, 2011, 908468. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | n | % |
|---|---|---|
| 18–25 | 27 | 18.7 |
| 26–30 | 28 | 19.4 |
| 31–35 | 32 | 22.2 |
| 36–40 | 23 | 15.9 |
| 41–45 | 11 | 7.6 |
| 46–50 | 8 | 5.5 |
| 51–55 | 13 | 9 |
| 56–60 | 2 | 1.3 |
| Variables | Unit | Hashimoto’s Disease | Control |
|---|---|---|---|
| TSH | mIU/L | 7.674 ± 2.55 (M ± SD) | 2.13 ± 1.42 (M ± SD) |
| FT4 | pmol/L | 14.03 ± 4.96 (M ± SD) | 17.25 ± 2.16 (M ± SD) |
| FT3 | pg/mL | 2.69 ± 0.19 (M ± SD) | 2.80 ± 0.15 (M ± SD) |
| Anti-TPO | (IU/mL) | 285 ± 142 Median ± IQR | 5.0 ± 10.69 Median ± IQR |
| Anti-TG | (IU/mL) | 160 ± 63.5 Median ± IQR | 39.6 ± 80.05 Median ± IQR |
| Variables | Unit | Hashimoto’s Disease | Healthy Controls | p-Value |
|---|---|---|---|---|
| Interlukin-1B | pg/mL | 6.253 ± 0.382 | 0.601 ± 0.1756 | 0.000 * |
| Interlukin-6 | 9.465 ± 0.486 | 2.632 ± 0.553 | 0.393 | |
| Interlukin-8 | 7.539 ± 0.558 | 3.063 ± 1.235 | 0.008 * | |
| Interlukin-10 | 4.325 ± 0.497 | 3.396 ± 0.353 | 0.002 * | |
| Interlukin-12 | 3.813 ± 0.483 | 3.44 ± 0.481 | 0.850 | |
| TNF-α | 7.662 ± 1.132 | 1.459 ± 0.357 | 0.000 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siddiq, A.; Naveed, A.K.; Ghaffar, N.; Aamir, M.; Ahmed, N. Association of Pro-Inflammatory Cytokines with Vitamin D in Hashimoto’s Thyroid Autoimmune Disease. Medicina 2023, 59, 853. https://doi.org/10.3390/medicina59050853
Siddiq A, Naveed AK, Ghaffar N, Aamir M, Ahmed N. Association of Pro-Inflammatory Cytokines with Vitamin D in Hashimoto’s Thyroid Autoimmune Disease. Medicina. 2023; 59(5):853. https://doi.org/10.3390/medicina59050853
Chicago/Turabian StyleSiddiq, Amer, Abdul Khaliq Naveed, Nabila Ghaffar, Muhammad Aamir, and Naveed Ahmed. 2023. "Association of Pro-Inflammatory Cytokines with Vitamin D in Hashimoto’s Thyroid Autoimmune Disease" Medicina 59, no. 5: 853. https://doi.org/10.3390/medicina59050853
APA StyleSiddiq, A., Naveed, A. K., Ghaffar, N., Aamir, M., & Ahmed, N. (2023). Association of Pro-Inflammatory Cytokines with Vitamin D in Hashimoto’s Thyroid Autoimmune Disease. Medicina, 59(5), 853. https://doi.org/10.3390/medicina59050853