
The Influence of the Q-Angle and Muscle Strength on Idiopathic Anterior Knee Pain in Adolescents
 , , , and
, , , and
Abstract
:1. Introduction
2. Patients and Methods
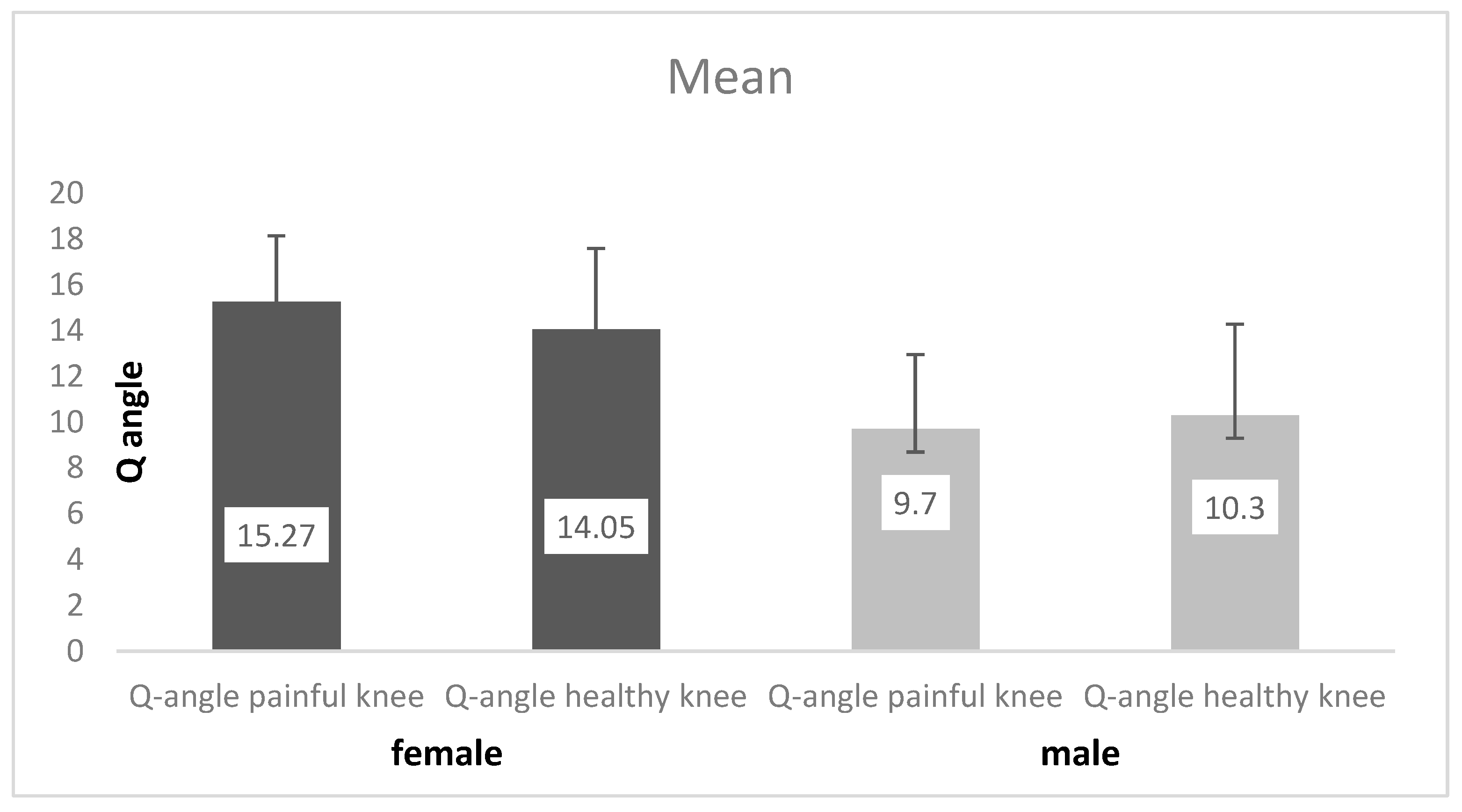
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shea, K.; Pfeiffer, R.; Curtin, M. Idiopathic anterior knee pain in adolescents. Orthop. Clin. N. Am. 2003, 34, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Thomee, R.; Augustsson, J.; Karlsson, J. Patellofemoral pain syndrome: A review of current issues. Sports Med. 1999, 28, 245–262. [Google Scholar] [CrossRef] [PubMed]
- Cutbill, J.; Ladly, K.; Bray, R.; Thorne, P.; Verhoef, M. Anterior knee pain: A Review. J. Sport. Med. 1997, 7, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Freedman, B.; Brindle, T.; Sheehan, F. Re-evaluating the functional implications of the Q-angle and its relationship to in-vivo patellofemoral kinematics. Clin. Biomech. 2014, 29, 1139–1145. [Google Scholar] [CrossRef]
- Miller, D.; Tumia, N.; Maffulli, N. Anterior knee pain. Trauma 2005, 7, 11–18. [Google Scholar] [CrossRef]
- Witvrouw, E.; Lysens, R.; Bellemans, J.; Cambier, D.; Vanderstraeten, G. Intrinsic risk factors for the development of anterior knee pain in an athletic population. Am. J. Sports Med. 2000, 28, 480–489. [Google Scholar] [CrossRef]
- Nimon, G.; Murray, D.; Sandow, M.; Goodfellow, J. Natural history of anterior knee pain: A 14- to 20-year follow-up of nonoperative management. J. Ped. Orthop. 1998, 18, 118–122. [Google Scholar] [CrossRef]
- Sanchis-Alfonso, V.; Rosello-Sastre, E.; Monteagudo-Castro, C.; Esquerdo, J. Quantitative analysis of nerve changes in the lateral retinaculum in patients with isolated symptomatic patellofemoral malalignment. A preliminary study. Am. J. Sports Med. 1998, 26, 703–709. [Google Scholar] [CrossRef]
- Fairbank, J.; Pynsent, P.; Poortvliet, J.; Phillips, H. Mechanical Factors in the Incidence of the Knee Pain in Adolescents and Young Adults. J. Bone Joint Surg. Br. 1984, 66, 685–693. [Google Scholar] [CrossRef]
- Sheehan, F.; Derasari, A.; Fine, K.; Brindle, T.; Alter, K. Q-angle and J-sign: Indicative of maltracking subgroups in patellofemoral pain. Clin. Orthop. Relat. Res. 2010, 468, 266–275. [Google Scholar] [CrossRef]
- Brattstroem, H. Shape of the intercondylar grove normaly and recurrent dislocation of patella. A clinical and X-ray-anatomical investigatione. Acta Orthop. Scand. Suppl. 1964, 68, 1–148. [Google Scholar] [CrossRef]
- Goldberg, B. Chronic anteriror knee pain in the adolescent. Ped. Ann. 1991, 20, 186–193. [Google Scholar] [CrossRef]
- Patil, S.; White, L.; Jones, A.; Hui, A.C. Idiopathic anterior knee pain in the young. A prospective controlled trial. Acta Orthop. Belg. 2010, 76, 356–359. [Google Scholar]
- Kannus, P.; Natri, A.; Paakkala, T.; Jarvinen, M. An outcome study of chronic patellofemoral pain syndrome. Seven-year follow-up of patients in a randomized, controlled trial. J. Bone Joint Surg. Am. 1999, 81, 355–363. [Google Scholar] [CrossRef]
- Karlsson, J.; Thomee, R.; Sward, L. Eleven year follow-up of patello-femoral pain syndrome. Clin. J. Sport. Med. 1996, 6, 22–26. [Google Scholar] [CrossRef]
- Natari, A.; Kannus, P.; Jarvinen, M. Which factors predict the long-term outcome in chronic patellofemoral pain syndrome? A 7-yr prospective follow-up study. Med. Sci. Sports Exerc. 1999, 30, 1572–1577. [Google Scholar] [CrossRef]
- Hand, C.J.; Spalding, T.J. Association between anatomical features and anterior knee pain in a “fit” service population. J. R. Nav. Med. Serv. 2004, 90, 125–134. [Google Scholar] [CrossRef]
- Sandow, M.J.; Goodfellow, J.W. The natural history of anterior knee pain in adolescents. J. Bone Joint Surg. Br. 1985, 67, 36–38. [Google Scholar] [CrossRef]
- Fulkerson, J.; Arendt, E. Anterior knee pain in females. Clin. Orthop. Relat. Res. 2000, 372, 69–73. [Google Scholar] [CrossRef]
- Fulkerson, J.; Hungerford, D.S. Disorders of the Patellofemoral Joint, 2nd ed.; Williams and Wilkins: Baltimore, MD, USA, 1990. [Google Scholar]
- Caylor, D.; Fites, R.; Worrell, T.W. The relationship between quadriceps angle and anterior knee pain syndrome. J. Orthop. Sports Phys. Ther. 1993, 17, 11–16. [Google Scholar] [CrossRef]
- Kaya, D.; Doral, M.N. Is there any relationship between Q-angle and lower extremity malalignment? Acta Orthop. Traumatol. Turc. 2012, 46, 416–419. [Google Scholar] [CrossRef] [PubMed]
- Haim, A.; Yaniv, M.; Dekel, S.; Amir, H. Patellofemoral pain syndrome: Validity of clinical and radiological features. Clin. Orthop. Relat. Res. 2006, 451, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Kumar, C.; Thapa, S.S.; Lamichhane, A.P. The relationship of quadriceps angle and anterior knee pain. J. Clin. Diagnostic Res. 2018, 12, 13–16. [Google Scholar] [CrossRef]
- Silva Dde, O.; Briani, R.V.; Pazzinatto, M.F.; Gonçalves, A.V.; Ferrari, D.; Aragão, F.A.; de Azevedo, F.M. Q-angle static or dynamic mesurements, which is the best choice for patellofemoral pain? Clin. Biomech. 2015, 30, 1083–1087. [Google Scholar] [CrossRef]
- Phatama, K.Y.; Isma, S.P.P.; Devi, L.K.; Siahaan, L.D.; Pribadi, A.; Pradana, A.S.; Mustasir, E.; Hidayat, M. Relationship of anterior knee pain with quadriceps angle and anthropometric mesurements in an Asia female population. Malays. Orthop. J. 2022, 16, 95–101. [Google Scholar]
- Erkocak, O.F.; Altan, E.; Altintas, M.; Turkmen, F.; Aydin, B.K.; Bayar, A. Lower extremity rotational deformities and patellofemoral alignment parameters in patients with anterior knee pain. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3011–3020. [Google Scholar] [CrossRef]
- Park, S.K.; Stefanyshyn, D. Greater Q angle may not be a risk factor of Patellofemoral Pain Syndrom. Clin. Biomech. 2011, 26, 392–396. [Google Scholar] [CrossRef]
- Werner, S.; Arvidsson, H.; Arvidsson, I.; Eriksson, E. Electrical stimulation of vastusmedialis and stretching of lateral thigh muscles in patients with patello-femoral symptoms. Knee Surg. Sports Traumatol. Arthrosc. 1993, 1, 85–92. [Google Scholar] [CrossRef]
- Kaya, D.; Citaker, S.; Kerimoglu, U.; Atay, O.A.; Nyland, J.; Callaghan, M.; Yakut, Y.; Yüksel, I.; Doral, M.N. Women with patellofemoral pain syndrome have quadriceps femoris volume and strength deficiency. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 242–247. [Google Scholar] [CrossRef]
- Boling, M.C.; Padua, D.A.; Marschall, S.W.; Guskiewicz, K.; Pyne, S.; Beutler, A. A prospective investigation of biomechanical risk factors for patellofemoral pain syndrome: The Joint Undertaking to Monitor and Prevent ACL Injury (JUMP-ACL) cohort. Am. J. Sports Med. 2009, 37, 2108–2116. [Google Scholar] [CrossRef]
- Callaghan, M.J.; Oldham, J.A. Quadriceps atrophy: To what extent does it exist in patellofemoral pain syndrome? Brit. J. Sport Med. 2004, 23, 295–299. [Google Scholar] [CrossRef]
- Giles, L.S.; Webster, K.E.; McClelland, J.A.; Cook, J. Does quadriceps atrophy exist in individuals with patellofemoral pain? A systematic literature review with meta-analysis. J. Orthop. Sports Phys. Ther. 2013, 43, 766–776. [Google Scholar] [CrossRef]
- Sac, A.; Tasmektepligil, M.Y. Correlation between the Q angle and the isokinetic strenght and muscle activity. Turk. J. Phys. Med. Rehab. 2018, 64, 308–313. [Google Scholar]

{kind=link}
| Muscle Strength | Mean | Number | Standard Deviation | |
|---|---|---|---|---|
| Male subgroup | Idiopathic AKP | 18.983 | 30 | 3.4876 |
| Non-affected knee | 22.517 | 30 | 2.2456 | |
| Female subgroup | Idiopathic AKP | 16.634 | 41 | 4.9548 |
| Non-affected knee | 19.902 | 41 | 3.6318 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milovanović, D.; Begović, N.; Bukva, B.; Dučić, S.; Vlahović, A.; Paunović, Z.; Kadija, M.; Topalović, N.; Stijak, L. The Influence of the Q-Angle and Muscle Strength on Idiopathic Anterior Knee Pain in Adolescents. Medicina 2023, 59, 1016. https://doi.org/10.3390/medicina59061016
Milovanović D, Begović N, Bukva B, Dučić S, Vlahović A, Paunović Z, Kadija M, Topalović N, Stijak L. The Influence of the Q-Angle and Muscle Strength on Idiopathic Anterior Knee Pain in Adolescents. Medicina. 2023; 59(6):1016. https://doi.org/10.3390/medicina59061016
Chicago/Turabian StyleMilovanović, Darko, Ninoslav Begović, Bojan Bukva, Siniša Dučić, Aleksandar Vlahović, Zoran Paunović, Marko Kadija, Nikola Topalović, and Lazar Stijak. 2023. "The Influence of the Q-Angle and Muscle Strength on Idiopathic Anterior Knee Pain in Adolescents" Medicina 59, no. 6: 1016. https://doi.org/10.3390/medicina59061016
APA StyleMilovanović, D., Begović, N., Bukva, B., Dučić, S., Vlahović, A., Paunović, Z., Kadija, M., Topalović, N., & Stijak, L. (2023). The Influence of the Q-Angle and Muscle Strength on Idiopathic Anterior Knee Pain in Adolescents. Medicina, 59(6), 1016. https://doi.org/10.3390/medicina59061016