
Assessment of mRNA Vaccine Immunogenicity in Solid Organ Transplant Recipients

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Blood Sampling
2.3. Humoral Response
2.4. Cellular Response
2.5. Statistical Analysis
3. Results
3.1. Patients with Natural Immunity
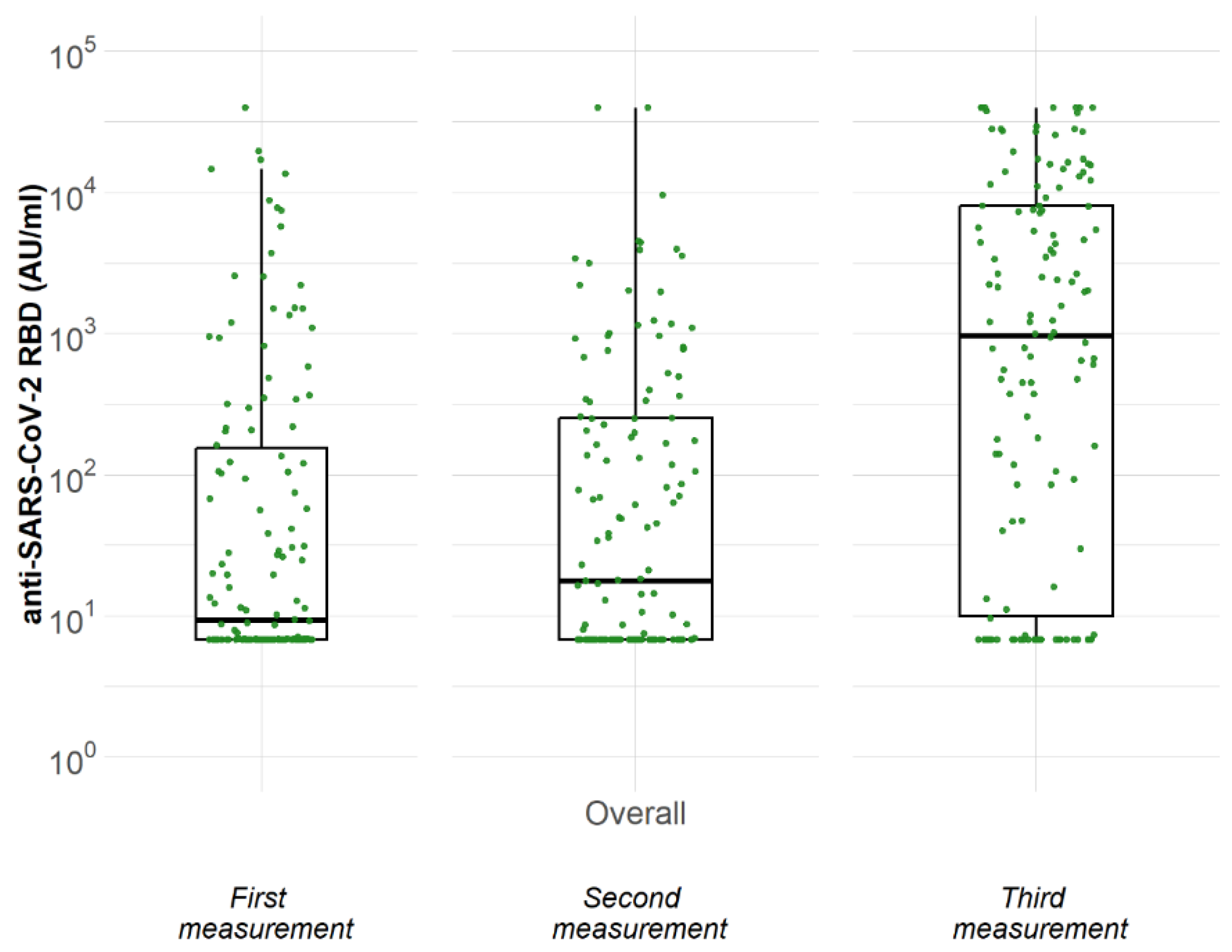
3.2. Humoral Response at Three Different Time Points
3.3. T-Cell Response before and after Booster Vaccination
3.4. Safety and Tolerability of the Third-Booster Dose
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/ (accessed on 19 December 2022).
- Ao, G.; Wang, Y.; Qi, X.; Nasr, B.; Bao, M.; Gao, M.; Sun, Y.; Xie, D. The association between severe or death COVID-19 and solid organ transplantation: A systematic review and meta-analysis. Transplant. Rev. 2021, 35, 100628. [Google Scholar] [CrossRef] [PubMed]
- Marinaki, S.; Tsiakas, S.; Korogiannou, M.; Grigorakos, K.; Papalois, V.; Boletis, I. A Systematic Review of COVID-19 Infection in Kidney Transplant Recipients: A Universal Effort to Preserve Patients’ Lives and Allografts. J. Clin. Med. 2020, 9, 2986. [Google Scholar] [CrossRef] [PubMed]
- Marinaki, S.; Adamopoulos, S.; Degiannis, D.; Roussos, S.; Pavlopoulou, I.D.; Hatzakis, A.; Boletis, I.N. Immunogenicity of SARS-CoV-2 BNT162b2 vaccine in solid organ transplant recipients. Am. J. Transplant. 2021, 21, 2913–2915. [Google Scholar] [CrossRef] [PubMed]
- Manuel, O.; Pascual, M.; Hoschler, K.; Giulieri, S.; Alves, D.; Ellefsen, K.; Bart, P.-A.; Venetz, J.-P.; Calandra, T.; Cavassini, M. Humoral response to the influenza A H1N1/09 monovalent AS03-adjuvanted vaccine in immunocompromised patients. Clin. Infect. Dis. 2011, 52, 248–256. [Google Scholar] [CrossRef]
- Eckerle, I.; Rosenberger, K.D.; Zwahlen, M.; Junghanss, T. Serologic vaccination response after solid organ transplantation: A systematic review. PLoS ONE 2013, 8, 56974. [Google Scholar] [CrossRef] [Green Version]
- Meshram, H.S.; Kute, V.; Rane, H.; Dave, R.; Banerjee, S.; Mishra, V.; Chauhan, S. Humoral and cellular response of COVID-19 vaccine among solid organ transplant recipients: A systematic review and meta-analysis. Transpl. Infect. Dis. 2022, 24, 13926. [Google Scholar] [CrossRef]
- Quiroga, B.; Soler, M.J.; Ortiz, A.; de Sequera, P. Lessons from SENCOVAC: A prospective study evaluating the response to SARS-CoV-2 vaccination in the CKD spectrum. Nefrología, 2022; in press. [Google Scholar] [CrossRef]
- Kamar, N.; Abravanel, F.; Marion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three Doses of an mRNA Covid-19 Vaccine in Solid-Organ Transplant Recipients. N. Engl. J. Med. 2021, 385, 661–662. [Google Scholar] [CrossRef]
- Stumpf, J.; Tonnus, W.; Paliege, A.; Ronny, R.; Anne, S.; Florian, G.; Friederike, K.; Hannah, K.; Patrick, A.; Jan, S.; et al. Cellular and Humoral Immune Responses after 3 Doses of BNT162b2 mRNA SARS-CoV-2 Vaccine in Kidney Transplant. Transplantation 2021, 105, E267–E269. [Google Scholar] [CrossRef]
- Reindl-Schwaighofer, R.; Heinzel, A.; Mayrdorfer, M.; Jabbour, R.; Hofbauer, T.M.; Merrelaar, A.; Eder, M.; Regele, F.; Doberer, K.; Spechtl, P.; et al. Comparison of SARS-CoV-2 Antibody Response 4 Weeks after Homologous vs Heterologous Third Vaccine Dose in Kidney Transplant Recipients: A Randomized Clinical Trial. JAMA Intern. Med. 2022, 182, 165–171. [Google Scholar] [CrossRef]
- Marinaki, S.; Degiannis, D.; Roussos, S.; Xagas, E.; Tsoutsoura, P.; Adamopoulos, S.; Sypsa, V.; Chaidaroglou, A.; Pavlopoulou, I.D.; Hatzakis, A.; et al. Head-to-Head Comparison of Response Rates to the Two mRNA SARS-CοV-2 Vaccines in a Large Cohort of Solid Organ Transplant (SOT) Recipients. Vaccines 2022, 10, 190. [Google Scholar] [CrossRef]
- Perkmann, T.; Perkmann-Nagele, N.; Breyer, M.K.; Breyer-Kohansal, R.; Burghuber, O.C.; Hartl, S.; Aletaha, D.; Sieghart, D.; Quehenberger, P.; Marculescu, R.; et al. Side-by-Side Comparison of Three Fully Automated SARS-CoV-2 Antibody Assays with a Focus on Specificity. Clin. Chem. 2020, 66, 1405–1413. [Google Scholar] [CrossRef] [PubMed]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 COVID-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef] [PubMed]
- Higashimoto, Y.; Kozawa, K.; Miura, H.; Kawamura, Y.; Ihira, M.; Hiramatsu, H.; Suzuki, R.; Haga, K.; Takai-Todaka, R.; Sawada, A.; et al. Correlation between anti-S IgG and neutralizing antibody titers against three live SARS-CoV-2 variants in BNT162b2 vaccine recipients. Hum. Vaccines Immunother. 2022, 18, 2105611. [Google Scholar] [CrossRef] [PubMed]
- Burbelo, P.D.; Riedo, F.X.; Morishima, C.; Rawlings, S.; Smith, D.; Das, S.; Strich, J.R.; Chertow, D.S.; Davey, R.T.; I Cohen, J. Sensitivity in Detection of Antibodies to Nucleocapsid and Spike Proteins of Severe Acute Respiratory Syndrome Coronavirus 2 in Patients with Coronavirus Disease 2019. J. Infect. Dis. 2020, 222, 206–213. [Google Scholar] [CrossRef]
- Alejo, J.L.; Mitchell, J.; Chiang, T.P.Y.; Abedon, A.T.B.; Sidoti, C.N.B.; Boyarsky, B.J.M.; Avery, R.K.; Tobian, A.A.M.; Levan, M.L.J.; Warren, D.S.; et al. Six-month Antibody Kinetics and Durability in SARS-CoV-2 mRNA Vaccinated Solid Organ Transplant Recipients. Transplantation 2022, 106, E109–E110. [Google Scholar] [CrossRef]
- Sakuraba, A.; Luna, A.; Micic, D. A Systematic Review and Meta-Analysis of Serologic Response following Coronavirus Disease 2019 (COVID-19) Vaccination in Solid Organ Transplant Recipients. Viruses 2022, 14, 1822. [Google Scholar] [CrossRef]
- Osmanodja, B.; Ronicke, S.; Budde, K.; Jens, A.; Hammett, C.; Koch, N.; Seelow, E.; Waiser, J.; Zukunft, B.; Bachmann, F.; et al. Serological Response to Three, Four and Five Doses of SARS-CoV-2 Vaccine in Kidney Transplant Recipients. J. Clin. Med. 2022, 11, 2565. [Google Scholar] [CrossRef]
- Kumar, D.; Hu, Q.; Samson, R.; Ferreira, V.H.; Hall, V.G.; Ierullo, M.; Majchrzak-Kita, B.; Hardy, W.; Gingras, A.-C.; Humar, A. Neutralization against Omicron variant in transplant recipients after three doses of mRNA vaccine. Am. J. Transplant. 2022, 22, 2089. [Google Scholar] [CrossRef]
- Tormo, N.; Giménez, E.; Martínez-Navarro, M.; Albert, E.; Navalpotro, D.; Torres, I.; Gimeno, C.; Navarro, D. Performance comparison of a flow cytometry immunoassay for intracellular cytokine staining and the QuantiFERON® SARS-CoV-2 test for detection and quantification of SARS-CoV-2-Spike-reactive-IFN-γ-producing T cells after COVID-19 vaccination. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 657–662. [Google Scholar] [CrossRef]
- Peled, Y.; Ram, E.; Lavee, J.; Segev, A.; Matezki, S.; Wieder-Finesod, A.; Halperin, R.; Mandelboim, M.; Indenbaum, V.; Levy, I.; et al. Third dose of the BNT162b2 vaccine in heart transplant recipients: Immunogenicity and clinical experience. J. Heart Lung Transplant. 2022, 41, 148. [Google Scholar] [CrossRef] [PubMed]
- Moga, E.; Lynton-Pons, E.; Domingo, P. The Robustness of Cellular Immunity Determines the Fate of SARS-CoV-2 Infection. Front. Immunol. 2022, 13, 3170. [Google Scholar] [CrossRef] [PubMed]
- Sekine, T.; Perez-Potti, A.; Rivera-Ballesteros, O.; Strålin, K.; Gorin, J.-B.; Olsson, A.; Llewellyn-Lacey, S.; Kamal, H.; Bogdanovic, G.; Muschiol, S.; et al. Robust T Cell Immunity in Convalescent Individuals with Asymptomatic or Mild COVID-19. Cell 2020, 183, 158–168.e14. [Google Scholar] [CrossRef]
- Crotty, S. Follicular Helper CD4 T Cells (TFH). Annu. Rev. Immunol. 2011, 29, 621–663. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, T.; Klemis, V.; Schub, D.; Schneitler, S.; Reichert, M.C.; Wilkens, H.; Sester, U.; Sester, M.; Mihm, J. Cellular immunity predominates over humoral immunity after homologous and heterologous mRNA and vector-based COVID-19 vaccine regimens in solid organ transplant recipients. Am. J. Transplant. 2021, 21, 3990–4002. [Google Scholar] [CrossRef]
- Korogiannou, M.; Vallianou, K.; Xagas, E.; Rokka, E.; Soukouli, I.; Boletis, I.N.; Marinaki, S. Disease Course, Management and Outcomes in Kidney Transplant Recipients with SARS-CoV-2 Infection during the Omicron-Variant Wave: A Single-Center Experience. Vaccines 2023, 11, 632. [Google Scholar] [CrossRef]
- Joint Statement about COVID-19 Vaccination in Organ Transplant Candidates and Recipients|American Society of Transplantation. Available online: https://www.myast.org/joint-statement-about-covid-19-vaccination-organ-transplant-candidates-and-recipients-0 (accessed on 29 December 2022).

{kind=link}
| N = 144 | |
|---|---|
| Gender, n (%) | |
| Male | 94 (65.3) |
| Female | 50 (34.7) |
| Age (years) mean (S.D.) 1 | 55.8 (13.8) |
| Age (years) median (25th, 75th) 2 | 56.5 (45.5, 68.7) |
| Age at transplantation (years) mean (S.D.) 1 | 45.1 (13.2) |
| Age at transplantation (years) median (25th, 75th) 2 | 46.5 (35.7, 55.0) |
| Time period between transplantation and second dose (years), median (25th, 75th) 2 | 9.3 (3.1, 16.1) |
| Time period between transplantation and second dose (years), n (%) | |
| <1 | 5 (3.5) |
| 1–9 | 64 (44.4) |
| >9 | 75 (52.1) |
| Organ transplant, n (%) | |
| Kidney | 136 (94.4) |
| Heart | 7 (4.9) |
| Kidney/Heart | 1 (0.7) |
| Kidney function | |
| Creatine (mg/dL) mean (S.D.) 1 | 1.5 (0.6) |
| Creatinine (mg/dL) Median (25th, 75th) 2 | 1.4 (1.1, 1.7) |
| eGFR (mL/min) mean (S.D.) 1 | 54.0 (18.7) |
| eGFR (mL/min) median (25th, 75th) 2 | 53 (42, 65) |
| Immunosuppression | |
| Tacrolimus, n (%) | |
| Yes | 109 (75.7) |
| No | 35 (24.3) |
| Tacrolimus levels (ng/mL) mean (S.D.) 1 | 6.0 (1.1) |
| Tacrolimus levels (ng/mL) median (25th, 75th) 2 | 6.0 (5.4, 6.7) |
| Mycophanolate acid, n (%) | |
| Yes | 125 (86.8) |
| No | 19 (13.2) |
| Azathioprine, n (%) | |
| Yes | 4 (2.8) |
| No | 140 (97.2) |
| Corticosteroids, n (%) | |
| Yes | 103 (71.5) |
| No | 41 (28.5) |
| Cyclosporine A, n (%) | |
| Yes | 35 (24.3) |
| No | 109 (75.7) |
| Everolimus, n (%) | |
| Yes | 14 (9.7) |
| No | 130 (90.3) |
| Everolimus levels (ng/mL) mean (S.D.) 1 | 5.7 (1.5) |
| Everolimus levels (ng/mL) median (25th, 75th) 2 | 5.9 (4.5, 6.6) |
| Vaccine Type for the first two doses, n (%) | |
| Pfizer–BioNTech | 94 (65.3) |
| Moderna | 50 (34.7) |
| Measurement N = 134 | |||
|---|---|---|---|
| First | Second | Third | |
| Antibodies (AU/mL), median (25th, 75th) 1 | 9 (7, 161) | 18 (7, 251) | 966 (10, 8027) |
| Antibody levels, n (%) | |||
| Negative (<50 AU/mL) | 89 (66.4) | 78 (58.2) | 41 (30.6) |
| Positive (≥50 AU/mL) | 45 (33.6) | 56 (41.8) | 93 (69.4) |
| Variable | Univariable RR (95% CI) | p-Value | Adjusted Multivariable RR (95% CI) | p-Value |
|---|---|---|---|---|
| Age (years) | 1.00 (0.99–1.01) | 0.614 | ||
| Age at transplantation (years) | 1.00 (1.00–1.01) | 0.283 | 1.01 (1.00–1.01) | 0.236 |
| Time from transplantation up to 2nd dose of vaccination (years) | 0.99 (0.98–1.01) | 0.382 | ||
| Gender | 0.145 | |||
| Male | Ref. | Ref. | ||
| Female | 0.83 (0.64–1.07) | 0.80 | 0.066 | |
| Vaccine | 0.204 | |||
| Pfizer/Biontech | Ref. | |||
| Moderna | 1.15 (0.92–1.44) | |||
| CNI = (Tacrolimus + Cyclosporine) | 0.698 | |||
| Yes | Ref. | |||
| No | 0.92 (0.61–1.40) | |||
| Mycophenolic Acid | <0.001 | <0.001 | ||
| Yes | Ref. | Ref. | ||
| No | 1.55 (1.35–1.77) | 1.48 (1.24–1.77) | ||
| Corticosteroids | 0.001 | 0.048 | ||
| Yes | Ref. | Ref. | ||
| No | 1.40 (1.15–1.71) | 1.24 (1.00–1.53) | ||
| Everolimus | 0.001 | |||
| Yes | Ref. | |||
| No | 0.72 (0.59–0.87) | |||
| Organ transplanted | <0.001 | |||
| Kidney | Ref. | |||
| Heart | 1.48 (1.31–1.67) |
| Cell Immunity | After 3rd Dose | ||
|---|---|---|---|
| Before 3rd Dose | No | Yes | Total |
| No | 23 (100.0%) | 12 (70.6%) | 35 (87.5%) |
| Yes | 0 (0.0%) | 5 (29.4%) | 5 (12.5%) |
| Total | 23 (100.0%) | 17 (100.0%) | 40 (100.0%) |
| Cell Immunity | |||
|---|---|---|---|
| Antibody levels after 3rd dose | No | Yes | Total |
| Negative (<50 AU/mL) | 11 (37.9%) | 4 (19.0%) | 15 (30.0%) |
| Positive (≥50 AU/mL) | 18 (62.1%) | 17 (81.0%) | 35 (70.0%) |
| Total | 29 (100.0%) | 21 (100.0%) | 50 (100.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsoutsoura, P.; Xagas, E.; Roussos, S.; Hatzakis, A.; Gourzi, P.; Boletis, I.N.; Marinaki, S. Assessment of mRNA Vaccine Immunogenicity in Solid Organ Transplant Recipients. Medicina 2023, 59, 1075. https://doi.org/10.3390/medicina59061075
Tsoutsoura P, Xagas E, Roussos S, Hatzakis A, Gourzi P, Boletis IN, Marinaki S. Assessment of mRNA Vaccine Immunogenicity in Solid Organ Transplant Recipients. Medicina. 2023; 59(6):1075. https://doi.org/10.3390/medicina59061075
Chicago/Turabian StyleTsoutsoura, Paraskevi, Efstathios Xagas, Sotirios Roussos, Angelos Hatzakis, Polyxeni Gourzi, Ioannis N. Boletis, and Smaragdi Marinaki. 2023. "Assessment of mRNA Vaccine Immunogenicity in Solid Organ Transplant Recipients" Medicina 59, no. 6: 1075. https://doi.org/10.3390/medicina59061075