

Influence of Patient-Reported Outcome Measures by Surgical Versus Conservative Management in Adult Ankle Fractures: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Inclusion and Exclusion Criteria of Literature
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
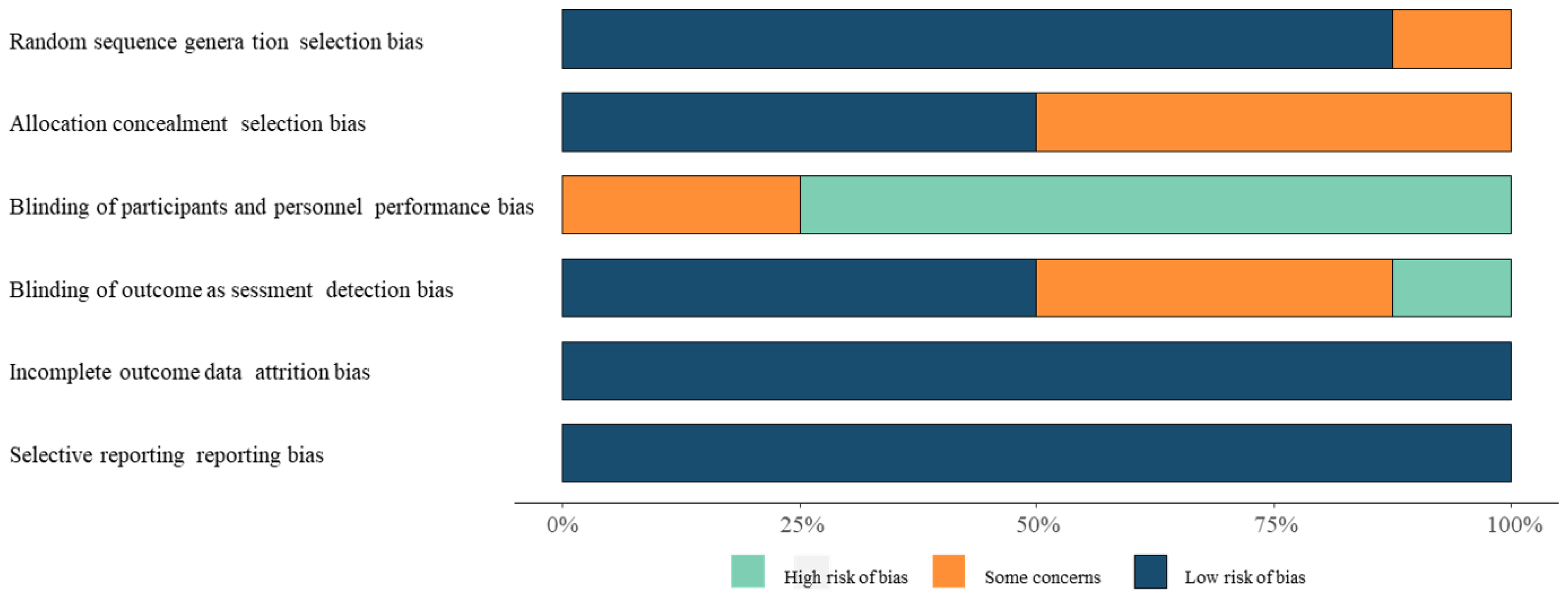
2.3. Quality Assessment
2.4. Data Extraction
2.5. Statistical Methods
3. Results
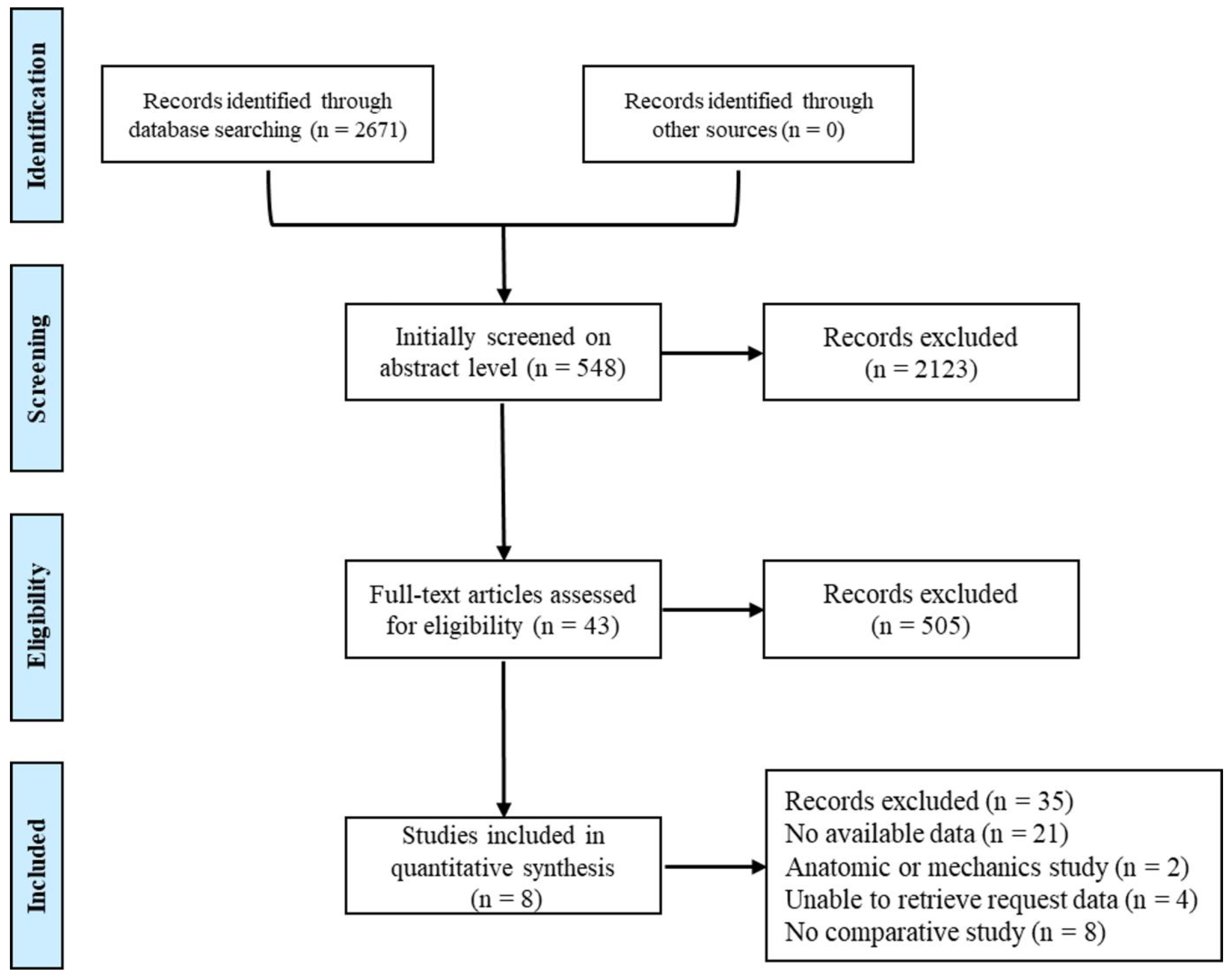
3.1. Results of the Literature Search and Intervention Studies
3.2. OMAS Analysis
3.2.1. OMAS Analysis after 6 Months of Treatment
3.2.2. OMAS Analysis after 12–24 Months of Treatment
3.2.3. OMAS Analysis after 24 Months of Treatment
3.3. SF-12 Analysis
3.3.1. SF12-Physical Analysis
3.3.2. SF12-Mental Analysis
3.4. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scheer, R.C.; Newman, J.M.; Zhou, J.J.; Oommen, A.J.; Naziri, Q.; Shah, N.V.; Pascal, S.C.; Penny, G.S.; McKean, J.M.; Tsai, J.; et al. Ankle Fracture Epidemiology in the United States: Patient-Related Trends and Mechanisms of Injury. J. Foot Ankle Surg. 2020, 59, 479–483. [Google Scholar] [CrossRef]
- Balasubramanian, A.; Zhang, J.; Chen, L.; Wenkert, D.; Daigle, S.G.; Grauer, A.; Curtis, J.R. Risk of subsequent fracture after prior fracture among older women. Osteoporos. Int. 2019, 30, 79–92. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Lin, J.; Hamid, K.S.; Bohl, D.D. Deltoid Ligament Rupture in Ankle Fracture: Diagnosis and Management. J. Am. Acad. Orthop. Surg. 2019, 27, e648–e658. [Google Scholar] [CrossRef] [PubMed]
- Kyriacou, H.; Mostafa, A.; Davies, B.M.; Khan, W.S. Principles and guidelines in the management of ankle fractures in adults. J. Perioper. Pract. 2021, 31, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Claessen, F.M.; Meijer, D.T.; van den Bekerom, M.P.; Gevers Deynoot, B.D.; Mallee, W.H.; Doornberg, J.N.; van Dijk, C.N. Reliability of classification for post-traumatic ankle osteoarthritis. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1332–1337. [Google Scholar] [CrossRef] [Green Version]
- Hsu, R.Y.; Ramirez, J.M.; Blankenhorn, B.D. Surgical Considerations for Osteoporosis in Ankle Fracture Fixation. Orthop. Clin. N. Am. 2019, 50, 245–258. [Google Scholar] [CrossRef]
- Ortiz, C.A.; Wagner, P.; Wagner, E. State-of-the-Art in Ankle Fracture Management in Chile. Foot Ankle Clin. 2016, 21, 367–389. [Google Scholar] [CrossRef]
- Canton, G.; Sborgia, A.; Maritan, G.; Fattori, R.; Roman, F.; Tomic, M.; Morandi, M.M.; Murena, L. Fibula fractures management. World J. Orthop. 2021, 12, 254–269. [Google Scholar] [CrossRef]
- Aiyer, A.A.; Zachwieja, E.C.; Lawrie, C.M.; Kaplan, J.R.M. Management of Isolated Lateral Malleolus Fractures. J. Am. Acad. Orthop. Surg. 2019, 27, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Vanderkarr, M.F.; Ruppenkamp, J.W.; Vanderkarr, M.; Parikh, A.; Holy, C.E.; Putnam, M. Incidence, costs and post-operative complications following ankle fracture—A US claims database analysis. BMC Musculoskelet. Disord. 2022, 23, 1129. [Google Scholar] [CrossRef]
- Bariteau, J.T.; Hsu, R.Y.; Mor, V.; Lee, Y.; DiGiovanni, C.W.; Hayda, R. Operative versus nonoperative treatment of geriatric ankle fractures: A Medicare Part A claims database analysis. Foot Ankle Int. 2015, 36, 648–655. [Google Scholar] [CrossRef]
- Blom, R.P.; Meijer, D.T.; de Muinck Keizer, R.O.; Stufkens, S.A.S.; Sierevelt, I.N.; Schepers, T.; Kerkhoffs, G.; Goslings, J.C.; Doornberg, J.N. Posterior malleolar fracture morphology determines outcome in rotational type ankle fractures. Injury 2019, 50, 1392–1397. [Google Scholar] [CrossRef]
- Zelle, B.A.; Bhandari, M.; Espiritu, M.; Koval, K.J.; Zlowodzki, M. Treatment of distal tibia fractures without articular involvement: A systematic review of 1125 fractures. J. Orthop. Trauma 2006, 20, 76–79. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Makwana, N.K.; Bhowal, B.; Harper, W.M.; Hui, A.W. Conservative versus operative treatment for displaced ankle fractures in patients over 55 years of age. A prospective, randomised study. J. Bone J. Surg. Br. 2001, 83, 525–529. [Google Scholar] [CrossRef]
- Willett, K.; Keene, D.J.; Mistry, D.; Nam, J.; Tutton, E.; Handley, R.; Morgan, L.; Roberts, E.; Briggs, A.; Lall, R.; et al. Close Contact Casting vs Surgery for Initial Treatment of Unstable Ankle Fractures in Older Adults: A Randomized Clinical Trial. JAMA 2016, 316, 1455–1463. [Google Scholar] [CrossRef] [PubMed]
- Parry, J.A.; Peterson, S.L.; Strage, K.E.; Hadeed, M.; Heare, A.; Stacey, S.C.; Mauffrey, C. Percent of Normal: A Pragmatic Patient-Reported Outcome Measure for the Orthopaedic Trauma Clinic. J. Orthop. Trauma 2021, 35, e429–e432. [Google Scholar] [CrossRef] [PubMed]
- Mittal, R.; Harris, I.A.; Adie, S.; Naylor, J.M. Surgery for Type B Ankle Fracture Treatment: A Combined Randomised and Observational Study (CROSSBAT). BMJ Open 2017, 7, e013298. [Google Scholar] [CrossRef]
- Lehtola, R.; Leskelä, H.V.; Flinkkilä, T.E.; Pakarinen, H.J.; Niinimäki, J.L.; Ohtonen, P.P.; Kortekangas, T.H. Syndesmosis fixation in supination-external rotation ankle fractures. Long-Term results of a prospective randomised study. Foot Ankle Surg. 2022, 28, 229–234. [Google Scholar] [CrossRef]
- Keene, D.J.; Mistry, D.; Nam, J.; Tutton, E.; Handley, R.; Morgan, L.; Roberts, E.; Gray, B.; Briggs, A.; Lall, R.; et al. The Ankle Injury Management (AIM) trial: A pragmatic, multicentre, equivalence randomised controlled trial and economic evaluation comparing close contact casting with open surgical reduction and internal fixation in the treatment of unstable ankle fractures in patients aged over 60 years. Health Technol. Assess. 2016, 20, 1–158. [Google Scholar]
- Hoelsbrekken, S.E.; Kaul-Jensen, K.; Mørch, T.; Vika, H.; Clementsen, T.; Paulsrud, Ø.; Petursson, G.; Stiris, M.; Strømsøe, K. Nonoperative treatment of the medial malleolus in bimalleolar and trimalleolar ankle fractures: A randomized controlled trial. J. Orthop. Trauma 2013, 27, 633–637. [Google Scholar] [CrossRef]
- Toth, M.J.; Yoon, R.S.; Liporace, F.A.; Koval, K.J. What’s new in ankle fractures. Injury 2017, 48, 2035–2041. [Google Scholar] [CrossRef] [PubMed]
- Michelson, J.D.; Wright, M.; Blankstein, M. Syndesmotic Ankle Fractures. J. Orthop. Trauma 2018, 32, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Smeeing, D.P.J.; Houwert, R.M.; Briet, J.P.; Groenwold, R.H.H.; Lansink, K.W.W.; Leenen, L.P.H.; van der Zwaal, P.; Hoogendoorn, J.M.; van Heijl, M.; Verleisdonk, E.J.; et al. Weight-bearing or non-weight-bearing after surgical treatment of ankle fractures: A multicenter randomized controlled trial. Eur. J. Trauma Emerg. Surg. 2020, 46, 121–130. [Google Scholar] [CrossRef] [Green Version]
- Kortekangas, T.; Haapasalo, H.; Flinkkilä, T.; Ohtonen, P.; Nortunen, S.; Laine, H.J.; Järvinen, T.L.; Pakarinen, H. Three week versus six week immobilisation for stable Weber B type ankle fractures: Randomised, multicentre, non-inferiority clinical trial. BMJ 2019, 364, k5432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumann, A.P.; Rammelt, S. Ankle fractures involving the posterior malleolus: Patient characteristics and 7-year results in 100 cases. Arch. Orthop. Trauma Surg. 2021, 142, 1823–1834. [Google Scholar] [CrossRef] [PubMed]
- Bullock, T.S.; Gutierrez-Naranjo, J.M.; DelBello, R.G.; Karia, R.A.; Zelle, B.A. Outpatient surgery in patients with ankle fractures minimises hospital admissions and utilisation of healthcare resources. Int. Orthop. 2021, 45, 2395–2400. [Google Scholar] [CrossRef]
- Balaji, G.; Bhukya, S.; Nema, S.; Rajeswari, M.; Vellaipandi, V. Predictors of Functional Outcome in Unstable Ankle Fractures Treated Surgically—A Prospective Cohort Study. Malays. Orthop. J. 2021, 15, 85–92. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Gender (Male/Female) | Age | Surgery | Non-Surgery | Main Indicators |
|---|---|---|---|---|---|---|
| Makwana NK [20] | 2001 | 12/31 | 66 (57 to 77) | 22 | 21 | OMAS |
| Willett K [21] | 2016 | 160/460 | 70.2 ± 7.4 | 309 | 311 | SF-12, OMAS |
| Keene DJ [22] | 2018 | 119/331 | 69.6 ± 6.7 | 226 | 224 | SF-12, OMAS |
| Mittal R [23] | 2017 | 56/104 | 38.9 ± 13.3 | 72 | 69 | SF-12 |
| Sanders DW [24] | 2012 | 41/40 | 41 | 41 | 40 | OMAS |
| Lehtola R [25] | 2022 | 15/9 | 43.6 ± 12.6 | 13 | 11 | OMAS |
| Keene DJ [26] | 2016 | 180/280 | 69.6 ± 11.2 | 309 | 311 | SF-12, OMAS |
| Hoelsbrekken SE [27] | 2013 | 31/51 | 52.8 ± 15.7 | 37 | 45 | OMAS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peng, H.; Guo, X.-B.; Zhao, J.-M. Influence of Patient-Reported Outcome Measures by Surgical Versus Conservative Management in Adult Ankle Fractures: A Systematic Review and Meta-Analysis. Medicina 2023, 59, 1152. https://doi.org/10.3390/medicina59061152
Peng H, Guo X-B, Zhao J-M. Influence of Patient-Reported Outcome Measures by Surgical Versus Conservative Management in Adult Ankle Fractures: A Systematic Review and Meta-Analysis. Medicina. 2023; 59(6):1152. https://doi.org/10.3390/medicina59061152
Chicago/Turabian StylePeng, Hui, Xiao-Bo Guo, and Jin-Min Zhao. 2023. "Influence of Patient-Reported Outcome Measures by Surgical Versus Conservative Management in Adult Ankle Fractures: A Systematic Review and Meta-Analysis" Medicina 59, no. 6: 1152. https://doi.org/10.3390/medicina59061152