
Cervical Cancer and Human Papillomavirus Awareness among Women in Antigua and Barbuda

 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Study Setting and Study Population
2.3. Data Collection and Questionnaires
2.4. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Cancer Observatory—International Agency for Research on Cancer. Available online: https://gco.iarc.fr/ (accessed on 31 May 2023).
- PAHO/WHO|Pan American Health Organization. Antigua and Barbuda Advances towards the Elimination of Cervical Cancer as a Public Health Problem. (n.d.). Available online: https://www.paho.org/en/news/3-8-2022-antigua-and-barbuda-advances-towards-elimination-cervical-cancer-public-health (accessed on 2 May 2023).
- Okunade, K.S. Human papillomavirus and cervical cancer. J. Obstet. Gynaecol. 2020, 40, 602–608. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Mabuchi, S.; Okazawa, M.; Kawano, M.; Kuroda, H.; Kamiura, S.; Kimura, T. Clinical implication of surgically treated early-stage cervical cancer with multiple high-risk factors. J. Gynecol. Oncol. 2015, 26, 3–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiffman, M.; Castle, P.E.; Jeronimo, J.; Rodriguez, A.C.; Wacholder, S. Human papillomavirus and cervical cancer. Lancet 2007, 370, 890–907. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Parkin, D.M.; Almonte, M.; Bruni, L.; Clifford, G.; Curado, M.P.; Piñeros, M. Burden and trends of type-specific human papillomavirus infections and related diseases in the latin america and Caribbean region. Vaccine 2008, 26 (Suppl 11), L1–L15. [Google Scholar] [CrossRef] [PubMed]
- You, D.; Han, L.; Li, L.; Hu, J.; Zimet, G.D.; Alias, H.; Danaee, M.; Cai, L.; Zeng, F.; Wong, L.P. Human Papillomavirus (HPV) Vaccine Uptake and the Willingness to Receive the HPV Vaccination among Female College Students in China: A Multicenter Study. Vaccines 2020, 8, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, S.; Adams, S. How Much Do You Know about Cervical Cancer?—Ministry of Health, Wellness and Environment. Ministry of Health, Wellness and Environment. Government of Antigua and Barbuda. 25 January 2023. Available online: https://health.gov.ag/elementor-9771/#:~:text=HPV%20vaccines%20are%20currently%20available,all%20clinics%20free%20of%20charge (accessed on 2 May 2023).
- Lwanga, S.K.; Lemeshow, S. Sample Size Determination in Health Studies: A Practical Manual; World Health Organization: Geneva, Switzerland, 1991. [Google Scholar]
- Qualtrics, X.M. Experience Management Software. 28 April 2023. Qualtrics. Available online: https://www.qualtrics.com/ (accessed on 2 May 2023).
- Yu, Y.; Xu, M.; Sun, J.; Li, R.; Li, M.; Wang, J.; Zhang, D.; Xu, A. Human Papillomavirus Infection and Vaccination: Awareness and Knowledge of HPV and Acceptability of HPV Vaccine among Mothers of Teenage Daughters in Weihai, Shandong, China. PLoS ONE 2016, 11, e0146741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, N.; Alcalá, H.E.; Anderson, R.; Balkrishnan, R. Cancer Disparities in Rural Appalachia: Incidence, Early Detection, and Survivorship. J. Rural. Health 2017, 33, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Guan, P.; Howell-Jones, R.; Li, N.; Bruni, L.; de Sanjosé, S.; Franceschi, S.; Clifford, G.M. Human papillomavirus types in 115,789 HPV-positive women: A meta-analysis from cervical infection to cancer. Int. J. Cancer 2012, 131, 2349–2359. [Google Scholar] [CrossRef] [PubMed]
- Richardson, L.A.; Tota, J.; Franco, E.L. Optimizing technology for cervical cancer screening in high-resource settings. Expert. Rev. Obstet. Gynecol. 2011, 6, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Onon, T.S.; Kitchener, H.C. The use of vaccines in treating cervical cancer: Present status and future prospects. Int. J. Gynecol. Cancer 1999, 9, 265–278. [Google Scholar] [CrossRef] [PubMed]
- Antigua and Barbuda—Country Profile. Health in the Americas. 4 April 2023. Available online: https://hia.paho.org/en/countries-22/antigua-barbuda-country-profile (accessed on 2 May 2023).
- Marlow, L.A.; Zimet, G.D.; McCaffery, K.J.; Ostini, R.; Waller, J. Knowledge of human papillomavirus (HPV) and HPV vaccination: An international comparison. Vaccine 2013, 31, 763–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warner, Z.C.; Reid, B.; Auguste, P.; Joseph, W.; Kepka, D.; Warner, E.L. Awareness and Knowledge of HPV, HPV Vaccination, and Cervical Cancer among an Indigenous Caribbean Community. Int. J. Environ. Res. Public Health 2022, 19, 5694. [Google Scholar] [CrossRef] [PubMed]
- Dodd, R.H.; McCaffery, K.J.; Marlow, L.A.; Ostini, R.; Zimet, G.D.; Waller, J. Knowledge of human papillomavirus (HPV) testing in the USA, the UK and Australia: An international survey. Sex. Transm. Infect. 2014, 90, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowyer, H.L.; Forster, A.S.; Marlow, L.A.; Waller, J. Predicting human papillomavirus vaccination behaviour among adolescent girls in England: Results from a prospective survey. J. Fam. Plan. Reprod. Health Care 2014, 40, 14–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pitts, M.K.; Heywood, W.; Ryall, R.; Smith, A.M.; Shelley, J.M.; Richters, J.; Simpson, J.M. Knowledge of human papillomavirus (HPV) and the HPV vaccine in a national sample of Australian men and women. Sex. Health 2010, 7, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Makwe, C.C.; Anorlu, R.I.; Odeyemi, K.A. Human papillomavirus (HPV) infection and vaccines: Knowledge, attitude and perception among female students at the University of Lagos, Lagos, Nigeria. J. Epidemiol. Glob. Health 2012, 2, 199–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raçi, P.Z.; Raçi, F.; Hadri, T. Kosovo women’s knowledge and awareness of human papillomavirus (HPV) infection, HPV vaccination, and its relation to cervical cancer. BMC Womens Health 2021, 21, 354. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Number of Responders | Category | Frequency (Total 464) | Percentage (%) |
|---|---|---|---|---|
| Age in years | 467 | 18 to 28 | 76 | 16.3 |
| 29 to 38 | 108 | 23.1 | ||
| 39 to 48 | 101 | 21.6 | ||
| 49 to 58 | 113 | 24.2 | ||
| >59 | 69 | 14.8 | ||
| Marital status | 466 | Single | 233 | 50 |
| Married | 139 | 29.8 | ||
| Living with partner | 40 | 8.6 | ||
| Divorced | 34 | 7.3 | ||
| Widowed | 9 | 1.9 | ||
| others | 11 | 2.4 | ||
| Race or ethnicity | 466 | Afro-Caribbean | 395 | 84.8 |
| White-Caribbean | 23 | 4.9 | ||
| Indo-Caribbean | 7 | 1.5 | ||
| Hispanic | 3 | 0.6 | ||
| Others | 38 | 8.2 | ||
| Education | 464 | Primary school | 21 | 4.5 |
| High school | 110 | 23.7 | ||
| Some college | 105 | 22.6 | ||
| College graduate or higher | 228 | 49.1 | ||
| Visited health care provider in the last year | 462 | Yes | 369 | 79.9 |
| No | 85 | 18.4 | ||
| Don’t remember | 8 | 1.7 | ||
| Health insurance | 462 | Yes | 240 | 51.9 |
| No | 218 | 47.2 | ||
| Don’t remember | 4 | 0.9 |
| Variable | Number of Responders | Category | Frequency | Percentage (%) |
|---|---|---|---|---|
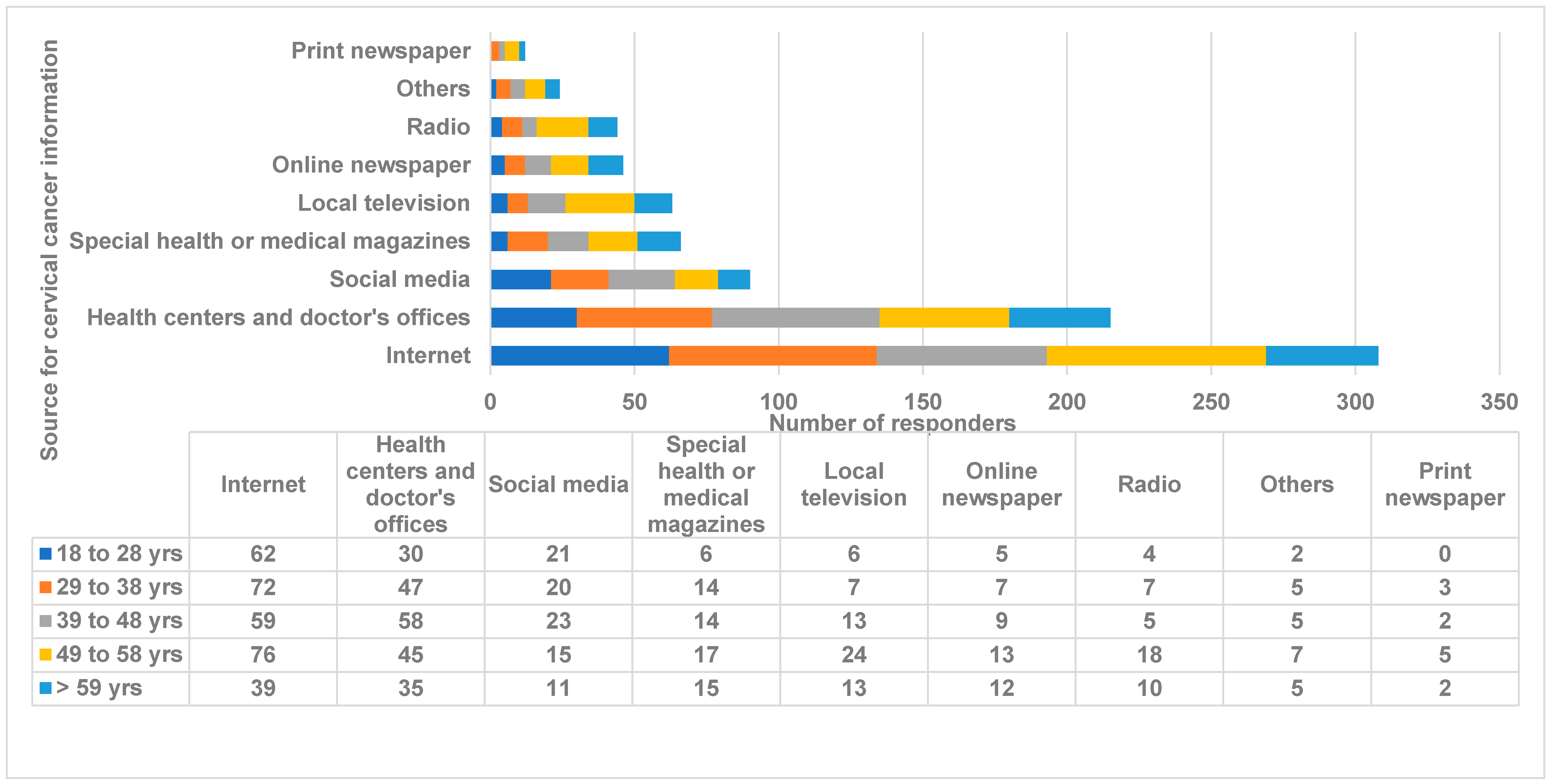
| Source of cervical cancer information | 451 | Online newspaper | 46 | 10.2 |
| Print newspaper | 12 | 2.7 | ||
| Special health or medical magazines | 66 | 14.6 | ||
| Radio | 44 | 9.8 | ||
| Local television | 63 | 14 | ||
| Internet | 308 | 68.3 | ||
| Social media | 90 | 20 | ||
| Health centers and doctor’s offices | 215 | 47.7 | ||
| Others | 24 | 5.3 | ||
| Heard of HPV | 450 | Yes | 412 | 91.6 |
| No | 38 | 8.4 | ||
| HPV causes cervical cancer | 450 | Yes | 318 | 70.7 |
| No | 21 | 4.7 | ||
| Don’t know | 111 | 24.7 | ||
| HPV is sexually transmitted | 450 | Yes | 255 | 56.7 |
| No | 91 | 20.2 | ||
| Don’t know | 104 | 23.1 | ||
| HPV infects both men and women | 449 | Yes | 291 | 64.8 |
| No | 64 | 14.3 | ||
| Don’t know | 94 | 20.9 | ||
| The HPV vaccine protects against HPV | 446 | Yes | 315 | 70.6 |
| No | 28 | 6.3 | ||
| Don’t know | 103 | 23.1 | ||
| Vaccinated against HPV | 446 | Yes | 57 | 12.8 |
| No | 389 | 87.2 | ||
| Parents/friends approve of you getting vaccinated against HPV | 389 | Approve | 204 | 52.4 |
| Disapprove | 16 | 4.1 | ||
| Don’t know | 169 | 43.4 | ||
| Barrier for getting the HPV vaccination | 386 | Religion | 7 | 1.8 |
| Worried about side effects | 85 | 22 | ||
| Accessibility | 18 | 4.7 | ||
| Too expensive/no insurance/cost | 17 | 4.4 | ||
| Doctor didn’t tell me about it | 116 | 30.1 | ||
| Not required | 45 | 11.7 | ||
| Laziness | 18 | 4.7 | ||
| I am over the eligible age group (more than 45 years) | 151 | 39.1 | ||
| Others | 42 | 10.9 | ||
| Willingness to get the HPV vaccine | 386 | Yes | 192 | 49.7 |
| No | 98 | 25.4 | ||
| Don’t know | 96 | 24.9 | ||
| Heard of the Pap smear | 440 | Yes | 435 | 98.9 |
| No | 5 | 1.1 | ||
| When was the last Pap smear received | 435 | Never | 53 | 12.2 |
| Within the last 6 to 10 years | 58 | 13.3 | ||
| Within the last 4 to 5 years | 47 | 10.8 | ||
| Within the last 3 years | 277 | 63.7 | ||
| Reason for not getting a Pap smear | 53 | Too young | 16 | 30.2 |
| No reason/never thought about it | 15 | 28.3 | ||
| Laziness | 5 | 7.5 | ||
| Not required | 4 | 9.4 | ||
| Too expensive/no insurance/cost | 2 | 3.8 | ||
| Working hours collides with testing time | 2 | 3.8 | ||
| Too painful, unpleasant | 1 | 1.9 | ||
| Embarrassing | 1 | 1.9 | ||
| Not so easily available | 1 | 1.9 | ||
| Others | 6 | 11.3 | ||
| Women who received the HPV vaccine and still required periodic Pap smears | 433 | True | 314 | 72.5 |
| False | 15 | 3.5 | ||
| Don’t know | 104 | 24 | ||
| Would you like to get more information about HPV and the HPV vaccine | 435 | Agree | 335 | 77 |
| Disagree | 55 | 12.6 | ||
| Don’t know | 45 | 10.3 | ||
| How do you decrease the risk of getting HPV infection | 433 | Avoiding sex | 142 | 32.8 |
| Vaccination | 277 | 64 | ||
| Using condoms | 221 | 51 | ||
| Antibiotics | 38 | 8.8 | ||
| Herbal medication | 40 | 9.2 | ||
| Don’t know | 86 | 19.9 |
| Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age in years | 0.455 | 0.0814 | 0.188 | 0.626 | 0.272 | <0.00001 * | 0.743 | <0.00001 * | 0.0785 | <0.00001 * | 0.003 * | 0.379 | 0.001 * |
| Marital status | 0.164 | <0.00001 * | 0.202 | 0.0710 | 0.0563 | 0.0572 | 0.651 | 0.299 | 0.409 | 0.00001 * | 0.261 | 0.397 | 0.507 |
| Race or ethnicity | 0.138 | 0.931 | 0.973 | 0.614 | 0.562 | 0.348 | 0.730 | 0.453 | 0.02 * | 0.989 | 0.949 | 0.973 | 0.367 |
| Education | 0.001 * | 0.0004 * | <0.00001 * | 0.0779 | <0.00001 * | 0.0643 | 0.492 | 0.653 | 0.186 | 0.07 | 0.763 | <0.00001 * | 0.129 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Honnavar, P.; Mansoor, E.; Tulloch, C.; Udayan, U.; Cosmello, I.; Patel, P.; Bersma, A. Cervical Cancer and Human Papillomavirus Awareness among Women in Antigua and Barbuda. Medicina 2023, 59, 1230. https://doi.org/10.3390/medicina59071230
Honnavar P, Mansoor E, Tulloch C, Udayan U, Cosmello I, Patel P, Bersma A. Cervical Cancer and Human Papillomavirus Awareness among Women in Antigua and Barbuda. Medicina. 2023; 59(7):1230. https://doi.org/10.3390/medicina59071230
Chicago/Turabian StyleHonnavar, Prasanna, Edmond Mansoor, Cherie Tulloch, Uttam Udayan, Isabella Cosmello, Purva Patel, and Ashley Bersma. 2023. "Cervical Cancer and Human Papillomavirus Awareness among Women in Antigua and Barbuda" Medicina 59, no. 7: 1230. https://doi.org/10.3390/medicina59071230