Abstract
Background and Objectives: Overweight/obesity puts individuals at greater risk for COVID-19 progression and mortality. We aimed to evaluate the impact of overweight/obesity on oxygen (O2) requirement outcomes of male and female kidney transplant recipients (KTRs) during the COVID-19 pandemic. Materials and Methods: We conducted a retrospective analysis of a cohort of KTRs diagnosed with COVID-19. Participants were stratified based on BMI categories, and data on the need for O2 therapy outcome were collected and analyzed separately for male and female KTRs. Results: In total, 284 KTRs (97 males and 187 females) were included in the study. Overweight/obesity was observed in 60.6% of male KTRs and 71% of female KTRs. Strikingly, overweight/obese women had a significantly higher requirement for supplemental O2 (63.3% vs. 41.7%, OR = 2.45, p = 0.03), particularly among older individuals (OR = 1.05, p = 0.04), smokers (OR = 4.55, p = 0.03), those with elevated lactate dehydrogenase (LDH) levels (OR = 1.01, p = 0.006), and those with lower admission and basal estimated glomerular filtration rate (eGFR) levels. Within this cohort, the necessity for O2 supplementation was correlated with more unfavorable outcomes. These included heightened mortality rates, transfers to the intensive care unit, employment of invasive mechanical ventilation, and the emergence of acute kidney injury requiring hemodialysis. On the other hand, although overweight/obese male KTRs had a higher prevalence of hypertension and higher fasting blood glucose levels, no significant association was found with COVID-19-related outcomes when compared to lean male KTRs. Conclusions: Overweight/obesity is highly prevalent in KTRs, and overweight/obese women demonstrated a higher need for supplemental O2. Therefore, the early identification of factors that predict a worse outcome in overweight/obese female KTRs affected by COVID-19 contributes to risk stratification and guides therapeutic decisions.
1. Introduction
Kidney transplant recipients (KTRs) face a significantly higher risk for severe COVID-19 outcomes, leading to increased mortality rates compared to the general population [1]. These concerning findings highlight the importance of comprehending the specific challenges encountered by KTRs during the pandemic. Our group has previously demonstrated that KTRs possess high rates of comorbidities, such as hypertension [2], diabetes mellitus (DM) [3], and overweight/obesity [4]. These comorbidities further compound the susceptibility of KTRs to severe COVID-19 complications, making tailored care strategies essential.
Obesity is an independent risks factor for the severity of COVID-19 [5]. Researchers have highlighted that obesity exacerbates the inflammatory response and hampers lung function, thereby contributing to the manifestation of more severe respiratory symptoms and prolonged viral shedding [5,6].
Obesity is a key component of metabolic syndrome, a cluster of metabolic abnormalities that often occur together and increase the risk of cardiovascular disease and type 2 DM [7]. In the context of metabolic syndrome, obesity contributes to the development of insulin resistance, dyslipidemia, and hypertension. Excess adipose tissue produces hormones and inflammatory molecules that disrupt insulin signaling and promote a chronic low-grade inflammatory state [8]. This combination of factors significantly raises the risk of cardiovascular complications and the development of DM. Therefore, managing obesity is essential in addressing metabolic syndrome and reducing the associated health risks [9].
Additionally, COVID-19 outcomes have shown notable differences between men and women. Several studies have highlighted that men tend to experience more severe illness, including higher rates of hospitalization, intensive care unit admission, and mortality compared to women [10]. Men have been observed to have more severe respiratory symptoms, greater systemic inflammation, and a higher prevalence of comorbidities such as hypertension and cardiovascular disease [10,11]. On the other hand, women appear to mount more robust immune responses, have lower mortality rates, and may exhibit milder manifestations of the disease. Underlying biological, genetic, and hormonal factors likely contribute to these sex-based differences in COVID-19 outcomes [12]. Understanding and addressing these disparities is crucial for developing targeted strategies for prevention, treatment, and care that consider the unique characteristics and susceptibilities of both men and women affected by COVID-19.
In our previous study, we established that body mass index (BMI) was an independent risk factor for oxygen (O2) requirement, particularly among overweight/obese KTRs who were older, smokers, and exhibited higher levels of lactate dehydrogenase (LDH), as well as lower levels of estimated glomerular filtration rate (eGFR), lymphocytes, and sodium at admission [4]. Therefore, this follow-up investigation aims to delve deeper into the differences between overweight/obese male and female KTRs, shedding light on crucial risk factors associated with O2 requirement.
2. Patients and Methods
2.1. Study Design and Setting
We conducted a cohort, cross-sectional, observational, and descriptive study at Hospital do Rim, São Paulo, SP, Brazil. The medical records of patients who were either hospitalized or non-hospitalized with the diagnosis of COVID-19 during the study period of March to August 2020 were evaluated, corresponding to the first wave of COVID-19 in Brazil. We included only patients in whom nasopharyngeal swab RT-PCR (reverse transcriptase-polymerase chain reaction) detected SARS-CoV-2. The population at risk included 11,875 KTRs. Of 590 KTRs who became ill, 284 were included in the study, as previously described [2]. The remaining patients were excluded due to admission to other services. Data were collected regarding patient demographics and laboratory parameters on admission with COVID-19 symptoms. The last patient was included in the study on 30 August 2020. The Ethics and Research Committee of the Federal University of São Paulo (CAEE 35311020.9.0000.8098) approved the study (30 March 2020). Informed consent was obtained from all patients, whereas a waiver was granted for patients who died in other hospitals.
Patient demographics included age, sex, race, body mass index (BMI), time of transplant, type of donor, as well as the presence of comorbidities (hypertension, DM, smoking, chronic obstructive pulmonary disease [COPD], heart disease, liver disease, and autoimmune disease).
Hypertension was defined whether individuals were on anti-hypertensive drugs, DM was defined according to the use of insulin and/or oral antidiabetics, heart disease whether heart failure and/or coronary artery disease were present, and liver disease whether hepatitis B or C were diagnosed. BMI analysis was performed using the World Health Organization criteria: <25 kg/m2 considered normal, ≥25–29.9 kg/m2 considered overweight, and ≥30 kg/m2 considered obesity.
All patients were under a steroid regimen, alongside other included medications: tacrolimus (n = 230, 81%), mycophenolate (n = 171, 60.2%), azathioprine (n = 69, 24.3%), cyclosporine (n = 34, 12%), mammalian target of rapamycin (mTOR) inhibitors (n = 33, 11.6%), and Belatacept (n = 1, 0.35%).
2.2. Laboratory Testing
On admission, we evaluated in-hospital laboratory data: serum creatinine, glycemia, alanine aminotransferase (ALT), aspartate aminotransferase (AST), lymphocytes, D-dimer, lactate dehydrogenase (LDH), and C-reactive protein (CRP). As for laboratory data before admission, we collected baseline creatinine (mean the last three measurements), fasting blood glucose (FBG, last measurement within 6 months), and glycated hemoglobin (HbA1c, last measurement within 1 year).
The estimated glomerular filtration rate (eGFR) was calculated using the formula defined in the CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) study.
2.3. Statistical Analyses
Two groups of renal recipients affected by COVID-19, e.g., overweight/obesity or BMI ≥ 25 kg/m2 and normal weight or BMI < 25 kg/m2 were separated. The primary aim was to investigate the differences in demographic and laboratory data, and COVID-19-related outcomes in both males and females who were overweight/obese compared to lean KTRs. The secondary aim was to investigate the risk factors associated with COVID-19-related outcomes, in particular, supplemental oxygen (O2) requirement in overweight/obese KTRs. Thus, we performed univariate analyses of demographic and laboratory data, and when the p-value was ≤0.1, the variables were entered simultaneously into a binary logistic regression model. The outcomes included death, transfer to intensive care unit (ICU), acute kidney injury (AKI) classified according to KDIGO (Kidney Disease Guidelines), need for hemodialysis (HD), supplemental O2, and invasive mechanical ventilation (IMV). Oxygen requirement was defined as any use of oxygen, including nasal prongs, masks, and non-invasive ventilation or high-flow, in particular when patients presented a SatO2 < 94% on room air and dyspnea. The results were expressed as odds ratios (ORs) with a confidence interval (CI) of 95%.
An independent samples t-test and chi-square test were used to identify the association between BMI and demographic and laboratory parameters, and the outcomes previously mentioned. Data were described as mean ± standard deviation or median and interquartile range, as indicated. Frequencies and percentages were reported for qualitative data.
Next, to determine which factors in both male and female KTRs who were overweight/obese increased the risk of the need for supplemental O2, demographic, and laboratory data were analyzed using the binary logistic regression model, as previously described.
Receiver Operating Characteristic (ROC) curves were used to identify the laboratory parameters associated with COVID-19-related outcomes. To calculate the LDH and eGFR cut-off values with better sensitivity and specificity for outcomes, we used the Youden index.
BMI was also evaluated as a continuous variable in a model of linear regression using demographic and laboratory data, as well as those outcomes, for both male and female KTRs.
We analyzed the data using IBM® SPSS (Statistical Product and Services Solutions, version 20.0, SPSS Inc, Chicago, IL, USA). A p-value of < 0.05 was considered significant for all data analyses.
3. Results
In our cohort, 60.6% (n = 97/160) of male KTRs were classified as overweight/obese, whereas 71% (n = 88/124) of female KTRs fell into the overweight/obese category (Table S1). Among overweight/obese males, a high prevalence of hypertension (86.6% vs. 73%, p = 0.03) and elevated FBG before admission (127.9 ± 65.5 vs. 106.4 ± 36.7 mg/dL, p = 0.02) were observed (Table 1). Additionally, overweight/obese males were less likely to developed lower grades of AKI less often (stage 1; 6.2% vs. 17.5%, p = 0.03). However, no significant differences in outcomes were observed between lean and overweight/obese male KTRs.

Table 1.
Clinical and epidemiological characteristics, laboratory data, and outcomes of male kidney transplant recipients who were overweight/obese and lean.
Remarkably, the overweight/obese female population exhibited a higher frequency of requiring supplemental O2 compared to their lean counterparts (63.6% vs. 41.7%, odds ratio [OR] = 2.45, p = 0.03) (Table 2).
Table 2.
Clinical and epidemiological characteristics, laboratory data, and outcomes of female kidney transplant recipients who were overweight and lean.
Within the overweight/obese female group, several factors including age (54.6 ± 11.7 vs. 49.5 ± 9.8 years, p = 0.04), smoking (32.1% vs. 9.4%, p = 0.03), basal eGFR (44.3 ± 21.4 vs. 56.4 ± 25.9 mL/min/1.73m2, p = 0.03), on-admission eGFR (32.3 ± 21.3 vs. 45.6 ± 20.1 mL/min/1.73m2, p = 0.01), and LDH levels (367.3 ± 227.4 vs. 237.5 ± 88.0 U/L, p = 0.006) were associated with an increased risk of requiring supplemental O2 (Table 3). Multivariate analysis identified age (p = 0.02) as an independent risk factor for the need for O2 supplementation in this population (Table 3). When we analyzed the outcomes of overweight/obese female KTRs who required O2, we observed that these patients exhibited elevated rates of mortality, transfer to ICU, IMV, and AKI necessitating HD (Table 3).
Table 3.
Risk factors for the use of supplemental oxygen (O2) and outcomes in female kidney transplant recipients who were overweight/obese.
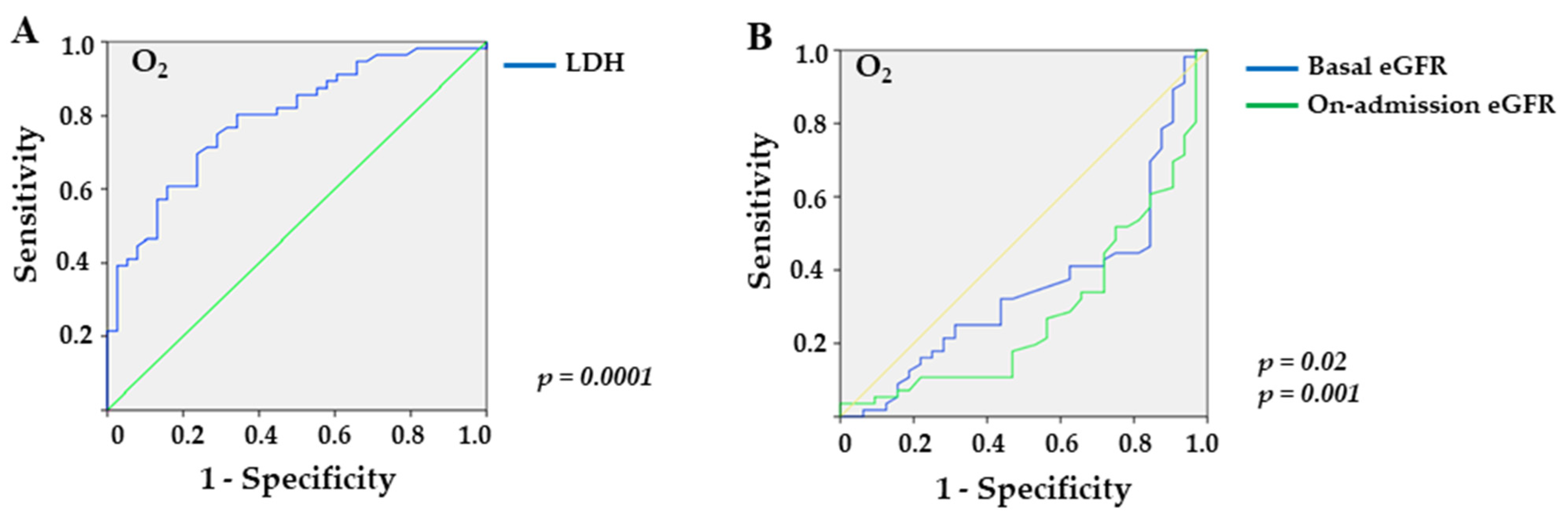
Furthermore, the ROC curve for LDH revealed an AUC of 0.792 (p < 0.0001) with a sensitivity of 70.5% and a specificity of 66.7% for values greater than 237.0 U/L in overweight/obese females requiring O2 supplementation (Figure 1A). Additionally, baseline and on-admission eGFR yielded AUCs of 0.354 (p = 0.02) and 0.285 (p = 0.001) with sensitivities of 46.4% and 34% and specificities of 84.4% and 71.9% for eGFR values lower than 38 mL/min/1.73 m2 and 38 mL/min/1.73 m2, respectively (Figure 1B).
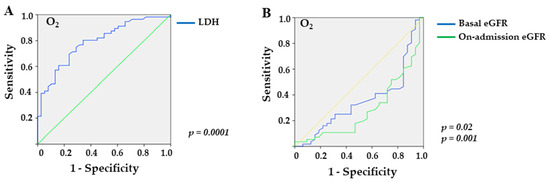
Figure 1.
Sensitivity and specificity of laboratory markers in female overweight/obese KTRs with COVID-19 who required supplemental O2: (A) LDH (lactate dehydrogenase; p = 0.0001), and (B) basal eGFR (estimated glomerular filtration rate; p = 0.02) and on-admission eGFR (p = 0.001).
To further support our findings, we conducted a linear regression model using BMI as a continuous and dependent variable (Tables S2 and S3). Notably, in the analysis of female KTRs, BMI remained a significant risk factor for O2 requirement (OR = 2.51, p = 0.004; Table S3).
4. Discussion
In our study, we observed distinct patterns of COVID-19 outcomes between male and female KTRs. Among male KTRs who were overweight/obese, we found a higher prevalence of hypertension and poorer glycemic control. Additionally, they were more likely to develop a more severe stage of AKI. However, we did not observe differences in other COVID-19-related outcomes compared to lean male KTRs. Surprisingly, among overweight/obese female KTRs, we observed a higher frequency of requiring supplemental O2. Age, smoking, lower renal function, and higher LDH levels were associated with an increased risk of needing O2 in this group. Among overweight/obese women requiring O2, elevated rates of mortality, ICU transfers, employment of IMV, and AKI necessitating HD were observed. These findings suggest that overweight/obesity and its associated comorbidities may have a different impact on the kidney transplant setting.
Obesity, when combined with other underlying cardiometabolic risk factors, such as hypertension, DM, and lipid disorders, can worsen clinical outcomes in the context of COVID-19 [13]. The number of metabolic syndrome components, particularly central obesity, has been associated with increased COVID-19 severity [14]. Obesity itself has been identified as an independent risk factor for SARS-CoV-2 infection (OR = 1.47–2.73), hospitalization (OR = 1.72–2.13), severe disease (OR = 3.81), the need for ICU admission (OR = 1.74–2.25), IMV (OR = 1.66), and mortality (OR = 1.48–1.61) [15,16]. Importantly, a temporal relationship between respiratory failure and kidney injury has been demonstrated in individuals with COVID-19 [17], as exemplified by our cohort of overweight/obese female KTRs requiring O2. This correlation is underpinned by analogous pathophysiologic mechanisms within kidney and lung tissues, incorporating direct damage by SARS-CoV-2, localized inflammation, endothelial dysfunction, and the development of microthrombi [18]. As a result, these patients exhibit a more unfavorable outcome [19].
However, it should be noted that the association between obesity and worse COVID-19 outcomes is often influenced by the presence of hypertension and DM [20].
Obesity is associated with COVID-19 severity through several mechanisms. Firstly, adipose tissue expresses the ACE2, a receptor used by SARS-CoV-2 for cell entry [21]. This suggests that this tissue may serve as a reservoir for viral replication, leading to increased COVID-19 burden. Additionally, ACE2 gene expression is higher in subcutaneous and visceral adipose tissues compared to lung cells in obese patients [22,23], along with elevated levels of soluble ACE2 (sACE2) in patients with metabolic syndrome [24]. Notably, chronic glucocorticoid use in KTRs may also contribute to obesity [25].
Secondly, the inflammatory imbalance in obesity affects the production of adipokines. Proinflammatory adipokines such as leptin are upregulated, while anti-inflammatory adipokines such as adiponectin are downregulated in severe COVID-19 [26]. This abnormality exacerbates cerebrovascular and cardiovascular diseases, insulin resistance, and increases susceptibility to viral lung infections [27]. These factors can ultimately contribute to the need for supplemental O2.
SARS-CoV-2 can also dysregulate the immune system, leading to endothelial cell damage associated with thrombosis and inflammation (thromboinflammation) [28] and imbalances in the renin–angiotensin–aldosterone and kallikrein–kinin systems [21]. Ectopic fat accumulation, including epicardial and visceral adipose tissue, contributes to the release of chemokines, cytokines, and adipokines, further driving COVID-19 severity in obese patients [29].
Thirdly, obesity-related comorbidities such as heart, kidney, and pancreatic diseases can contribute to dysregulation of the ACE/ACE2 axis in tissue associated with these diseases [21]. Increased ACE2 expression has been observed in overweight patients with COPD [30]. Smoking, which upregulates ACE2 expression in the lungs [31], can also contribute to the need for supplemental O2 in overweight/obese KTRs who smoke.
Lastly, higher grades of obesity are associated with lower levels of the PaO2/FIO2 ratio, indicating a ventilation capacity failure due to mechanical impairment and the burden of COVID-19 [32]. Obese patients experience pulmonary pathophysiological changes, including increased atelectasis formation due to the negative effects of thoracic wall weight and abdominal fat mass [33]. They also exhibit increased work of breathing and abnormalities in blood gas exchange [34].
In our study, despite overweight/obese male KTRs exhibiting a higher prevalence of hypertension and elevated glycaemia before admission, they did not experience worse COVID-19-related outcomes compared to lean male KTRs. It is important to highlight that hypertension has been identified as an independent risk factor for COVID-19 progression and mortality [2,35], as well as glycemic levels [3,36] in KTRs and the general population. Nevertheless, the case-fatality rate among KTRs remains higher than that of the general population [37], as we observed in our study (approximately 25%). Additionally, the prevalence of obesity-related comorbidities such as hypertension, DM, and heart disease was similar between overweight/obese male KTRs and their counterparties in our population (86.6% vs. 73%, 40.2% vs. 33.3%, and 13.4% vs. 11.1%, respectively). A similar pattern was observed in overweight/obese female KTRs compared to lean individuals in terms of hypertension (69.3% vs. 63.9%), DM (42% vs. 41.7%), and heart disease (12.5% vs. 2.8%). These findings indicate that obesity and its related comorbidities may have a different impact within the kidney transplant population, which may be explained by the dysregulation of the ACE1/ACE2 axis [21,38].
It is worth noting that a majority of our KTR population was overweight/obese, and this finding was consistent among males and females. However, despite this consistency, no discernible differences in mortality rates were observed between lean and overweight/obese male and female KTR individuals.
Sex differences in non-transplant individuals regarding BMI indicate that females with COVID-19 require hospitalization more frequently, while males have worse outcomes such as ICU transfer, the need for IMV, and higher mortality rates, which can be partly explained by higher rates of hypertension and DM, as mentioned earlier [20]. Moreover, age seems to have a more pronounced effect on COVID-19 outcomes in males, whereas obesity has a stronger bearing on outcomes in females [39,40].
Several studies have investigated the impact of sex and age on the levels of ACE2. The higher expression of ACE2 in men and its location on the X chromosome may explain why SARS-CoV-2 binds more frequently to ACE2 in men [38]. In females, ACE2 on either X chromosome can recognize the virus, but the chance of both ACE2 copies binding perfectly to the virus is low, allowing unbound ACE2 to cleave angiotensin II and decrease COVID-19-related complications [41]. Other genes involved in the immune response, located on the X chromosome, may contribute to a more robust immune response in females [42].
Additionally, females mount a stronger adaptive immune response, while males exhibit a more robust innate immune response [43]. In COVID-19 patients, immune profiling has unveiled dynamic alterations in both innate and adaptive immune cells, with specific natural killer-cell receptors and IgM+ B cells linked to significant CD4 and CD8 T-cell exhaustion, thereby elevating the risk of intubation and mortality [44]. These immune dynamics can elucidate the variations in COVID-19 progression between males, with potential implications for clinical outcomes.
Likewise, estrogens and their receptors play a crucial role in regulating innate immune responses to viral infections by regulating the type-I interferon (IFN) response through several mechanisms, including inhibiting the production of type-I IFNs, and suppressing IFN signaling [12,41]. They can also modulate the production of proinflammatory cytokines by blocking NF-κB signaling [12,41]. In addition to regulating immune responses, estrogens and their receptors also have an impact on the severity of viral infections. These hormones have been shown to mitigate this inflammatory response by reducing the overexpression of proinflammatory cytokines, leading to more balanced immune responses that can effectively clear the virus without causing excessive damage to the host [45]. Estrogen may also regulate the ACE1/ACE2 axis and leads to anti-inflammatory and anti-oxidative effects [12,46].
However, the protective effect of the female sex on COVID-19 outcomes, attributed to genetic factors (ACE2 gene location in the X chromosome), immunologic privilege, and hormonal benefits (estrogen) [12], may be compromised by obesity, as we observed in our study. Previous studies have shown higher levels of ACE2 expression in adipose tissue in females compared to males [23], and increased levels of plasma sACE2, released from cytoplasmic membrane to plasma when tissues are damaged [21], were more pronounced in postmenopausal women compared to premenopausal women [24]. Consequently, the beneficial effect of estrogen may be diminished during the postmenopausal period. Although we did not assess the menopausal status in our population, which is likely high given the mean age of 52 years.
Moreover, in a pre-clinical model of diet-induced obesity in K18-hACE2 transgenic mice, obese female animals demonstrated a shorter time to morbidity, indicating increased susceptibility to SARS-CoV-2, while the obese male mice did not exhibit the same trend. Furthermore, this increased susceptibility in obese female animals was linked to higher viral RNA load and interferon production [47]. Additionally, in non-transplanted individuals, it was discovered that a higher BMI posed a greater risk of COVID-19 mortality in females when compared to males [40]. These observations emphasize the importance of considering gender disparities and the potential impact of obesity on COVID-19 outcomes.
Overall, understanding the influence of sex and age on ACE2 expression and immune responses is crucial for elucidating the differences in COVID-19 outcomes and developing tailored therapies. Moreover, the identification of individuals at high risk of COVID-19-related complications is of paramount importance for effective healthcare management. Emerging data indicate factors such as female sex, pulmonary disease, DM, obesity, and organ transplants as potential risk factor for long COVID-19 [48,49]. It is worth noting that obesity rates have been on the rise in Brazil, particularly among women [50,51]. Therefore, our findings underscore the importance of policymakers, stakeholders, and patients themselves in implementing non-pharmacological, such as lifestyle modifications, and pharmacological approaches to address obesity and related risk factors effectively.
In our study, it is important to highlight that all data were retrospectively collected, and the sample size was limited. Importantly, the attributes of our population, particularly the heightened occurrence of overweight/obesity among KTR women, in conjunction with the limitations imposed by the confined geographical area, could potentially restrict the generalizability of our findings. Additionally, we did not assess the impact of the immunosuppressive regimen on COVID-19 outcomes, a pivotal aspect for consideration. This is particularly relevant as it could be associated with elevated trough levels, possibly stemming from factors such as vomiting, diarrhea, and hepatic injury [52]. Moreover, the impact of longitudinal analyses of laboratory parameters and the vaccination on COVID-19 outcomes in KTRs who are overweight/obese should be further investigated.
In conclusion, our findings highlight the importance of considering gender disparities and the potential impact of obesity on COVID-19 outcomes in the kidney transplant setting.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/medicina59091555/s1. Table S1: Clinical and epidemiological characteristics, laboratory data, and outcomes of male and female kidney transplant recipients. Table S2: Clinical and epidemiological characteristics, laboratory data, and outcomes of male kidney transplant recipients (n = 160) using BMI as a continuous variable. Table S3: Clinical and epidemiological characteristics, laboratory data, and outcomes of female kidney transplant recipients (n = 124) using BMI as a continuous variable.
Author Contributions
Conceptualization, A.V.-A. and É.B.R.; methodology, A.V.-A., D.D.d.L., I.A.-B. and É.B.R.; validation, H.T.-S., J.O.M.-P. and É.B.R.; formal analysis, A.V.-A., D.D.d.L. and I.A.-B.; investigation, A.V.-A. and É.B.R.; data curation, A.V.-A., D.D.d.L., I.A.-B. and M.P.C.; writing—original draft preparation, A.V.-A., D.D.d.L. and É.B.R.; writing—review and editing, A.V.-A. and É.B.R.; visualization, A.V.-A. and É.B.R.; supervision, É.B.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics and Research Committee of the Federal University of São Paulo, São Paulo, Brazil (number CAEE35311020.9.0000.8098, date of approval 30 March 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study, whereas a waiver was granted for patients who died in other hospitals.
Data Availability Statement
The data presented in this study are available on request from the corresponding authors. The data are not publicly available due to clinical patient information.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Demir, E.; Ucar, Z.A.; Dheir, H.; Danis, R.; Yelken, B.; Uyar, M.; Parmaksiz, E.; Artan, A.S.; Sinangil, A.; Merhametsiz, O.; et al. COVID-19 in Kidney Transplant Recipients: A Multicenter Experience from the First Two Waves of Pandemic. BMC Nephrol. 2022, 23, 183. [Google Scholar] [CrossRef] [PubMed]
- Aguiar-Brito, I.; de Lucena, D.D.; Veronese-Araújo, A.; Cristelli, M.P.; Tedesco-Silva, H.; Medina-Pestana, J.O.; Rangel, É.B. Impact of Hypertension on COVID-19 Burden in Kidney Transplant Recipients: An Observational Cohort Study. Viruses 2022, 14, 2409. [Google Scholar] [CrossRef] [PubMed]
- Rangel, É.B.; de Lucena, D.D.; Aguiar-Brito, I.; de Andrade, L.G.M.; Veronese-Araújo, A.; Cristelli, M.P.; Tedesco-Silva, H.; Medina-Pestana, J.O. COVID-19 in Kidney Transplant Recipients with Diabetes Mellitus: A Pro-pensity Score Matching Analysis. Transpl. Int. 2022, 35, 10375. [Google Scholar] [CrossRef]
- Veronese-Araújo, A.; de Lucena, D.D.; Aguiar-Brito, I.; Modelli de Andrade, L.G.; Cristelli, M.P.; Tedesco-Silva, H.; Medina-Pestana, J.O.; Rangel, É.B. Oxygen Requirement in Overweight/Obese Kidney Transplant Recipients with COVID-19: An Observational Cohort Study. Diagnostics 2023, 13, 2168. [Google Scholar] [CrossRef] [PubMed]
- Aghili, S.M.M.; Ebrahimpur, M.; Arjmand, B.; Shadman, Z.; Sani, M.P.; Qorbani, M.; Larijani, B.; Payab, M. Obesity in COVID-19 era, implications for mechanisms, comorbidities, and prognosis: A review and meta-analysis. Int. J. Obes. 2021, 45, 998–1016. [Google Scholar] [CrossRef]
- Moriconi, D.; Masi, S.; Rebelos, E.; Virdis, A.; Manca, M.L.; De Marco, S.; Taddei, S.; Nannipieri, M. Obesity prolongs the hospital stay in patients affected by COVID-19, and may impact on SARS-COV-2 shedding. Obes. Res. Clin. Pract. 2020, 14, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Kivimäki, M.; Kuosma, E.; Ferrie, J.E.; Luukkonen, R.; Nyberg, S.T.; Alfredsson, L.; Batty, G.D.; Brunner, E.J.; Fransson, E.; Goldberg, M.; et al. Overweight, obesity, and risk of cardiometabolic multimorbidity: Pooled analysis of individual-level data for 120 813 adults from 16 cohort studies from the USA and Europe. Lancet Public Health 2017, 2, e277–e285. [Google Scholar] [CrossRef]
- Fuster, J.J.; Ouchi, N.; Gokce, N.; Walsh, K. Obesity-Induced Changes in Adipose Tissue Microenvironment and Their Impact on Cardiovascular Disease. Circ. Res. 2016, 118, 1786–1807. [Google Scholar] [CrossRef]
- Iwamoto, S.J.; Abushamat, L.A.; Zaman, A.; Millard, A.J.; Cornier, M.-A. Obesity Management in Cardiometabolic Disease: State of the Art. Curr. Atheroscler. Rep. 2021, 23, 59. [Google Scholar] [CrossRef]
- Nguyen, N.T.; Chinn, J.; De Ferrante, M.; Kirby, K.A.; Hohmann, S.F.; Amin, A. Male gender is a predictor of higher mortality in hospitalized adults with COVID-19. PLoS ONE 2021, 16, e0254066. [Google Scholar] [CrossRef]
- Ten-Caten, F.; Gonzalez-Dias, P.; Castro, Í.; Ogava, R.L.; Giddaluru, J.; Silva, J.C.S.; Martins, F.; Gonçalves, A.N.; Costa-Martins, A.G.; Araujo, J.D.; et al. In-depth analysis of laboratory parameters reveals the interplay between sex, age, and systemic inflammation in individuals with COVID-19. Int. J. Infect. Dis. 2021, 105, 579–587. [Google Scholar] [CrossRef]
- Kumar, A.; Narayan, R.K.; Kulandhasamy, M.; Prasoon, P.; Kumari, C.; Kumar, S.; Pareek, V.; Sesham, K.; Shekhawat, P.S.; Kant, K.; et al. COVID-19 pandemic: Insights into molecular mechanisms leading to sex-based differences in patient outcomes. Expert Rev. Mol. Med. 2021, 23, e7. [Google Scholar] [CrossRef] [PubMed]
- Kompaniyets, L.; Pennington, A.F.; Goodman, A.B.; Rosenblum, H.G.; Belay, B.; Ko, J.Y.; Chevinsky, J.R.; Schieber, L.Z.; Summers, A.D.; Lavery, A.M.; et al. Underlying Medical Conditions and Severe Illness among 540,667 Adults Hospitalized with COVID-19, March 2020–March 2021. Prev. Chronic Dis. 2021, 18, E66. [Google Scholar] [CrossRef] [PubMed]
- Cho, D.-H.; Choi, J.; Gwon, J.G. Metabolic syndrome and the risk of COVID-19 infection: A nationwide population-based case-control study. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2596–2604. [Google Scholar] [CrossRef]
- Cai, Z.; Yang, Y.; Zhang, J. Obesity is associated with severe disease and mortality in patients with coronavirus disease 2019 (COVID-19): A meta-analysis. BMC Public Health 2021, 21, 1505. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Du, S.; Green, W.D.; Beck, M.A.; Algaith, T.; Herbst, C.H.; Alsukait, R.F.; Alluhidan, M.; Alazemi, N.; Shekar, M. Faculty Opinions recommendation of Individuals with obesity and COVID-19: A global perspective on the epidemiology and biological relationships. Obes. Rev. 2020, 21, e13128. [Google Scholar] [CrossRef]
- Hirsch, J.S.; Ng, J.H.; Ross, D.W.; Sharma, P.; Shah, H.H.; Barnett, R.L.; Hazzan, A.D.; Fishbane, S.; Jhaveri, K.D.; on behalf of the Northwell COVID-19 Research Consortium and the Northwell Nephrology COVID-19 Research Consortium. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int. 2020, 98, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Legrand, M.; Bell, S.; Forni, L.; Joannidis, M.; Koyner, J.L.; Liu, K.; Cantaluppi, V. Pathophysiology of COVID-19-associated acute kidney injury. Nat. Rev. Nephrol. 2021, 17, 751–764. [Google Scholar] [CrossRef]
- Robbins-Juarez, S.Y.; Qian, L.; King, K.L.; Stevens, J.S.; Husain, S.A.; Radhakrishnan, J.; Mohan, S. Outcomes for Patients with COVID-19 and Acute Kidney Injury: A Systematic Review and Meta-Analysis. Kidney Int. Rep. 2020, 5, 1149–1160. [Google Scholar] [CrossRef]
- Tong, L.; Khani, M.; Lu, Q.; Taylor, B.; Osinski, K.; Luo, J. Association between body-mass index, patient characteristics, and obesity-related comorbidities among COVID-19 patients: A prospective cohort study. Obes. Res. Clin. Pract. 2022, 17, 47–57. [Google Scholar] [CrossRef]
- Beyerstedt, S.; Casaro, E.B.; Rangel, E.B. COVID-19: Angiotensin-converting enzyme 2 (ACE2) expression and tissue susceptibility to SARS-CoV-2 infection. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 905–919. [Google Scholar] [CrossRef] [PubMed]
- Al-Benna, S. Association of high level gene expression of ACE2 in adipose tissue with mortality of COVID-19 infection in obese patients. Obes. Med. 2020, 19, 100283. [Google Scholar] [CrossRef]
- Li, Y.; Xu, Q.; Ma, L.; Wu, D.; Gao, J.; Chen, G.; Li, H. Systematic profiling of ACE2 expression in diverse physiological and pathological conditions for COVID-19/SARS-CoV-2. J. Cell. Mol. Med. 2020, 24, 9478–9482. [Google Scholar] [CrossRef] [PubMed]
- Kornilov, S.A.; Lucas, I.; Jade, K.; Dai, C.L.; Lovejoy, J.C.; Magis, A.T. Plasma levels of soluble ACE2are associated with sex, Metabolic Syndrome, and its biomarkers in a large cohort, pointing to a possible mechanism for increased severity in COVID-19. Crit. Care 2020, 24, 452. [Google Scholar] [CrossRef] [PubMed]
- De Lucena, D.D.; Rangel, É.B. Glucocorticoids use in kidney transplant setting. Expert Opin. Drug Metab. Toxicol. 2018, 14, 1023–1041. [Google Scholar] [CrossRef]
- Perrotta, F.; Scialò, F.; Mallardo, M.; Signoriello, G.; D’Agnano, V.; Bianco, A.; Daniele, A.; Nigro, E. Adiponectin, Leptin, and Resistin Are Dysregulated in Patients Infected by SARS-CoV-2. Int. J. Mol. Sci. 2023, 24, 1131. [Google Scholar] [CrossRef]
- Salvator, H.; Grassin-Delyle, S.; Naline, E.; Brollo, M.; Fournier, C.; Couderc, L.-J.; Devillier, P. Contrasting Effects of Adipokines on the Cytokine Production by Primary Human Bronchial Epithelial Cells: Inhibitory Effects of Adiponectin. Front. Pharmacol. 2020, 11, 56. [Google Scholar] [CrossRef]
- Wagner, D.D.; Heger, L.A. Thromboinflammation: From Atherosclerosis to COVID-19. Arter. Thromb. Vasc. Biol. 2022, 42, 1103–1112. [Google Scholar] [CrossRef]
- Lasbleiz, A.; Gaborit, B.; Soghomonian, A.; Bartoli, A.; Ancel, P.; Jacquier, A.; Dutour, A. COVID-19 and Obesity: Role of Ectopic Visceral and Epicardial Adipose Tissues in Myocardial Injury. Front. Endocrinol. 2021, 12, 726967. [Google Scholar] [CrossRef]
- Higham, A.; Singh, D. Increased ACE2 Expression in Bronchial Epithelium of COPD Patients who are Overweight. Obesity 2020, 28, 1586–1589. [Google Scholar] [CrossRef]
- Leung, J.M.; Yang, C.X.; Tam, A.; Shaipanich, T.; Hackett, T.-L.; Singhera, G.K.; Dorscheid, D.R.; Sin, D.D. ACE-2 expression in the small airway epithelia of smokers and COPD patients: Implications for COVID-19. Eur. Respir. J. 2020, 55, 2000688. [Google Scholar] [CrossRef]
- Dana, R.; Bannay, A.; Bourst, P.; Ziegler, C.; Losser, M.-R.; Gibot, S.; Levy, B.; Audibert, G.; Ziegler, O. Obesity and mortality in critically ill COVID-19 patients with respiratory failure. Int. J. Obes. 2021, 45, 2028–2037. [Google Scholar] [CrossRef] [PubMed]
- De Jong, A.; Chanques, G.; Jaber, S. Mechanical ventilation in obese ICU patients: From intubation to extubation. Crit. Care 2017, 21, 63. [Google Scholar] [CrossRef] [PubMed]
- Kress, J.P.; Pohlman, A.S.; Alverdy, J.; Hall, J.B. The impact of morbid obesity on oxygen cost of breathing (VO(2RESP)) at rest. Am. J. Respir. Crit. Care Med. 1999, 160, 883–886. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Liu, Y.; Qin, J.; Ruan, C.; Zeng, X.; Xu, A.; Yang, R.; Li, J.; Cai, H.; Zhang, Z. Hypertension as an independent risk factor for severity and mortality in patients with COVID-19: A retrospective study. Postgrad. Med. J. 2021, 98, 515–522. [Google Scholar] [CrossRef]
- Wong, R.; Hall, M.; Vaddavalli, R.; Anand, A.; Arora, N.; Bramante, C.T.; Garcia, V.; Johnson, S.; Saltz, M.; Tronieri, J.S.; et al. Glycemic Control and Clinical Outcomes in U.S. Patients With COVID-19: Data from the National COVID Cohort Collaborative (N3C) Database. Diabetes Care 2022, 45, 1099–1106. [Google Scholar] [CrossRef]
- Weiss, A.M.; Hendrickx, R.; Stensgaard, E.M.; Jellingsø, M.M.; Sommer, M.O. Kidney Transplant and Dialysis Patients Remain at Increased Risk for Succumbing to COVID-19. Transplantation 2023, 107, 1136–1138. [Google Scholar] [CrossRef]
- Gemmati, D.; Bramanti, B.; Serino, M.L.; Secchiero, P.; Zauli, G.; Tisato, V. COVID-19 and Individual Genetic Susceptibility/Receptivity: Role of ACE1/ACE2 Genes, Immunity, Inflammation and Coagulation. Might the Double X-Chromosome in Females Be Protective against SARS-CoV-2 Compared to the Single X-Chromosome in Males? Int. J. Mol. Sci. 2020, 21, 3474. [Google Scholar] [CrossRef] [PubMed]
- Mufarrih, S.H.; Qureshi, N.Q.; Yunus, R.; Ngo, D.; Katz, D.; Krakower, D.; Bhambhani, V.; Quadir, J.; Solleveld, P.; Banner-Goodspeed, V.; et al. Influence of Increasing Age and Body Mass Index of Gender in COVID-19 Patients. J. Women’s Health 2022, 31, 779–786. [Google Scholar] [CrossRef]
- Peters, S.A.E.; MacMahon, S.; Woodward, M. Obesity as a risk factor for COVID-19 mortality in women and men in the UK biobank: Comparisons with influenza/pneumonia and coronary heart disease. Diabetes Obes. Metab. 2021, 23, 258–262. [Google Scholar] [CrossRef]
- Li, Y.; Jerkic, M.; Slutsky, A.S.; Zhang, H. Molecular mechanisms of sex bias differences in COVID-19 mortality. Crit. Care 2020, 24, 405. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.S.A.; Moritz, M.J.; Saaed, M.I.; Heifets, M.; Sustento-Reodica, N.; Fyfe, B.; Kumar, A. Avoidance of Chronic Steroid Therapy in African American Kidney Transplant Recipients Monitored by Surveillance Biopsy: 1-Year Results. Am. J. Transplant. 2005, 5, 1976–1985. [Google Scholar] [CrossRef] [PubMed]
- Qi, S.; Ngwa, C.; Scheihing, D.A.M.; Al Mamun, A.; Ahnstedt, H.W.; Finger, C.E.; Colpo, G.D.; Sharmeen, R.; Kim, Y.; Choi, H.A.; et al. Sex differences in the immune response to acute COVID-19 respiratory tract infection. Biol. Sex Differ. 2021, 12, 66. [Google Scholar] [CrossRef] [PubMed]
- Rendeiro, A.F.; Casano, J.; Vorkas, C.K.; Singh, H.; Morales, A.; A DeSimone, R.; Ellsworth, G.B.; Soave, R.; Kapadia, S.N.; Saito, K.; et al. Profiling of immune dysfunction in COVID-19 patients allows early prediction of disease progression. Life Sci. Alliance 2020, 4, e202000955. [Google Scholar] [CrossRef]
- Harding, A.T.; Heaton, N.S. The Impact of Estrogens and Their Receptors on Immunity and Inflammation during Infection. Cancers 2022, 14, 909. [Google Scholar] [CrossRef] [PubMed]
- Bukowska, A.; Spiller, L.; Wolke, C.; Lendeckel, U.; Weinert, S.; Hoffmann, J.; Bornfleth, P.; Kutschka, I.; Gardemann, A.; Isermann, B.; et al. Protective regulation of the ACE2/ACE gene expression by estrogen in human atrial tissue from elderly men. Exp. Biol. Med. 2017, 242, 1412–1423. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.S.; Russ, B.P.; Wong, T.Y.; Horspool, A.M.; Winters, M.T.; Barbier, M.; Bevere, J.R.; Martinez, I.; Damron, F.H.; Cyphert, H.A. Obesity and metabolic dysfunction drive sex-associated differential disease profiles in hACE2-mice challenged with SARS-CoV-2. iScience 2022, 25, 105038. [Google Scholar] [CrossRef]
- Notarte, K.I.; de Oliveira, M.H.S.; Peligro, P.J.; Velasco, J.V.; Macaranas, I.; Ver, A.T.; Pangilinan, F.C.; Pastrana, A.; Goldrich, N.; Kavteladze, D.; et al. Age, Sex and Previous Comorbidities as Risk Factors Not Associated with SARS-CoV-2 Infection for Long COVID-19: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 7314. [Google Scholar] [CrossRef]
- Daitch, V.; Yelin, D.; Awwad, M.; Guaraldi, G.; Milić, J.; Mussini, C.; Falcone, M.; Tiseo, G.; Carrozzi, L.; Pistelli, F.; et al. Characteristics of long-COVID among older adults: A cross-sectional study. Int. J. Infect. Dis. 2022, 125, 287–293. [Google Scholar] [CrossRef]
- Moura, E.C.; Claro, R.M. Estimates of obesity trends in Brazil, 2006–2009. Int. J. Public Health 2011, 57, 127–133. [Google Scholar] [CrossRef]
- Xavier, P.B.; Garcez, A.; Silva, J.C.D.; Cibeira, G.H.; Germano, A.; Olinto, M.T.A. Obesity among Industrial Workers in Brazil: A Cross-Sectional Study on Prevalence and Associated Factors. J. Occup. Environ. Med. 2022, 64, e231–e236. [Google Scholar] [CrossRef] [PubMed]
- McMinn, J.; Black, H.; Harrison, L.L.; Geddes, C. SARS-CoV-2 and Tacrolimus Blood Concentration in Kidney Transplant Recip-ients. Kidney Int. Rep. 2021, 6, 2694–2697. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).