Abstract
Background and Objective: About 14 million people will likely suffer a traumatic brain injury (TBI) per year by 2050 in sub-Saharan Africa. Studying TBI characteristics and their relation to outcomes can identify initiatives to improve TBI prevention and care. The objective of this study was to define the features and outcomes of TBI patients seen over a 1-year period in a level-I trauma centre in Cameroon. Materials and Methods: Data on demographics, causes, clinical aspects, and discharge status were collected over a period of 12 months. The Glasgow Outcome Scale-Extended (GOSE) and the Quality-of-Life Questionnaire after Brain Injury (QoLIBRI) were used to evaluate outcomes six months after TBI. Comparisons between two categorical variables were done using Pearson’s chi-square test. Results: A total of 160 TBI patients participated in the study. The age group 15–45 years was most represented (78%). Males were more affected (90%). A low educational level was seen in 122 (76%) cases. Road traffic incidents (RTI) (85%), assaults (7.5%), and falls (2.5%) were the main causes of TBI, with professional bike riders being frequently involved (27%). Only 15 patients were transported to the hospital by ambulance, and 14 of these were from a referring hospital. CT-imaging was performed in 78% of cases, and intracranial traumatic abnormalities were identified in 64% of cases. Financial constraints (93%) was the main reason for not performing a CT scan. Forty-six (33%) patients were discharged against medical advice (DAMA) due to financial constraints. Mortality was 14% (22/160) and high in patients with severe TBI (46%). DAMA had poor outcomes with QoLIBRI. Only four patients received post-injury physical therapy services. Conclusions: TBI in Cameroon mainly results from RTIs and commonly affects young adult males. Lack of pre-hospital care, financial constraints limiting both CT scanning and medical care, and a lack of acute physiotherapy services likely influenced care and outcomes adversely.
1. Introduction
Traumatic brain injury (TBI) is considered a global public health challenge, affecting about 69 million individuals annually and is the leading cause of death and disability globally [1,2]. In sub-Saharan Africa (SSA), an estimated 3.2 million people sustain TBI annually, and this number is expected to rise to 14 million by 2050 [3]. Road traffic incidents (RTIs), falls, and assaults are the most common causes of TBI [4,5], with RTIs being the predominant cause in SSA [1,6].
The global TBI burden is increasing, and to a greater extent in SSA, as shown by its fast-rising incidence [7]. In the U.S., about 90,000 people have long-term disabilities due to a TBI [8], but such data are not available from many countries due to limited research. Djientcheu et al. [9] reported TBI outcomes in SSA, with a mortality rate of 77% in severe injuries, 16% in moderate injuries, and 1% in mild cases (again, RTIs were the most common cause). In addition to mortality and morbidity, TBI adversely influences the lives of those affected and their families, often leading to a decreased life expectancy compared with the general population. These injuries often affect lower-income families, and surviving patients incur substantial direct and indirect costs [10,11]. Furthermore, the heterogeneous nature of traumatic brain injuries complicates the accurate assessment of severity and prediction of clinical outcomes [12,13].
Despite the social and economic impact of TBI in Cameroon, data on its characteristics and medium- or long-term outcomes are lacking; only a few studies from SSA report traumatic brain injuries as a major cause of death and disability. Ndoumbe et al. [14] and Motah et al. [15] addressed TBI management and outcomes, but only severe TBI or intracranial haemorrhage were considered, and cases of medium- or long-term outcomes were not included. Furthermore, the study of Ndoumbe et al. [14] was retrospective in design; hence, outcome evaluations were not appropriate for patient characteristics and medium-term outcomes after TBI [16].
Our study seeks to provide patient characteristics and medium-term outcomes with the Glasgow Outcome Scale Extended (GOSE) and Quality of Life after TBI questionnaire (QoLIBRI) from a Level I trauma centre. The study was conducted in Douala, Cameroon to evaluate how TBI patient’s features interact with the outcomes in a LMIC setting.
2. Materials and Methods
2.1. Study Design
We conducted a prospective cohort study on TBI patients attending a Level I trauma centre at the Laquintinie Hospital in Douala (LHD), Cameroon, from January 2021 to February 2022. Douala is situated on the Atlantic Ocean and is the economic capital of the country, with an estimated population of 4 million [17]. The Laquintinie Hospital manages all types of trauma and is among the few hospitals with technical expertise for TBI care. It has a fully functional neurosurgical unit with four neurosurgeons, a CT scanner, and a 0.5 Tesla MRI.
2.2. Study Population
Our study included all patients with TBI received at the LHD within 24 h who were able to consent (on some occasions, from family members). TBI patients with pre-existing neuropsychiatric problems and thieves were excluded, along with those with delayed presentation to LHD (arrived > 24 h after injury, n = 18). We also excluded patients who could not be contacted for the 6-month evaluation (n = 8).
2.3. Data Collection
After a definitive diagnosis of TBI, the study purpose was meticulously explained to the patients or their proxies, and consent was obtained to participate in the study. Data collection was based on the NIH-NINDS common data elements and included information such as sociodemographic characteristics (age, sex, profession, marital status, religion, and nationality, monthly income), clinical details (heart rate, blood pressure, temperature, Glasgow Coma Scale (GCS), and neuro-imaging findings), and pre-hospital factors (transport means, time between injury and arrival). Hypothermia was defined as <35 °C, normal between 35 °C and 37.9 °C, and fever if the temperature was >38 °C (CDC, 2019). Hypotension was noted as blood pressure below 90/60 mmHg; values of 130–139/80–89 mmHg were considered stage one hypertension; systolic values > 140 mmHg and/or diastolic values > 90 mmHg were considered stage 2 hypertension [18]. TBI severity was classified according to the GCS: 3–8 for severe, 9–12 for moderate, and 13–15 for mild. We included data on aetiology, injury mechanism, presenting symptoms, hospital length of stay, and outcomes. The GOSE and QoLIBRI were recorded 6 months after hospital discharge by telephone communication with patients and their families (good recovery, mental or physical disability, vegetative state, death). Data collection and reporting were in accordance with the STROBE guidelines (Table S4).
2.4. Outcome Measures
Discharge status was scored using the Disability Rating Scale (DRS) with a total score of 29 (level of disability: 0 none, 1 mild, 2–3 partial, 4–6 moderate, 7–11 moderately severe, 12–16 severe, 17–21 extremely severe, 22–24 vegetative state, 25–29 extreme vegetative state) [19]. The DRS was completed on the day of discharge (including DAMA), and the patient’s welfare was inquired about at 2 and 4 months after discharge to maintain contact and facilitate final evaluations. The 6-month outcome evaluations were performed with the structured interview for GOSE (death, vegetative state, lower or upper severe disability, upper and lower moderate disability, or good recovery) and QoLIBRI (<60 impaired, 60–66 borderline, 67–82 normal, >82 above average). In the majority of the cases, the 6-month outcomes were completed by telephone interviews since patients were from faraway areas (a few were completed in person). To limit the bias of subjectivity on the part of the patients, we interviewed both the patients and their relatives.
2.5. Data Management and Analysis
Continuous variables were reported as medians with 25th and 75th percentiles and as means and standard deviations. Categorical variables were described as frequencies and percentages. Comparisons between two categorical variables were done using the chi-square test or Fisher exact test (when the expected frequency was less than 5). p-values < 0.05 were considered statistically significant.
2.6. Ethical Clearance and Administrative Authorizations
Ethical clearance for the study was obtained from the Institutional Review Board of the Faculty of Health Sciences (IRB-FHS), University of Buea (Reference N° 1238-08), and administrative authorization was obtained from LHD. Informed consent was given by the participants or their family members, and all data collected was kept strictly confidential with physical and electronic barriers.
3. Results
3.1. Presentation of Sociodemographic and Clinical Features
The study enrolled 160 patients with TBI between January 2021 and February 2022. The median age was 32 (26, 39). Most patients were adolescents/adults aged 15–45 years (78%; 125); 90% of patients were males (144/160). Most participants (76%) had not finished secondary education, and approximately two-thirds were of low economic status (65%). The most common professional group was commercial bike riders (27%; 43/160). Most of the participants who were drivers had no driving licence (81%; 73/90). More than half of the patients (61%; 97) were alcohol consumers or smokers (59%; 95), and pre-existing hypertension was present in 14 (8.8%) patients (Table 1).

Table 1.
Sociodemographic characteristics.
3.2. Clinical Details of Participants
The two most common clinical manifestations of TBI among participants were headache and loss of consciousness (74%; 119 and 98%; 156), respectively. The median GCS was 12.0 (8.0–14.0), and an eye-opening score of 4, verbal response of 4, and motor response of 6 were the most frequently recorded component scores. There was no pupil reaction in 5 (3.1%) of the cases, and the median heart rate was 88 (78 to 99). About 75% of the victims had a normal temperature (131, or 91%), while 3 (2.1%) had hypothermia. Driving after alcohol consumption was suspected in 33 (21%) of the cases (Table 2).
Table 2.
Clinical details of TBI patients.
3.3. Injury Details of Participants
The main cause of TBI was RTIs in 136 (85%), and 60% of these involved a motorcyclist. Other causes of TBI admissions at LHD included assault by a blunt instrument (7.5%, 12) and falls (5%, 8) (Table 3).
Table 3.
Injury details of TBI patients.
3.4. Pre-Hospital Details of TBI Patients
A total of 95 patients (59%) were secondarily referred from other health facilities, and only 65 (41%) were transported directly from the injury site. The main form of transportation was by non-medical means (91%; 145/160). Only one patient (1/65) was transported from the injury site to the hospital by ambulance. Of those referred from other health structures (n = 95), 14 patients (15%) were transported by ambulances (Table 4).
Table 4.
Pre-hospital details of study participants.
3.5. Injury Characteristics and Management
Isolated TBI occurred in 88% (141/160) of the cases, and only a few cases (12%; 19/160) had TBI and other associated trauma. Mild TBI cases were the most common presentation form (41%; 66/160), followed by moderate (34%; 55/160) and severe (24%; 39/160) TBI. A CT scan was not obtained in 22% of TBI cases, and financial constraint was the main reason. When performed, CT showed traumatic intracranial abnormalities in 64% (77/125) of cases. The two most common types of TBI were cerebral contusion (54%; 65/160) and extradural haemorrhage (49%; 59/160). Skull fractures were seen in 36 (30%) of the cases, and 17 (22% of the 77 victims) required neurosurgical intervention (Table 5).
Table 5.
Characterization of injury, neuro-imaging, and management.
3.6. Discharge Status of Participants
The median hospital stay for non-operated TBI patients was 4.0 days (2.0–6.8), while those who underwent neurosurgery stayed for 7 days (4–11). Twenty-one patients died (13%), of whom 18 had sustained a severe TBI. The median time between injury and death was 24 h. A total of 121 (79%) patients were discharged home, and only 4 (3%) went to rehabilitation services (physiotherapy). Forty-six patients (33%) were discharged against medical advice (DAMA), with financial constraints as the main reason. In survivors, the median disability rating score recorded was 4 (1–10), with 18% of patients (25/139) scoring a good recovery (DRS = 0), as seen in Table 6.
Table 6.
Discharge status of TBI patients.
3.7. Six Months Outcome after Hospital Discharge
At 6-months, 25% of patients (38/152) had an unfavourable outcome (GOSE 1–4), and 75% (114/152) had a favourable outcome (GOSE 5–8). “One DAMA patient had died since discharge, increasing the overall mortality rate to 14% (22). The GOSE assessment was missing for eight patients. The QoLIBRI identified 36 patients as impaired (28%; 36/130), as shown in Table 7a. Differences in outcome between surviving patients discharged against medical advice (DAMA) versus those completing hospital treatment were explored; no clear difference (p = 0.6) was found in the unfavourable outcomes of 15% (6/40) and 12% (11/90), respectively, but a significant difference (p = 0.019) was found in the number of patients with impaired scores on the QoLIBRI of 39% (16/41) vs. 22% (20/89) as shown in Table 7b.
Table 7.
(a) Outcome at discharge with DRS and 6 months’ outcome with GOSE and QoLIBRI. (b) Correlation between discharge against medical advice and 6-month outcome.
3.8. Comparison of Six-Month TBI Outcomes and Time Difference between Injury and Arrival, Type of Referral, and TBI Severity
There was no statistically significant difference in outcomes comparing TBI severity and arrival at the hospital (0.847 and 0.577, DRS, QoLIBRI, and GOSE, respectively) (Table S1). Likewise, we found no difference between direct or indirect referrals and discharge outcomes in the DRS (p = 0.061), the 6-month outcomes using the GOSE (p = 0.067), or the quality of life after brain injury score (p = 0.8) (Table S2). As expected, a statistically significant correlation was seen with the injury severity and outcomes (discharge and 6-months) for DRS, GOSE, and QoLIBRI (Table S3).
4. Discussion
This study presented the characteristics of TBI and outcomes at a level one trauma centre in Douala, Cameroon, with the aim of identifying measures to improve TBI prevention and care.
4.1. Demographic and Injury Characteristics
We enrolled 160 TBI cases, of whom the majority (78%) were aged 15–45 years and predominantly male (90%), consistent with other reports from LMICs [20,21]. Most of the participants (76%, 122/160) had not finished secondary education. As noted by Ashkan et al. [22] and Amram et al. [23], low educational levels constitute one of the specific risk factors for RTIs and assaults and are greatly understudied in low-resource settings. RTIs were the main cause of TBI (85%) and often involved commercial bike riders, which is in line with a 5-year retrospective study conducted in Cameroon by Buh et al. [24]. In Cameroon, many youths are involved in hazardous occupations like commercial bike riding as better jobs are difficult to obtain. In addition, recent socio-political insecurity in the two English-speaking regions (the Anglophone crisis) has led to a rural exodus of youths into Douala. These young citizens are frequently involved in commercial bike riding, often without helmets, and seldom have a driving license, and are hence ignorant of the highway codes and traffic laws [25]. In contrast to LMICs, falls are the main cause of TBI in developed countries [26,27]. This difference in the causes observed can be explained by the fact that HICs have better road infrastructure and the implementation of safety road practises is stricter than in most LMICs, including Cameroon.
Many of the TBI patients involved in the RTIs (81%, 73/90) were drivers without a license. This high percentage of motor vehicle and motorcycle drivers without driving licences is in line with the Cameroon government’s 2019 statistics, where 70% of RTIs were reported to originate from human causes, including a lack of driving licences or illegal driving licences [28]. Furthermore, the use of helmets and seat belts is not a common practise in Cameroon and SSA [29]. The low socioeconomic status of TBI patients could explain the relatively high DAMA cases, as suggested by Amram et al. [23]. Moreover, the majority of the citizens are not insured, hence not able to meet the financial costs of TBI care.
More than half of the TBI victims were alcohol consumers (61%), which corroborates a study in Cameroon that reported high alcohol consumption rates of 41% of men and 25.8% of women [30]. Our result, however, differs from the study of Wakabayashi et al. [31] in Thailand, where only 11.6% of TBI cases consumed alcohol. This low alcohol consumption in Thailand may be explained by religious restrictions compared to Cameroon, where the majority are Christians who, in most cases, are not restricted from alcohol consumption. Alcohol consumption before driving, a reported risk factor for RTIs, was suspected in 21% of cases, which is frequently reported in the literature [32,33]. Hypotension, often associated with negative outcomes after TBI, was registered in 19 (12%) cases, twice the rate reported by Landes et al. [33] in Ethiopia.
4.2. Pre-Hospital Care and Post-Acute Care
The results of our study are highly illustrative of the specific challenges and disparities in care in low-resource settings. The main transportation means of TBI cases were through non-medical means (91%), similar to reports by Motah et al. [15] and Buh et al. [24]. Only one patient was transferred from the scene of the accident to the study centre by ambulance. Of patients secondarily referred, only 14 (15%) inter-hospital transports were by ambulance; the others were by taxi or private vehicle. These observations highlight the deficiency of emergency transport systems in LMICS, like Cameroon.
The median length of stay (LOS) for non-operated TBI victims was 4.0 days (2.0, 6.8), which is in line with the study of Tesfay et al. [34] in Ethiopia and Buh et al. [24] in a 5-year retrospective in a Level 1 trauma centre in Douala, Cameroon. Only four (3%) were recommended rehabilitation services (physiotherapy). Unfortunately, acute physiotherapy services were not recommended for hospitalised patients with disabilities, as there are no local standards for physiotherapy referrals for TBI patients. Such therapy is recommended to enhance recovery [35,36,37,38]. The lack of appropriate post-acute care constitutes a major problem in the care of TBI patients, especially in low-income settings, which may greatly impact the outcome of TBI patients. Acute physiotherapy services in TBI can deliver better functional outcomes [38] in SSA, and implementation of these should be high on the policy agenda.
4.3. Disparities in Care due to Financial Constraints
Substantial disparities in care due to deficiencies in the health care system and the financial constraints of patients (or their relatives) were identified, as illustrated in Figure 1. CT scanning on presentation was clinically indicated but not performed in 28 out of 160 patients, of whom 35% (10/28) had moderate or severe TBI. In 26 of these (93%), the reason was the inability of patients or their relatives to pay the costs of a CT scan (75,000 FCFA = 122 USD). Forty-six patients (33%) were discharged against medical advice, with financial constraints as the main reason (100%). This rate of DAMA is much higher than the reported rates in high-income countries of 2.8%, 1.9%, and 1.8% by Kim et al. [39], Guise et al. [40], and Marcoux et al. [41]. DAMA cases are disproportionately high in low-income settings like Cameroon. Furthermore, the observed rate of 33% is likely an underestimation of the true financial constraint on treatment after TBI in low-resource settings, as a large part of the population lives in poverty. Some TBI patients without financial means remained in the hospital as their family members tried to raise the necessary funds. Two patients registered in this study received treatment and were later not permitted to leave the hospital premises until they settled their debts. This situation likely caused psychological distress and negatively impacted their recovery, as suggested in the literature [42,43,44]. Findings from this study revealed that survivors of DAMA cases were more likely to have disabilities and a poorer quality of life six months after injury than survivors discharged regularly (p = 0.019 for QoLIBRI). No clear difference was found on the GOSE. However, there was a trend towards lower GOSE in DAMA cases, and the absence of statistical significance is likely due to the relatively low sample size. Unfortunately, the negative consequences of financial constraints, such as DAMA, remain largely unreported in LMICs where the burden of TBI is significant.
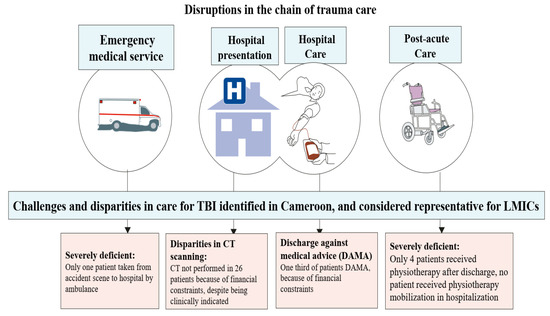
Figure 1.
Disruptions in the chain of trauma care. TBI: Traumatic Brain Injury, LMICs: Low-Middle-Income Countries, CT: Computed Tomography, DAMA: Discharged Against Medical Advice, H: Hospital.
4.4. Outcome
Mortality occurred in 22 patients (14%), consistent with the 10–24% mortality reported by Pelieu et al. [45] in Switzerland, Tesfay et al. [34] in Ethiopia, and El-Menyar et al. [21] in the Middle East. The median time between injury and death was 1 day, much lower than reported in the study of Gao et al. [46], where mortality occurred within 14 days. This difference can likely be explained by the exclusion of cases that died at the emergency service in the study by Gao et al. [46] and also by the higher healthcare standards in China compared to Cameroon. The mortality rate of severe TBI victims in this study (46%, 18/39) is disproportionately high compared with high-income countries. Lu et al. [47] reported a mortality rate of 27% for patients with severe TBI in 1996 in HICs, and the European CENTER-TBI study (2014–2017) reported a mortality rate of 27.8% (Maas, personal communication). This higher death rate with severe TBI in LMICs could be explained by little or no pre-hospital care, limited resources, and financial constraints faced by patients to obtain the necessary health care. Another factor that would have influenced adverse mortality in severe TBI in this study and that may be overlooked in low-income settings is the lack of intracranial pressure monitoring, as previously reported by Buh et al. [48].
The 6-month GOSE outcomes showed that 44 (29%) patients had an upper-good recovery, 21% had an upper-moderate disability, and 12 (8%) had an upper-severe disability, consistent with reports from Paris, France [49] and Tanzania [6]. Ndoumbe et al. [14] from Cameroon noted that only 12.6% of their patients fully recovered and 55% of cases had permanent disability; however, only severe TBI patients were considered in this study. Using the QoLIBRI, 36 (28%) of patients were impaired, while 46 (36%) had above-average scores, consistent with reports by Born et al. [50] in Switzerland.
4.5. Strengths and Limitations
This is one of the very few studies designed to present the characteristics of TBI patients and their interaction with the outcome in Cameroon. A major strength of this study is its prospective design with the collection of 6-month outcome data and the fact that we outline and discuss poor standards of prehospital and post-acute care and describe how DAMA due to financial constraints adversely affects management and outcome. The results can inform healthcare policies to improve prevention and develop strategies to achieve the best care services, aimed at improving outcomes for patients with TBI in Cameroon and SSA. We hope to increase the sample size and collect data such as O2 saturation, duration before CT, and treatment. Another limitation was the difficulty in following up with patients at the hospital; TBI patients were sometimes admitted to other services/wards, making complete and timely data collection challenging. A few cases (n = 8) were also missed at the 6-month evaluation due to incomplete or inaccurate contact information. Despite these limitations, our results are pertinent, offering insights into the TBI situation in an LMIC. The challenges described in Cameroon are illustrative of the problems that governments and health systems face in low-resource settings.
5. Conclusions
Traumatic brain injury in Cameroon commonly occurs in young males of low educational (76%) and socioeconomic status and often involves commercial bike riders. The main cause of TBI in Cameroon is road traffic accidents. Mortality in patients with severe TBI is disproportionately high compared to high-income countries. We report deficiencies in prehospital and postacute care, which likely negatively impact care and outcome when added to the already poor health resources and infrastructure in resource-limited settings. Substantial disparities in care caused by financial constraints were identified as having a clear adverse effect on outcomes. Implementation of universal health insurance may be expected to improve hospital care and outcomes and reduce the number of DAMA cases. Road traffic safety and the prevention of RTIs should be high on the policy agenda. In terms of care provision, improvement of pre-hospital care and development of post-acute care facilities should be the highest priority.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/medicina59091558/s1. Supplemental Table S1 shows that there was no statistically significant difference in outcomes comparing TBI severity and arrival at the hospital (0.847 and 0.577, DRS, QoLIBRI, and GOSE, respectively). Likewise, Table S2 revealed no difference between direct or indirect referrals and discharge outcomes in the DRS (p = 0.061), the 6-month outcomes using the GOSE (p = 0.067), or the quality of life after brain injury score (p = 0.8). As expected, Table S3 indicated a statistically significant correlation was seen with the injury severity and outcomes (discharge and 6-months) for DRS, GOSE, and QoLIBRI. Table S4: STROBE statement.
Author Contributions
F.C.B.: study design, data collection, writing, I.U.N.S.: study design, editing, A.I.R.M.: study design, editing, M.M.: study design, editing; J.V.P.: editing; E.Y.: data analysis; B.K.M.: editing; F.H.K.: editing; K.W.W.: editing, P.J.A.H.: study design, editing; G.S.T.: study design, editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Institutional Review Board of the Faculty of Health Sciences, University of Buea, Cameroon (IRB-FHS). Reference number: 2022/1238-08/UB/SG/IRB/FHS.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
We acknowledge the administration and health personnel of the Laquintinie Hospital Douala for facilitating the data collection phase. Our gratitude also goes to the NIHR Global Health Research Group on Acquired Brain and Spine Injury, University of Cambridge (UK), for the technical support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Dewan, M.C.; Rattani, A.; Gupta, S.; Baticulon, R.E.; Hung, Y.-C.; Punchak, M.; Agrawal, A.; Adeleye, A.O.; Shrime, M.G.; Rubiano, A.M.; et al. Estimating the global incidence of traumatic brain injury. J. Neurosurg. 2019, 130, 1080–1097. [Google Scholar] [CrossRef]
- Wongchareon, K.; Thompson, H.J.; Mitchell, P.H.; Barber, J.; Temkin, N. IMPACT and CRASH prognostic models for traumatic brain injury: External validation in a South-American cohort. INJ Prev. 2020, 26, 546–554. [Google Scholar] [CrossRef]
- GBD 2016 Traumatic Brain Injury and Spinal Cord Injury Collaborators. Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 56–87. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.; Jiang, B.; Ru, X.; Sun, H.; Fu, J.; Wu, S.; Wang, L.; Wang, L.; Zhang, M.; Liu, B.; et al. For the NESS-China investigators. Prevalence and Altered Causes of Traumatic Brain Injury in China: A Nationwide Survey in 2013. Neuroepidemiology 2020, 54, 106–113. [Google Scholar] [CrossRef]
- Brazinova, A.; Rehorcikova, V.; Taylor, M.S.; Buckova, V.; Majdan, M.; Psota, M.; Peeters, W.; Feigin, V.; Theadom, A.; Holkovic, L.; et al. Epidemiology of Traumatic Brain Injury in Europe: A Living Systematic Review. J. Neurotrauma 2021, 38, 1411–1440. [Google Scholar] [CrossRef]
- Boniface, R.; Lugazia, E.R.; Musa, A.; Kiloloma, O. Management and outcome of traumatic brain injury patients at Muhimbili Orthopaedic Institute Dar es Salaam, Tanzania. Pan Afr. Med. J. 2017, 26, 140. [Google Scholar] [CrossRef]
- Adegboyega, G.; Zolo, Y.; Sebopelo, L.A.; Dalle, D.U.; Dada, O.E.; Mbangtang, C.B.; Tetinou, F.; Kanmounye, U.S.; Alalade, A.F. The Burden of Traumatic Brain Injury in Sub-Saharan Africa: A Scoping Review. World Neurosurg. 2021, 156, e192–e205. [Google Scholar] [CrossRef]
- Toth, A. Advanced Imaging in Traumatic Brain Injury 2017. Ph.D. Thesis, Universitas Quinqueecclesiennsis, Pecs, Hungary, 2017; p. 119. [Google Scholar]
- Djientcheu, V.; Fongang, E.N.; Etoundi, P.O.; Esiene, A.; Motah, M.; Tchaleu, C.; Emakam, E.; Tonye, R.; Nonga, B.N.; Essiben, X.; et al. Mortality of head injuries in Sub-Saharan African countries: The case of the university teaching hospitals of Cameroon. J. Neurol. Sci. 2016, 371, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Najem, D.; Rennie, K.; Ribecco-Lutkiewicz, M.; Ly, D.; Haukenfrers, J.; Liu, Q.; Nzau, M.; Fraser, D.D.; Bani-Yaghoub, M. Traumatic brain injury: Classification, models, and markers. Biochem. Cell Biol. 2018, 96, 391–406. [Google Scholar] [CrossRef]
- National Institute of Neurological Disorders. Traumatic Brain Injury: Hope through Research. 2019. Available online: https://catalog.ninds.nih.gov/sites/default/files/publications/traumatic-brain-injury-hope-through-research_1.pdf (accessed on 2 August 2023).
- Dadas, A.; Washington, J.; Diaz-Arrastia, R.; Janigro, D. Biomarkers in traumatic brain injury (TBI): A review. Neuropsychiatr. Dis. Treat. 2018, 14, 2989–3000. [Google Scholar] [CrossRef] [PubMed]
- Ashley, M.J. Assessment of mild traumatic brain injury. In Traumatic Brain Injury Rehabilitation, Treatment, and Case Management, 4th ed.; Ashley, M.J., Hovda, M.J., Eds.; CRC Press/Taylor & Francis: Boca Raton, FL, USA, 2018; pp. 321–3340. [Google Scholar]
- Ndoumbe, A.; Edu, P.B.N.; Simeu, C.; Takongmo, S. Epidemiological Analysis of 135 Cases of Severe Traumatic Brain Injury Managed at a Surgical Intensive Care Unit. Open J. Mod. Neurosurg. 2018, 8, 119–131. [Google Scholar] [CrossRef][Green Version]
- Motah, M.; Ndoumbe, A.; Massi, D.G.; Bekolo, F.F.; Inemb, G.B.; Moumi, M.; Esene, I.; Chunteng, N.T.; Boukar, Y.E.; Eyenga, V.-C. Traumatic intracranial haemorrhage in Cameroon: Clinical features, treatment options and outcome. Interdiscip. Neurosurg. 2021, 26, 101346. [Google Scholar] [CrossRef]
- Eaton, J.; Hanif, A.B.; Grudziak, J.; Charles, A. Epidemiology, Management, and Functional Outcomes of Traumatic Brain Injury in Sub-Saharan Africa. World Neurosurg. 2017, 108, 650–655. [Google Scholar] [CrossRef] [PubMed]
- World Population Review. Douala Population 2023. Available online: https://worldpopulationreview.com/world-cities/doualapopulation (accessed on 20 June 2023).
- National Heart, Lung and Blood Institute. Low Blood Pressure. Consulted 26 March 2022; 2022. Available online: https://www.nih.gov/about-nih/what-we-do/nih-almanac/national-heart-lung-blood-institute-nhlbi (accessed on 2 August 2023).
- Rappaport, M.; Hall, K.M.; Hopkins, K.; Belleza, T.; Cope, D.N. Disability rating scale for severe head trauma: Coma to community. Arch. Phys. Med. Rehabil. 1982, 63, 118–123. [Google Scholar]
- Mehmood, A.; Zia, N.; Kobusingye, O.; Namaganda, R.H.; Ssenyonjo, H.; Kiryabwire, J.; Hyder, A.A. Determinants of emergency department disposition of patients with traumatic brain injury in Uganda: Results from a registry. Trauma Surg. Acute Care Open 2018, 3, e000253. [Google Scholar] [CrossRef]
- El-Menyar, A.; Mekkodathil, A.; Al-Thani, H.; Consunji, R.; Latifi, R. Incidence, Demographics, and Outcome of Traumatic Brain Injury in The Middle East: A Systematic Review. World Neurosurg. 2017, 107, 6–21. [Google Scholar] [CrossRef] [PubMed]
- Sami, A.; Moafian, G.; Najafi, A.; Aghabeigi, M.-R.; Yamini, N.; Heydari, S.T.; Lankarani, K.-B. Educational level and age as contributing factors to road traffic accidents. Chin. J. Traumatol. 2013, 16, 281–285. [Google Scholar]
- Amram, O.; Schuurman, N.; Pike, I.; Yanchar, N.L.; Friger, M.; McBeth, P.B.; Griesdale, D. Socio Economic Status and Traumatic Brain Injury amongst Pediatric Populations: A Spatial Analysis in Greater Vancouver. Int. J. Environ. Res. Public Health 2015, 12, 15594–15604. [Google Scholar] [CrossRef]
- Buh, F.C.; Taiwe, G.S.; Maas, A.I.R.; Motah, M.; Youm, E.; Wanyu, B.Y.; Wang, K.W.; Hutchinson, P.J.A.; Sumbele, I.U.N. Demographics, Causes, and Outcome of Traumatic Brain Injury among Trauma Cases in Cameroon: A Multi-Center Five Year’s Retrospective Study. Neurotrauma Rep. 2022, 3, 569–583. [Google Scholar] [CrossRef]
- Kouagheu, J. Au Cameroun, dans la jungle des motos-taxisA Douala, sept accidents de la circulation sur dix sont causés par les bend-skinneurs, ces jeunes chauffeurs sans le sou et, souvent, sans permis de conduire. Monde Afr 2020. Available online: https://www.lemonde.fr/afrique/article/2020/02/03/au-cameroun-dans-la-jungle-des-motos-taxis_6028276_3212.html (accessed on 2 August 2023).
- Fu, T.S.; Jing, R.; McFaull, S.R.; Cusimano, M.D. Health & Economic Burden of Traumatic Brain Injury in the Emergency Department. Can. J. Neurol. Sci. 2016, 43, 238–247. [Google Scholar]
- Steyerberg, E.W.; Wiegers, E.; Sewalt, C.; Buki, A.; Citerio, G.; De Keyser, V.; Ercole, A.; Kunzmann, K.; Lanyon, L.; Lecky, F.; et al. CENTER-TBI Participants and Investigators. Case-mix, care pathways, and outcomes in patients with traumatic brain injury in CENTER-TBI: A European prospective, multicentre, longitudinal, cohort study. Lancet Neurol. 2019, 18, 923–934. [Google Scholar] [CrossRef] [PubMed]
- Isah, M. Multisectorial Approach in Reducing Road Traffic Accidents in Cameroon. Nfafu Policy Institute. 2020. Available online: https://nkafu.org/multi-sectorial-approach-in-reducing-road-traffic-accidents-in-cameroon/ (accessed on 2 August 2023).
- Bezabeh, G.B.; Souare, M.; Oumarou, A. Road Safety in Africa Assessment of Progresses and Challenges in Road Safety Management System 2013; African Development Bank Group: Tunis, Tunisia, 2013. [Google Scholar]
- Kongnyuy, E.J.; Wiysonge, C.S. Alcohol use and extramarital sex among men in Cameroon. BMC Int. Health Hum. Rights 2007, 7, 6. [Google Scholar] [CrossRef]
- Wakabayashi, M.; McKetin, R.; Banwell, C.; Yiengprugsawan, V.; Kelly, M.; Seubsman, S.-A.; Iso, H.; Sleigh, A.; Thai Cohort Study Team. Alcohol consumption patterns in Thailand and their relationship with non-communicable disease. BMC Public Health 2015, 15, 1297. [Google Scholar] [CrossRef] [PubMed]
- Pawłowski, W.; Lasota, D.; Goniewicz, M.; Rzońca, P.; Goniewicz, K.; Krajewski, P. The Effect of Ethyl Alcohol upon Pedestrian Trauma Sustained in Traffic Crashes. Int. J. Environ. Res. Public Health 2019, 16, 1471. [Google Scholar] [CrossRef] [PubMed]
- Landes, M.; Venugopal, R.; Berman, S.; Heffernan, S.; Maskalyk, J.; Azazh, A. Epidemiology, clinical characteristics and outcomes of head injured patients in an Ethiopian emergency centre. Afr. J. Emerg. Med. 2017, 7, 130–134. [Google Scholar] [CrossRef]
- Tesfay, M. Clinical Profile and Outcome of Traumatic Brain Injury Patients at the Emergency Department of AaBET Hospital. Master’s Thesis, College of Health Science, Addis Ababa University, Addis Ababa, Ethiopia, 2020. [Google Scholar]
- Foster, M.; Tilse, C. Referral to rehabilitation following traumatic brain injury: A model for understanding inequities in access. Soc. Sci. Med. 2003, 56, 2201–2210. [Google Scholar] [CrossRef]
- Hellweg, S.; Johannes, S. Physiotherapy after traumatic brain injury: A systematic review of the literature. Brain Inj. 2008, 22, 365–373. [Google Scholar] [CrossRef]
- Lendraitienė, E.; Petruševičienė, D.; Savickas, R.; Žemaitienė, I.; Mingaila, S. The impact of physical therapy in patients with severe traumatic brain injury during acute and post-acute rehabilitation according to coma duration. J. Phys. Ther. Sci. 2016, 28, 2048–2054. [Google Scholar] [CrossRef]
- John Hopkins Medicine. Rehabilitation after Traumatic Brain Injury. 2023. Available online: https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/rehabilitation-after-traumatic-brain-injury (accessed on 2 August 2023).
- Kim, Y.J. The Impact of Time from ED Arrival to Surgery on Mortality and Hospital Length of Stay in Patients with Traumatic Brain Injury. J. Emerg. Nurs. 2011, 37, 328–333. [Google Scholar] [CrossRef]
- de Guise, E.; LeBlanc, J.; Dagher, J.; Tinawi, S.; Lamoureux, J.; Marcoux, J.; Maleki, M.; Feyz, M. Characteristics of patients with acute traumatic brain injury discharged against medical advice in a Level 1 urban trauma centre. Brain Inj. 2014, 28, 1288–1294. [Google Scholar] [CrossRef]
- Marcoux, J.; Alkutbi, M.; Lamoureux, J.; Feyz, M.; Saluja, R.S.; de Guise, E. Discharge against Medical Advice in Traumatic Brain Injury: Follow-Up and Readmission Rate. Can. J. Neurol. Sci. 2017, 44, 311–317. [Google Scholar] [CrossRef]
- Kalogriopoulos, N.A.; Baran, J.; Nimunkar, A.J.; Webstar, J.G. Electronic Medical Record Systems for Developing Countries: Review. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 1730–1733. Available online: https://ewh.slc.engr.wisc.edu/publications/conferences/2009/IEEEEMBC/KalogriopoulosNWMedRSIEEEMBC2009.pdf (accessed on 26 August 2023).
- Ramakrishnan, N.; Ranganathan, L.; Abraham, B.K.; Rajagopalan, S.; Venkataraman, R. What Happens to Patients Discharged Against Medical Advice? Indian J. Crit. Care Med. 2018, 22, 580–584. [Google Scholar]
- Albayati, A.; Douedi, S.; Alshami, A.; Hossain, M.A.; Sen, S.; Buccellato, V.; Cutroneo, A.; Beelitz, J.; Asif, A. Why Do Patients Leave against Medical Advice? Reasons, Consequences, Prevention, and Interventions. Healthcare 2021, 9, 111. [Google Scholar] [CrossRef] [PubMed]
- Pélieu, I.; Kull, C.; Walder, B. Prehospital and Emergency Care in Adult Patients with Acute Traumatic Brain Injury. Med. Sci. 2019, 7, 12. [Google Scholar] [CrossRef]
- Gao, G.; Wu, X.; Feng, J.; Hui, J.; Mao, Q.; Lecky, F.; Lingsma, H.; Maas, A.I.R.; Jiang, J. Clinical characteristics and outcomes in patients with traumatic brain injury in China: A prospective, multicentre, longitudinal, observational study. Lancet Neurol. 2020, 19, 670–677. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Marmarou, A.; Choi, S.; Maas, A.; Murray, G.; Steyerberg, E.W. Impact and Abic Study Group. Mortality from traumatic brain injury. Acta Neurochir. 2005, 95, 281–285. [Google Scholar]
- Buh, F.C.; Hutchinson, P.J.A.; Anwar, F. Early neuro-rehabilitation in traumatic brain injury: The need for an African perspective. BMC Med. 2023, 21, 290. [Google Scholar] [CrossRef]
- Ruet, A.; Bayen, E.; Jourdan, C.; Ghout, I.; Meaude, L.; Lalanne, A.; Pradat-Diehl, P.; Nelson, G.; Charanton, J.; Aegerter, P.; et al. A Detailed Overview of Long-Term Outcomes in Severe Traumatic Brain Injury Eight Years Post-injury. Front. Neurol. 2019, 10, 120. [Google Scholar] [CrossRef]
- Born, K.; Amsler, F.; Gross, T. Prospective evaluation of the Quality of Life after Brain Injury (QOLIBRI) score: Minor differences in patients with major versus no or mild traumatic brain injury at one-year follow up. Heal. Qual. Life Outcomes 2018, 16, 136. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).