

Urolithiasis in Kidney Transplant Patients: A Multicenter KSER Research Series


 ,
,  on behalf of the Korean Society of Endourology and Robotics (KSER) Research Committee
on behalf of the Korean Society of Endourology and Robotics (KSER) Research Committee
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. Classification from Cohort
2.3. Treatment for Stone Disease
2.4. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Stone Characteristics
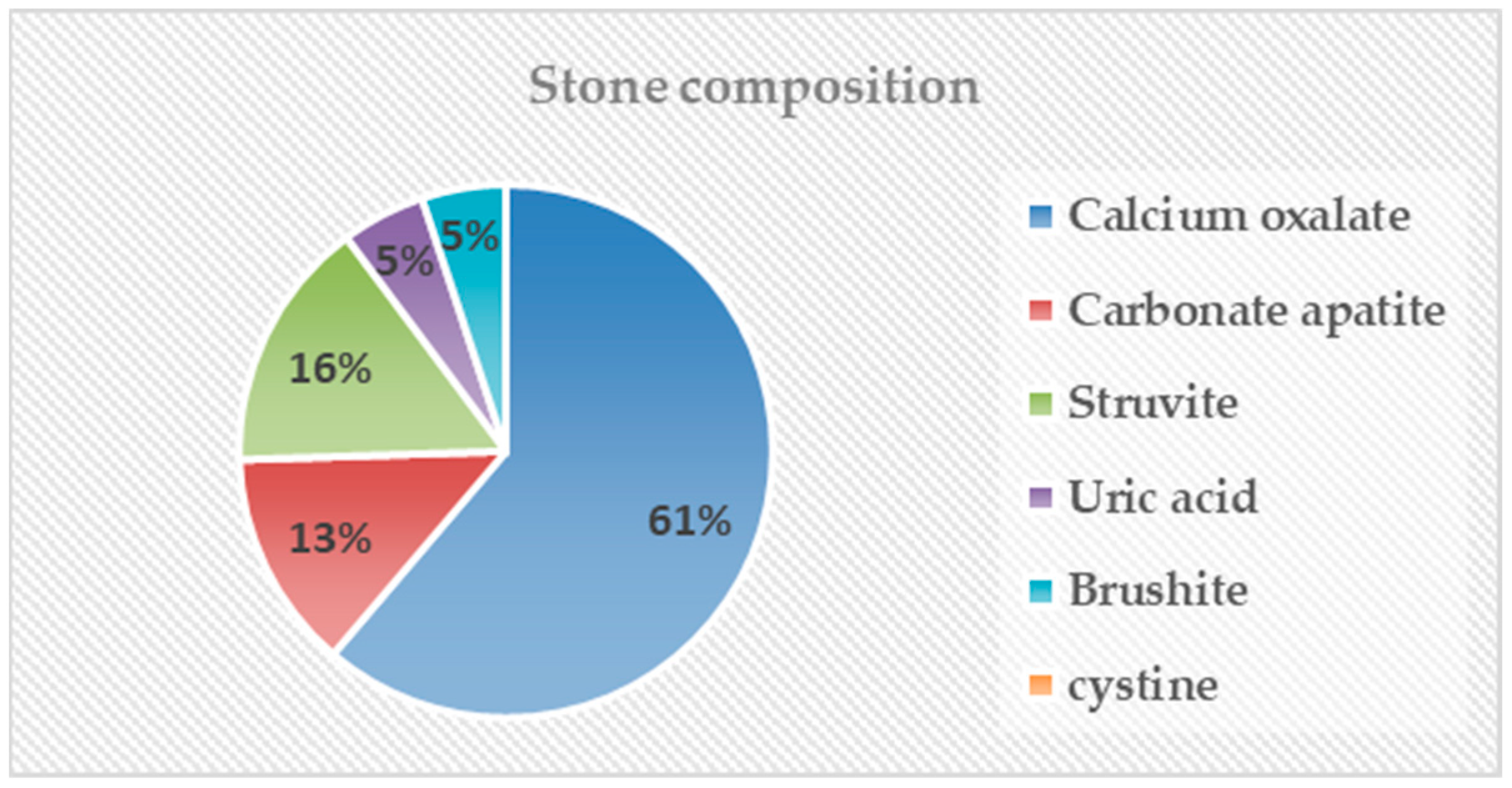
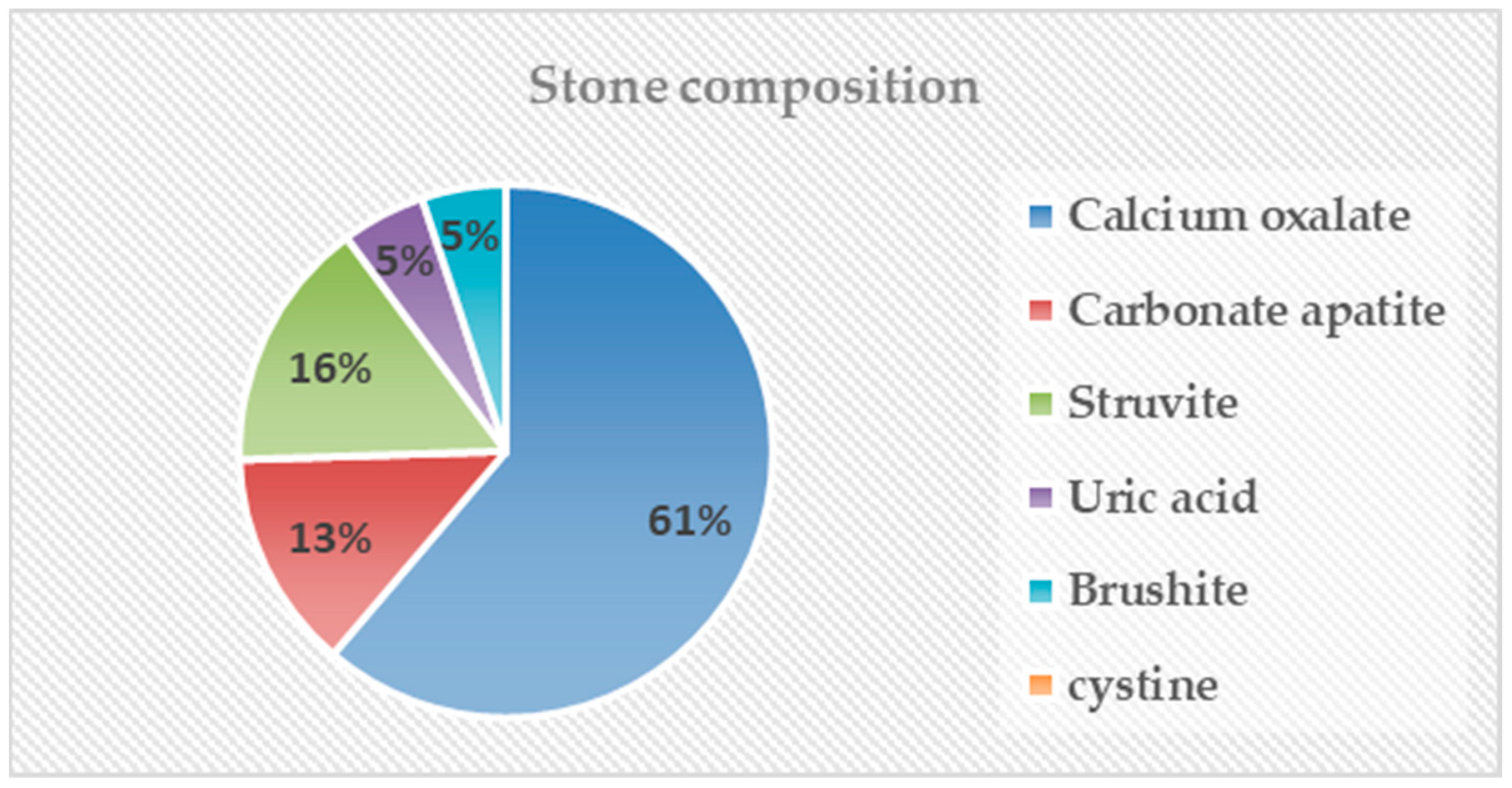
3.3. Stone Composition
3.4. Causes of Stone Formation
3.5. Management of Disease
3.6. Treatment Outcome
4. Discussion

{kind=link}
| Author | StudyDesign | Country | Duration | Stone Patients (n) | Prevalence (%) | Mean Age (Years) | Stone Location (n) | Mean Stone Size | Any Procedure (n) | Treatment Modality (n) | SFR (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Yuan et al. [3] | Single center | China | 2000–2014 | 19 | 1.20% | 38 | Kidney 9 (47.34%)Ureter 9 (47.34%)Both 1 (5.2%) | 4.2 mm | 17/19 (89.5%) | SWL 5 (29.4%)URS 5 (29.4%)PCNL 7 (41.2%) | 100 |
| Challacombe et al. [1] | Single center | UK | 1977–2003 | 21 | 1% | 41 | N/A | 8.1 mm | 19/21 (90.5%) | SWL 12 (63.2%)URS 2 (10.5%)PCNL 3 (15.8%)Others 2 (10.5%) | 100 |
| Emiliani et al. [19] | Single center | Spain | 1983–2017 | 51 | 2.40% | 48.9 | Kidney 19 (37.25%)Ureter 32 (62.75%) | 9 mm | 37/51 (54.4%) | SWL 22 (59.5%)URS 9 (24.3%)PCNL 4 (10.8%)others 2 (5.4%) | 52.9 |
| Verrier et al. [15] | Single center | France | 1978–2010 | 31 | 1.03% | 40.5 | Kidney 11 (35.5%)Ureter 16 (51.6%)Bladder 4 (12.9%) | N/A | 19/31 (61.3%) | SWL 3 (15.8%)URS 5 (26.3%)PCNL 1 (5.2%)Others 10 (51.7%) | 58.1 |
| Current study | Multi center | Korea | 1997–2021 | 58 | N/A | 59.1 | Kidney 15 (25.9%)Ureter 35 (60.3%)Both 8 (13.8%) | 575.8 mm³ | 51/58 (87.9%) | SWL 12 (23.5%)URS 23 (45.1%)PCNL 14 (27.5%)Others 2 (3.9%) | 60.8 |
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Challacombe, B.; Dasgupta, P.; Tiptaft, R.; Glass, J.; Koffman, G.; Goldsmith, D.; Khan, M.S. Multimodal management of urolithiasis in renal transplantation. BJU Int. 2005, 96, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Stravodimos, K.G.; Adamis, S.; Tyritzis, S.; Georgios, Z.; Constantinides, C.A. Renal transplant lithiasis: Analysis of our series and review of the literature. J. Endourol. 2012, 26, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.J.; Yang, D.D.; Cui, Y.S.; Men, C.P.; Gao, Z.L.; Shi, L.; Wu, J.T. Minimally invasive treatment of renal transplant nephrolithiasis. World J. Urol. 2015, 33, 2079–2085. [Google Scholar] [CrossRef]
- Choi, E.J.; Lee, S.H.; Oh, C.K.; Kim, Y.B.; Bang, J.B. Cytomegalovirus-associated hemophagocytic syndrome diagnosed by liver biopsy in a kidney transplant recipient. Yonsei Med. J. 2021, 62, 274–277. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.; Kim, J.; Lee, J.; Choi, S.Y.; Joo, H.J.; Koo, B.N. Effects of the type of intraoperative fluid in living donor kidney transplantation: A single-center retrospective cohort study. Yonsei Med. J. 2022, 63, 380–388. [Google Scholar] [CrossRef]
- Sorokin, I.; Mamoulakis, C.; Miyazawa, K.; Rodgers, A.; Talati, J.; Lotan, Y. Epidemiology of stone disease across the world. World J. Urol. 2017, 35, 1301–1320. [Google Scholar] [CrossRef]
- Jung, H.D.; Lee, J.Y.; Kang, D.H.; Ko, K.; Koh, D.H.; Kwon, O.; Koo, K.C.; Kim, K.T.; Kim, M.S.; Kim, B.S.; et al. Korean society of endourology and robotics (kser) recommendation on the diagnosis, treatment, and prevention of urolithiasis. Investig. Clin. Urol. 2023, 64, 325–337. [Google Scholar] [CrossRef]
- Klingler, H.C.; Kramer, G.; Lodde, M.; Marberger, M. Urolithiasis in allograft kidneys. Urology 2002, 59, 344–348. [Google Scholar] [CrossRef]
- Bhadauria, R.P.; Ahlawat, R.; Kumar, R.V.; Srinadh, E.S.; Banerjee, G.K.; Bhandari, M. Donor-gifted allograft lithiasis: Extracorporeal shockwave lithotripsy with over table module using the lithostar plus. Urol. Int. 1995, 55, 51–55. [Google Scholar] [CrossRef]
- Harper, J.M.; Samuell, C.T.; Hallson, P.C.; Wood, S.M.; Mansell, M.A. Risk factors for calculus formation in patients with renal transplants. Br. J. Urol. 1994, 74, 147–150. [Google Scholar] [CrossRef]
- Zarrabi, A.; Gross, A.J. The evolution of lasers in urology. Ther. Adv. Urol. 2011, 3, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Jeon, S.H. Lasers for the treatment of urinary stone disease. Investig. Clin. Urol. 2021, 62, 241–242. [Google Scholar] [CrossRef]
- Park, S.; Kim, M.; Kim, J.E.; Kim, K.; Park, M.; Kim, Y.C.; Joo, K.W.; Kim, Y.S.; Lee, H. Characteristics of kidney transplantation recipients over time in south korea. Korean J. Intern. Med. 2020, 35, 1457–1467. [Google Scholar] [CrossRef]
- Lieske, J.C.; Rule, A.D.; Krambeck, A.E.; Williams, J.C.; Bergstralh, E.J.; Mehta, R.A.; Moyer, T.P. Stone composition as a function of age and sex. Clin. J. Am. Soc. Nephrol. 2014, 9, 2141–2146. [Google Scholar] [CrossRef] [PubMed]
- Van Gansbeke, D.; Zalcman, M.; Matos, C.; Simon, J.; Kinnaert, P.; Struyven, J. Lithiasic complications of renal transplantation: The donor graft lithiasis concept. Urol. Radiol. 1985, 7, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Verrier, C.; Bessede, T.; Hajj, P.; Aoubid, L.; Eschwege, P.; Benoit, G. Decrease in and management of urolithiasis after kidney transplantation. J. Urol. 2012, 187, 1651–1655. [Google Scholar] [CrossRef]
- Torrecilla Ortiz, C.; González-Satué, C.; Riera Canals, L.; Colom Feixas, S.; Franco Miranda, E.; Aguilo Lucía, F.; Serrallach Mila, N. Incidence and treatment of urinary lithiasis in renal transplantation. Actas Urol. Esp. 2001, 25, 357–363. [Google Scholar] [CrossRef]
- Henderickx, M.; Baard, J.; Wesselman van Helmond, P.C.; Jansen, I.; Kamphuis, G.M. Donor kidney lithiasis and back-table endoscopy: A successful combination. Acta Chir. Belg. 2023, 123, 170–173. [Google Scholar] [CrossRef]
- Emiliani, E.; Subiela, J.D.; Regis, F.; Angerri, O.; Palou, J. Over 30-yr experience on the management of graft stones after renal transplantation. Eur. Urol. Focus. 2018, 4, 169–174. [Google Scholar] [CrossRef]
- Jung, H.D.; Seo, I.Y.; Lee, J.Y. Large database study of urinary stone composition in south korea: Korean society of endourology and robotics (kser) research series. Investig. Clin. Urol. 2021, 62, 462–469. [Google Scholar] [CrossRef]
- Miano, R.; Germani, S.; Vespasiani, G. Stones and urinary tract infections. Urol. Int. 2007, 79 (Suppl. S1), 32–36. [Google Scholar] [CrossRef]
- Gordon, E.J.; Prohaska, T.R.; Gallant, M.P.; Sehgal, A.R.; Strogatz, D.; Yucel, R.; Conti, D.; Siminoff, L.A. Longitudinal analysis of physical activity, fluid intake, and graft function among kidney transplant recipients. Transpl. Int. 2009, 22, 990–998. [Google Scholar] [CrossRef] [PubMed]
- Abou-Elela, A. Epidemiology, pathophysiology, and management of uric acid urolithiasis: A narrative review. J. Adv. Res. 2017, 8, 513–527. [Google Scholar] [CrossRef]
- Hyams, E.; Marien, T.; Bruhn, A.; Quirouet, A.; Andonian, S.; Shah, O.; Matlaga, B. Ureteroscopy for transplant lithiasis. J. Endourol. 2012, 26, 819–822. [Google Scholar] [CrossRef] [PubMed]
- Millán Rodríguez, F.; González de Chaves, E.; Rousaud Barón, F.; Izquierdo Latorre, F.; Rousaud Barón, A. Treatment of urinary calculi in transplanted kidney with extracorporeal shock wave lithotripsy. Arch. Esp. Urol. 2003, 56, 793–798. [Google Scholar] [PubMed]
- Patel, T.; Kozakowski, K.; Hruby, G.; Gupta, M. Skin to stone distance is an independent predictor of stone-free status following shockwave lithotripsy. J. Endourol. 2009, 23, 1383–1385. [Google Scholar] [CrossRef]
- Traxer, O.; Smith, T.G., 3rd; Pearle, M.S.; Corwin, T.S.; Saboorian, H.; Cadeddu, J.A. Renal parenchymal injury after standard and mini percutaneous nephrostolithotomy. J. Urol. 2001, 165, 1693–1695. [Google Scholar] [CrossRef]
- He, Z.; Li, X.; Chen, L.; Zeng, G.; Yuan, J. Minimally invasive percutaneous nephrolithotomy for upper urinary tract calculi in transplanted kidneys. BJU Int. 2007, 99, 1467–1471. [Google Scholar] [CrossRef]
- Taguchi, K.; Yamashita, S.; Hamamoto, S.; Deguchi, R.; Kawase, K.; Okada, T.; Kato, T.; Ando, R.; Okada, A.; Kohjimoto, Y.; et al. Ureteroscopy-assisted puncture for ultrasonography-guided renal access significantly improves overall treatment outcomes in endoscopic combined intrarenal surgery. Int. J. Urol. 2021, 28, 913–919. [Google Scholar] [CrossRef]
| Total | |
|---|---|
| Number of patients | 58 (100.0%) |
| Sex | |
| Male | 37 (63.8%) |
| Female | 21 (36.2%) |
| Previous stone history | 4/58 (6.9%) |
| Age (years) | 59.09 ± 10.70 |
| BMI (kg/m2) | 23.37 ± 3.37 |
| Detection period after KT (months) | 76.26 ± 183.14 |
| Mode of stone detection | |
| Asymptomatic routine check-up | 30 (54.7%) |
| Hematuria | 14 (24.1%) |
| Pain | 4 (6.9%) |
| Urinary tract infection | 3 (5.2%) |
| Other | 7 (12.1%) |
| Multiplicity | |
| Single | 33 (56.9%) |
| Multiple | 25 (43.1%) |
| Location | |
| Kidney | 15 (25.9%) |
| Ureter | 35 (60.3%) |
| Both | 8 (13.8%) |
| Hydronephrosis | 48 (82.8%) |
| Volume of target stone (mm3) | 575.84 ± 1739.69 |
| MSL (mm) | 11.63 ± 9.83 |
| MSD (HU) | 693.40 ± 354.20 |
| Emergency intervention | 25 (43.1%) |
| PCN insertion | 19/25 (76.0%) |
| Ureteral stent insertion | 6/25 (24.0%) |
| Any other procedure | 51 (87.9%) |
| Procedure for initial treatment | |
| SWL | 12 (23.5%) |
| URS | 23 (45.1%) |
| PCNL | 14 (27.5%) |
| Other | 2 (3.9%) |
| Number of Patients | |
|---|---|
| Direct causes | |
| Ureteral stent (left for a prolonged period) | 4 (6.8%) |
| Cadaveric donor | 2 (3.4%) |
| Remnant suture material | 0 (0.0%) |
| Comorbidity | |
| Oliguria | 1 (1.7%) |
| Recurrent urinary tract infection | 1 (1.7%) |
| Stenosis | 2 (3.4%) |
| Voiding difficulty | 2 (3.4%) |
| Vesicoureteral reflux | 0 (0.0%) |
| Renal Stone Group | Ureter Stone Group | p-Value | |
|---|---|---|---|
| Total number of patients | 15 (25.9%) | 43 (74.1%) | |
| Treatment | 0.010 a | ||
| Conservative care | 5 (33.3%) | 2 (4.7%) | |
| Any other procedure | 10 (66.7%) | 41 (95.3%) | |
| Need for emergency intervention | 0.036 a | ||
| No | 12 (80.0%) | 21 (48.8%) | |
| Yes | 3 (20.0%) | 22 (51.2%) | |
| Initial treatment option | 0.562 a | ||
| SWL | 3 (30.0%) | 9 (21.9%) | 0.682 b |
| URS | 3 (30.0%) | 20 (48.8%) | 0.480 b |
| PCNL | 4 (40.0%) | 10 (24.4%) | 0.432 b |
| Others | 0 (0.0%) | 2 (4.9%) | - |
| Stone-free rate | 6/10 (60.0%) | 26/41 (63.4%) | 0.924 a |
| Operation success rate | 7/10 (70.0%) | 32/41 (78.0%) | 0.881 a |
| Variable | Total | Non-Stone-Free Group | Stone-Free Group | p-Value |
|---|---|---|---|---|
| Number of patients | 49 | 17 | 32 | |
| Age (years) | 58.57 ± 11.01 | 55.88 ± 11.94 | 61.00 ± 9.73 | 0.105 |
| BMI (kg/m2) | 23.55 ± 3.49 | 23.30 ± 3.86 | 23.1 ± 2.47 | 0.431 |
| Detection period (months) | 71.00 ± 191.88 | 111.35 ± 325.17 | 49.44 ± 58.00 | 0.406 |
| Target stone volume (mm3) | 647.82 ± 1845.49 | 1311.94 ± 3087.56 | 298.98 ± 447.27 | 0.004 |
| MSL (mm) | 11.81 ± 10.27 | 14.34 ± 15.65 | 10.55 ± 6.18 | 0.003 |
| MSD (HU) | 738.84 ± 344.14 | 864.91 ± 394.40 | 680.15 ± 311.74 | 0.106 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shim, K.H.; Choi, K.B.; Kim, W.B.; Yang, S.W.; Kim, D.K.; Choo, M.S.; Chung, D.Y.; Jung, H.D.; Lee, S.W.; Kim, B.S.; et al. Urolithiasis in Kidney Transplant Patients: A Multicenter KSER Research Series. Medicina 2024, 60, 132. https://doi.org/10.3390/medicina60010132
Shim KH, Choi KB, Kim WB, Yang SW, Kim DK, Choo MS, Chung DY, Jung HD, Lee SW, Kim BS, et al. Urolithiasis in Kidney Transplant Patients: A Multicenter KSER Research Series. Medicina. 2024; 60(1):132. https://doi.org/10.3390/medicina60010132
Chicago/Turabian StyleShim, Kang Hee, Kwi Bok Choi, Woong Bin Kim, Seung Woo Yang, Do Kyung Kim, Min Soo Choo, Doo Yong Chung, Hae Do Jung, Sin Woo Lee, Bum Soo Kim, and et al. 2024. "Urolithiasis in Kidney Transplant Patients: A Multicenter KSER Research Series" Medicina 60, no. 1: 132. https://doi.org/10.3390/medicina60010132
APA StyleShim, K. H., Choi, K. B., Kim, W. B., Yang, S. W., Kim, D. K., Choo, M. S., Chung, D. Y., Jung, H. D., Lee, S. W., Kim, B. S., Jeon, S. H., Kang, S. H., Paick, S., & Lee, J. Y., on behalf of the Korean Society of Endourology and Robotics (KSER) Research Committee. (2024). Urolithiasis in Kidney Transplant Patients: A Multicenter KSER Research Series. Medicina, 60(1), 132. https://doi.org/10.3390/medicina60010132