
Giant Congenital Hemangioma of the Skull: Prenatal Diagnosis and Multimodal Endovascular and Surgical Management

 , , , and
, , , and
Abstract
:1. Introduction
2. Case Report
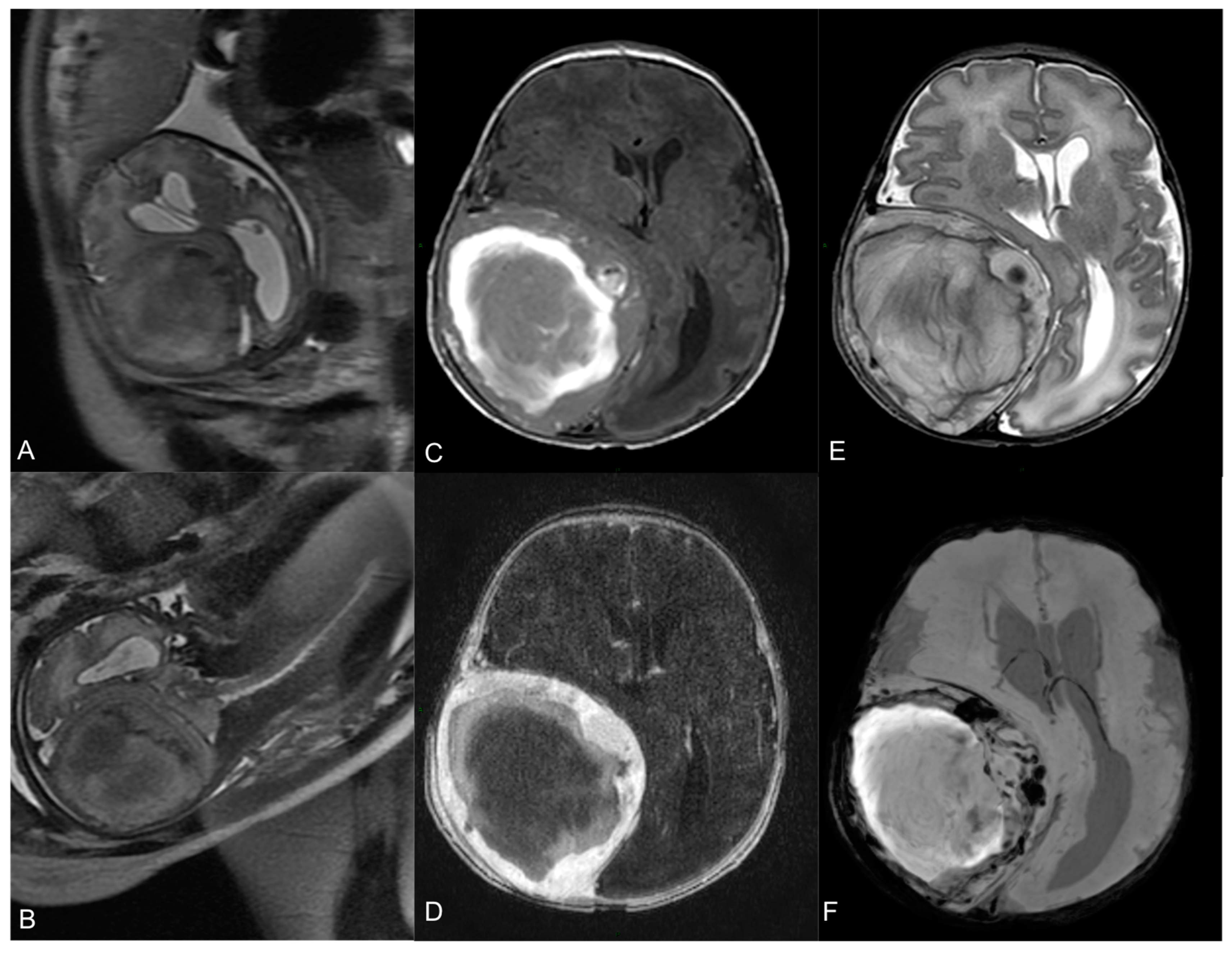
2.1. Presentation and Clinical Characteristics
2.2. Endovascular Embolization and Surgical Treatment
3. Discussion

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors, Year | n° Cases | Location | Radiological Aspect | Management | Histopathology |
|---|---|---|---|---|---|
| Yoshida et al., 1999 [16] | 1 | Lt Parietal | Skull bone thickening | Surgery | Cavernous |
| Koulouris et al., 2005 [9] | 1 | Multiple | Space-occupying lesions + Skull bone thickening | Prednisolone + Biopsy | n.a. |
| Elia et al., 2008 [12] | 2 | Rt occipital Lt frontal | Space-occupying lesion with extracranial extension Skull bone thickening | Spontaneous regression Spontaneous regression | n.a |
| Vural et al., 2009 [13] | 1 | Rt Parietal | Skull bone thickening | Surgery | Cavernous |
| Martìnez-Lage et al., 2010 [11] | 1 | Lt Parietal | Skull bone thickening | Surgery | Cavernous |
| Yucel et al., 2010 [14] | 1 | Rt Parietal | Skull bone thickening | Surgery | Cavernous |
| Rumana et al., 2013 [15] | 1 | Rt Parietal | Skull bone thickening | Surgery | Cavernous |
| Brichacek et al., 2018 [2] | 1 | Rt Parietal | Skull bone thickening | Biopsy + Propranolol | Cavernous |
| Benvenisti et al., 2014 [17] | 1 | Lt Occipital | Space-occupying lesion with intracranial extension | Biopsy + Propranolol | n.a. |
| Present study | 1 | Rt Fronto-Parietal | Space-occupying lesion with large intracranial extension | Endovascular Embolization + Surgery | Capillary |
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- North, P.E. Classification and Pathology of Congenital and Perinatal Vascular Anomalies of the Head and Neck. Otolaryngol. Clin. N. Am. 2018, 51, 1–39. [Google Scholar] [CrossRef] [PubMed]
- Brichacek, M.; Naeem, A.; Filler, G.; Hammond, R.; Yazdani, A.; Ranger, A. Congenital calvarial hemangioma. J. Craniofac. Surg. 2018, 29, 1625–1628. [Google Scholar] [CrossRef] [PubMed]
- Hook, S.R.; Font, R.L.; McCrary, J.A.; Harper, R.L. Intraosseous capillary hemangioma of the frontal bone. Am. J. Ophthalmol. 1987, 103, 824–827. [Google Scholar] [CrossRef] [PubMed]
- Pastore, F.S.; De Caro, G.M.; Faiola, A.; Mauriello, A.; Giuffrè, R. Cavernous hemangioma of the parietal bone. Case report and review of the literature. Neurochirurgie 1999, 45, 312–315. [Google Scholar] [PubMed]
- Prasad, G.L.; Pai, K. Pediatric cranial intraosseous hemangiomas: A review. Neurosurg. Rev. 2018, 41, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Warren, T.A.; Gandhi, M.; Panizza, B. Pictorial review: Vascular anomalies of the head and neck. J. Med. Imaging Radiat. Oncol. 2012, 56, 84–92. [Google Scholar] [CrossRef]
- Goyal, P.; Mangla, R.; Gupta, S.; Malhotra, A.; Almast, J.; Sapire, J.; Kolar, B. Pediatric Congenital Cerebrovascular Anomalies. J. Neuroimaging 2019, 29, 165–181. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.S.; Snelling, B.M.; Sur, S.; Ramnath, A.; Bandstra, E.; Yavagal, D. Scalp congenital hemangioma with associated high-output cardiac failure in a premature infant: Case report and review of literature. Interv. Neuroradiol. 2017, 23, 102–106. [Google Scholar] [CrossRef]
- Koulouris, G.; Rao, P. Multiple congenital cranial hemangiomas. Skeletal Radiol. 2005, 34, 485–489. [Google Scholar] [CrossRef] [PubMed]
- Johnson, E.F.; Davis, D.M.; Tollefson, M.M.; Fritchie, K.; Gibson, L.E. Vascular tumors in infants: Case report and review of clinical, histopathologic, and immunohistochemical characteristics of infantile hemangioma, pyogenic granuloma, noninvoluting congenital hemangioma, tufted angioma, and kaposiform hemangioendothelioma. Am. J. Dermatopathol. 2018, 40, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Lage, J.F.; Torroba, M.A.; Pérez, B.C.; Almagro, M.J.; Lòpez-Guerrero, A.L.; de la Rosa, P. Cavernous hemangiomas of the cranial vault in infants: A case-based update. Child’s Nerv. Syst. 2010, 26, 861–865. [Google Scholar] [CrossRef] [PubMed]
- Elia, D.; Garel, C.; Enjolras, O.; Vermouneix, L.; Soupre, V.; Oury, J.-F.; Guibaud, L. Prenatal imaging findings in rapidly involuting congenital hemangioma of the skull. Ultrasound Obstet. Gynecol. 2008, 31, 572–575. [Google Scholar] [CrossRef] [PubMed]
- Vural, M.; Acikalin, M.F.; Adapinar, B.; Atasoy, M.A. Congenital cavernous hemangioma of the calvaria: Case report. J. Neurosurg. Pediatr. 2009, 3, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Yucel, E.; Akkaya, H.; Gürkanlar, D.; Ergun, T. Congenital cavernous hemangioma of the skull. Turk. Neurosurg. 2011, 21, 645–647. [Google Scholar] [PubMed]
- Rumana, M.; Khursheed, N.; Farhat, M.; Othman, S.; Masood, L. Congenital intraosseous cavernous hemangioma of the skull: An unusual case. Pediatr. Neurosurg. 2013, 49, 229–231. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, D.; Sugisaki, Y.; Shimura, T.; Teramoto, A. Cavernous hemangioma of the skull in a neonate. Child’s Nerv. Syst. 1999, 15, 351–353. [Google Scholar] [CrossRef] [PubMed]
- Benvenisti, H.; Ben-Sira, L.; Constantini, S.; Roth, J. Giant cranial and cerebellar hemangioma treated with propranolol. Child’s Nerv. Syst. 2015, 31, 805–808. [Google Scholar] [CrossRef] [PubMed]
- Haine, E.; Sevely, A.; Boetto, S.; Delisle, M.B.; Cances, C. Infantile Hemangioma of the Posterior Fossa in a Newborn: Early Management and Long-Term Follow-Up. Neuropediatrics 2017, 48, 378–381. [Google Scholar] [CrossRef] [PubMed]
- Frei-Jones, M.; McKinstry, R.C.; Perry, A.; Leonard, J.R.; Park, T.S.; Rubin, J.B. Use of thalidomide to diminish growth velocity in a life-threatening congenital intracranial hemangioma: Case report. J. Neurosurg. Pediatr. 2008, 2, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Pedicelli, A.; Iacobucci, M.; Frassanito, P.; Lozupone, E.; Masselli, G.; Di Rocco, C.; Colosimo, C. Prenatal Diagnosis and Multimodal Neonatal Treatment of a Rare Pial Arteriovenous Fistula: Case Report and Review of the Literature. World Neurosurg. 2017, 104, 1050.e13–1050.e18. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alexandre, A.M.; Romi, A.; Gaudino, S.; Gessi, M.; Frassanito, P.; Camilli, A.; Luca, S.; Pedicelli, A. Giant Congenital Hemangioma of the Skull: Prenatal Diagnosis and Multimodal Endovascular and Surgical Management. Medicina 2024, 60, 145. https://doi.org/10.3390/medicina60010145
Alexandre AM, Romi A, Gaudino S, Gessi M, Frassanito P, Camilli A, Luca S, Pedicelli A. Giant Congenital Hemangioma of the Skull: Prenatal Diagnosis and Multimodal Endovascular and Surgical Management. Medicina. 2024; 60(1):145. https://doi.org/10.3390/medicina60010145
Chicago/Turabian StyleAlexandre, Andrea M., Andrea Romi, Simona Gaudino, Marco Gessi, Paolo Frassanito, Arianna Camilli, Scarcia Luca, and Alessandro Pedicelli. 2024. "Giant Congenital Hemangioma of the Skull: Prenatal Diagnosis and Multimodal Endovascular and Surgical Management" Medicina 60, no. 1: 145. https://doi.org/10.3390/medicina60010145