
Age-Related Response to Remimazolam among Older Patients Undergoing Orthopedic Surgery: A Single-Center Prospective Observational Study

Abstract
1. Introduction
2. Methods
2.1. Ethical Considerations
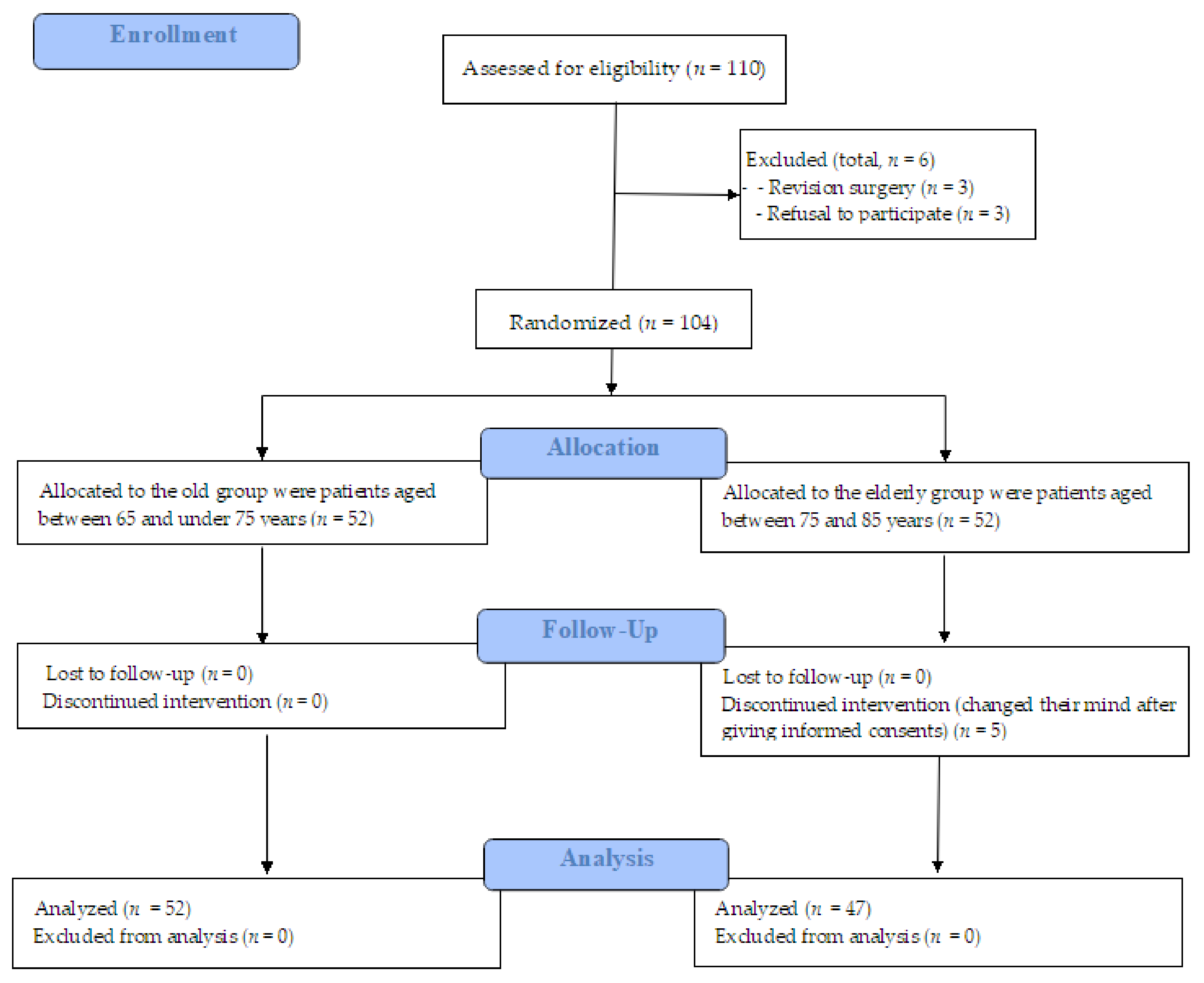
2.2. Study Population
2.3. Study Protocol
2.4. Anesthetic Methods
2.5. Clinical Variables
2.5.1. Primary Outcome
2.5.2. Secondary Outcomes
2.6. Statistical Analyses and Sample Size
3. Results
3.1. Demographic Characteristics
3.1.1. Preoperative Characteristics
3.1.2. Intraoperative Variables
3.1.3. Postoperative Variables
3.2. Remimazolam-Related Perioperative Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kumar Das, D.; Shafer, S.L. Remimazolam in Focus: Enhancing Anesthesia, Managing Risks. ASA Monit. 2024, 88, 1–5. [Google Scholar] [CrossRef]
- Wiltshire, H.R.; Kilpatrick, G.J.; Tilbrook, G.S.; Borkett, K.M. A placebo- and midazolam-controlled phase I single ascending-dose study evaluating the safety, pharmacokinetics, and pharmacodynamics of remimazolam (CNS 7056): Part II. Population pharmacokinetic and pharmacodynamic modeling and simulation. Anesth. Analg. 2012, 115, 284–296. [Google Scholar] [CrossRef] [PubMed]
- Duan, J.; Ju, X.; Wang, X.; Liu, N.; Xu, S.; Wang, S. Effects of Remimazolam and Propofol on Emergence Agitation in Elderly Patients Undergoing Hip Replacement: A Clinical, Randomized, Controlled Study. Drug Des. Dev. Ther. 2023, 17, 2669–2678. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.K.; Jang, Y.; Park, S.J. Comparison of remimazolam and propofol induction on hemodynamic response in hypertensive patients. Medicine 2023, 102, e34358. [Google Scholar] [CrossRef] [PubMed]
- Deng, W.; Zeng, Z.; Liu, Q.; Deng, J.; Wang, L.; Li, H.; Zhang, Y. Effects of Propofol, Low and High Doses of Remimazolam on Hemodynamic and Inflammatory Response in Laparoscopic Surgery. Drug Des. Dev. Ther. 2024, 18, 3329–3336. [Google Scholar] [CrossRef]
- Katsuragawa, T.; Mimuro, S.; Sato, T.; Aoki, Y.; Doi, M.; Katoh, T.; Nakajima, Y. Effect of remimazolam versus sevoflurane on intraoperative hemodynamics in noncardiac surgery: A retrospective observational study using propensity score matching. JA Clin. Rep. 2023, 9, 70. [Google Scholar] [CrossRef]
- Lee, B.; Kim, M.H.; Kong, H.J.; Shin, H.J.; Yang, S.; Kim, N.Y.; Chae, D. Effects of Remimazolam vs. Sevoflurane Anesthesia on Intraoperative Hemodynamics in Patients with Gastric Cancer Undergoing Robotic Gastrectomy: A Propensity Score-Matched Analysis. J. Clin. Med. 2022, 11, 2643. [Google Scholar] [CrossRef]
- Takaki, R.; Yokose, M.; Mihara, T.; Saigusa, Y.; Tanaka, H.; Yamamoto, N.; Masui, K.; Goto, T. Hypotension after general anaesthesia induction using remimazolam or propofol in geriatric patients undergoing sevoflurane anaesthesia with remifentanil: A single-centre, double-blind, randomised controlled trial. Br. J. Anaesth. 2024, 133, 24–32. [Google Scholar] [CrossRef]
- Vellinga, R.; Koomen, J.V.; Eleveld, D.J.; Stöhr, T.; Pesic, M.; Struys, M.; Colin, P.J. Target-controlled Infusion of Remimazolam in Healthy Volunteers Shows Some Acute Tolerance. Anesthesiology 2024, 140, 207–219. [Google Scholar] [CrossRef]
- Nakayama, J.; Ogihara, T.; Yajima, R.; Innami, Y.; Ouchi, T. Anesthetic management of super-elderly patients with remimazolam: A report of two cases. JA Clin. Rep. 2021, 7, 71. [Google Scholar] [CrossRef]
- Lee, M.; Lee, C.; Choi, G.J.; Kang, H. Remimazolam for Procedural Sedation in Older Patients: A Systematic Review and Meta-Analysis with Trial Sequential Analysis. J. Pers. Med. 2024, 14, 276. [Google Scholar] [CrossRef] [PubMed]
- Ahmer, W.; Imtiaz, S.; Alam, D.M.; Ahmed, K.; Sajid, B.; Yousuf, J.; Asnani, S.; Fahim, M.A.A.; Ali, R.; Mansoor, M.; et al. Remimazolam versus propofol for sedation in gastrointestinal endoscopy and colonoscopy within elderly patients: A meta-analysis of randomized controlled trials. Eur. J. Clin. Pharmacol. 2024, 80, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Lu, K.; Wei, S.; Ling, W.; Wei, Y.; Ran, X.; Huang, H.; Wang, M.; Wei, N.; Liao, Y.; Qin, Z.; et al. Remimazolam versus propofol for deep sedation/anaesthesia in upper gastrointestinal endoscopy in elderly patients: A multicenter, randomized controlled trial. J. Clin. Pharm. Ther. 2022, 47, 2230–2236. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.B.; Oh, J.H.; Park, J.H.; Choi, S.P.; Wee, J.H. Differences in youngest-old, middle-old, and oldest-old patients who visit the emergency department. Clin. Exp. Emerg. Med. 2018, 5, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Keam, S.J. Remimazolam: First Approval. Drugs 2020, 80, 625–633. [Google Scholar] [CrossRef]
- Hu, Q.; Liu, X.; Wen, C.; Li, D.; Lei, X. Remimazolam: An Updated Review of a New Sedative and Anaesthetic. Drug Des. Dev. Ther. 2022, 16, 3957–3974. [Google Scholar] [CrossRef]
- Furuta, M.; Ito, H.; Yamazaki, M. Anaesthetic management using remimazolam in a patient with severe aortic stenosis: A case report. BMC Anesthesiol. 2021, 21, 202. [Google Scholar] [CrossRef]
- Doi, M.; Hirata, N.; Suzuki, T.; Morisaki, H.; Morimatsu, H.; Sakamoto, A. Safety and efficacy of remimazolam in induction and maintenance of general anesthesia in high-risk surgical patients (ASA Class III): Results of a multicenter, randomized, double-blind, parallel-group comparative trial. J. Anesth. 2020, 34, 491–501. [Google Scholar] [CrossRef]
- Rex, D.K.; Bhandari, R.; Lorch, D.G.; Meyers, M.; Schippers, F.; Bernstein, D. Safety and efficacy of remimazolam in high risk colonoscopy: A randomized trial. Dig. Liver Dis. 2021, 53, 94–101. [Google Scholar] [CrossRef]
- Jeong, H.; Kim, H.; Ahn, H.J. An Adequate Infusion Rate of Remimazolam for Induction of General Anesthesia in Adult Patients: A Prospective Up-and-Down Dose-Finding Study. J. Clin. Med. 2023, 12, 1763. [Google Scholar] [CrossRef]
- Yokose, M.; Takaki, R.; Mihara, T.; Saigusa, Y.; Yamamoto, N.; Masui, K.; Goto, T. Hypotension after general anesthesia induction using remimazolam in geriatric patients: Protocol for a double-blind randomized controlled trial. PLoS ONE 2022, 17, e0275451. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Jiang, K.; Shi, W.; Xiao, S.; Zhang, S.; Zhang, Y.; Zhou, Y.; Tan, C.; Tan, S.; Zou, X. Effect of Remimazolam Tosilate on Respiratory Depression in Elderly Patients Undergoing Gastroscopy: A Multicentered, Prospective, and Randomized Study. Drug Des. Dev. Ther. 2022, 16, 4151–4159. [Google Scholar] [CrossRef] [PubMed]
- Xin, Z.; Wang, N.; Wang, H. Remimazolam and Remifentanil Use Induced Severe Respiratory Depression and Laryngeal Spasm During Intravenous Sedation and Analgesia: A Case Report. Curr. Drug Saf. 2024, 19, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, T.; Sento, Y.; Kamimura, Y.; Tsuji, T.; Kako, E.; Sobue, K. Remimazolam for induction of anesthesia in elderly patients with severe aortic stenosis: A prospective, observational pilot study. BMC Anesthesiol. 2021, 21, 306. [Google Scholar] [CrossRef] [PubMed]
- Ling, L.; Yang, T.X.; Lee, S.W.K. Effect of Anaesthesia Depth on Postoperative Delirium and Postoperative Cognitive Dysfunction in High-Risk Patients: A Systematic Review and Meta-Analysis. Cureus 2022, 14, e30120. [Google Scholar] [CrossRef]
- Pérez-Otal, B.; Aragón-Benedí, C.; Pascual-Bellosta, A.; Ortega-Lucea, S.; Martínez-Ubieto, J.; Ramírez-Rodríguez, J.M. Neuromonitoring depth of anesthesia and its association with postoperative delirium. Sci. Rep. 2022, 12, 12703. [Google Scholar] [CrossRef]
- Evered, L.A.; Chan, M.T.V.; Han, R.; Chu, M.H.M.; Cheng, B.P.; Scott, D.A.; Pryor, K.O.; Sessler, D.I.; Veselis, R.; Frampton, C.; et al. Anaesthetic depth and delirium after major surgery: A randomised clinical trial. Br. J. Anaesth. 2021, 127, 704–712. [Google Scholar] [CrossRef]
- Shimamoto, Y.; Sanuki, M.; Kurita, S.; Ueki, M.; Kuwahara, Y.; Matsumoto, A. Factors affecting prolonged time to extubation in patients given remimazolam. PLoS ONE 2022, 17, e0268568. [Google Scholar] [CrossRef]
- Liao, Y.Q.; Min, J.; Wu, Z.X.; Hu, Z. Comparison of the effects of remimazolam and dexmedetomidine on early postoperative cognitive function in elderly patients with gastric cancer. Front. Aging Neurosci. 2023, 15, 1123089. [Google Scholar] [CrossRef]
- Yang, J.J.; Lei, L.; Qiu, D.; Chen, S.; Xing, L.K.; Zhao, J.W.; Mao, Y.Y.; Yang, J.J. Effect of Remimazolam on Postoperative Delirium in Older Adult Patients Undergoing Orthopedic Surgery: A Prospective Randomized Controlled Clinical Trial. Drug Des. Dev. Ther. 2023, 17, 143–153. [Google Scholar] [CrossRef]
- Aoki, Y.; Kurita, T.; Nakajima, M.; Imai, R.; Suzuki, Y.; Makino, H.; Kinoshita, H.; Doi, M.; Nakajima, Y. Association between remimazolam and postoperative delirium in older adults undergoing elective cardiovascular surgery: A prospective cohort study. J. Anesth. 2023, 37, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Li, H.X.; Li, B.L.; Wang, T.H.; Xu, X.; Wang, F.; Zhang, X.; Zhang, X.; Li, H.Y.; Mu, B.; Sun, Y.L.; et al. Comparison of the effects of remimazolam tosylate and propofol on postoperative delirium among older adults undergoing major non-cardiac surgery: Protocol for a randomised controlled trial. BMJ Open 2023, 13, e071912. [Google Scholar] [CrossRef] [PubMed]
- Song, J.C.; Wang, X.X.; Fu, X.; Chen, W.; Tang, S.H.; Deng, F.; Yang, H.; Liu, W. Relationship between age and remimazolam dose required for inducing loss of consciousness in older surgical patients. Front. Med. 2024, 11, 1331103. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Group | Old Group | Elderly Group | p-Value |
|---|---|---|---|
| n | 52 | 47 | |
| Preoperative variables | |||
| Age (years) | 68.8 ± 3.3 | 78.1 ± 3.0 | <0.001 |
| Sex | 0.666 | ||
| Male | 2 (3.8%) | 3 (6.4%) | |
| Female | 50 (96.2%) | 44 (93.6%) | |
| ASA physical class | 0.244 | ||
| I | 3 (5.8%) | 0 (0.0%) | |
| II | 49 (94.2%) | 47 (100.0%) | |
| Body mass index (kg/m2) | 25.2 ± 3.8 | 24.5 ± 2.5 | 0.288 |
| Height (m) | 1.6 ± 0.1 | 1.5 ± 0.1 | 0.332 |
| Weight (kg) | 61.4 ± 9.2 | 58.9 ± 7.0 | 0.145 |
| Intraoperative variables | |||
| Operation duration (min) | 79.9 ± 22.4 | 74.4 ± 12.9 | 0.131 |
| Anesthesia duration (min) | 112.0 ± 23.8 | 107.2 ± 16.2 | 0.25 |
| Tourniquet time (min) | 47.2 ± 14.6 | 48.6 ± 15.4 | 0.647 |
| Remifentanil | |||
| Total dosage (mg) | 0.5 ± 0.2 | 0.4 ± 0.2 | 0.177 |
| Postoperative variables | |||
| Total PCA infusion (mL) | 48.0 ± 21.6 | 47.8 ± 25.6 | 0.973 |
| Group | Old Group | Elderly Group | p-Value |
|---|---|---|---|
| n | 52 | 47 | |
| Intraoperative remimazolam | |||
| Infusion rate (ug/kg/min) | 23.0 ± 5.3 | 21.5 ± 5.5 | 0.2 |
| Total infusion time (min) | 101.0 ± 22.7 | 93.4 ± 17.5 | 0.054 |
| Primary outcome | |||
| flumazenil required in the OR | 13 (25.0%) | 18 (38.3%) | 0.154 |
| Secondary outcomes | |||
| 1. Induction of general anesthesia | |||
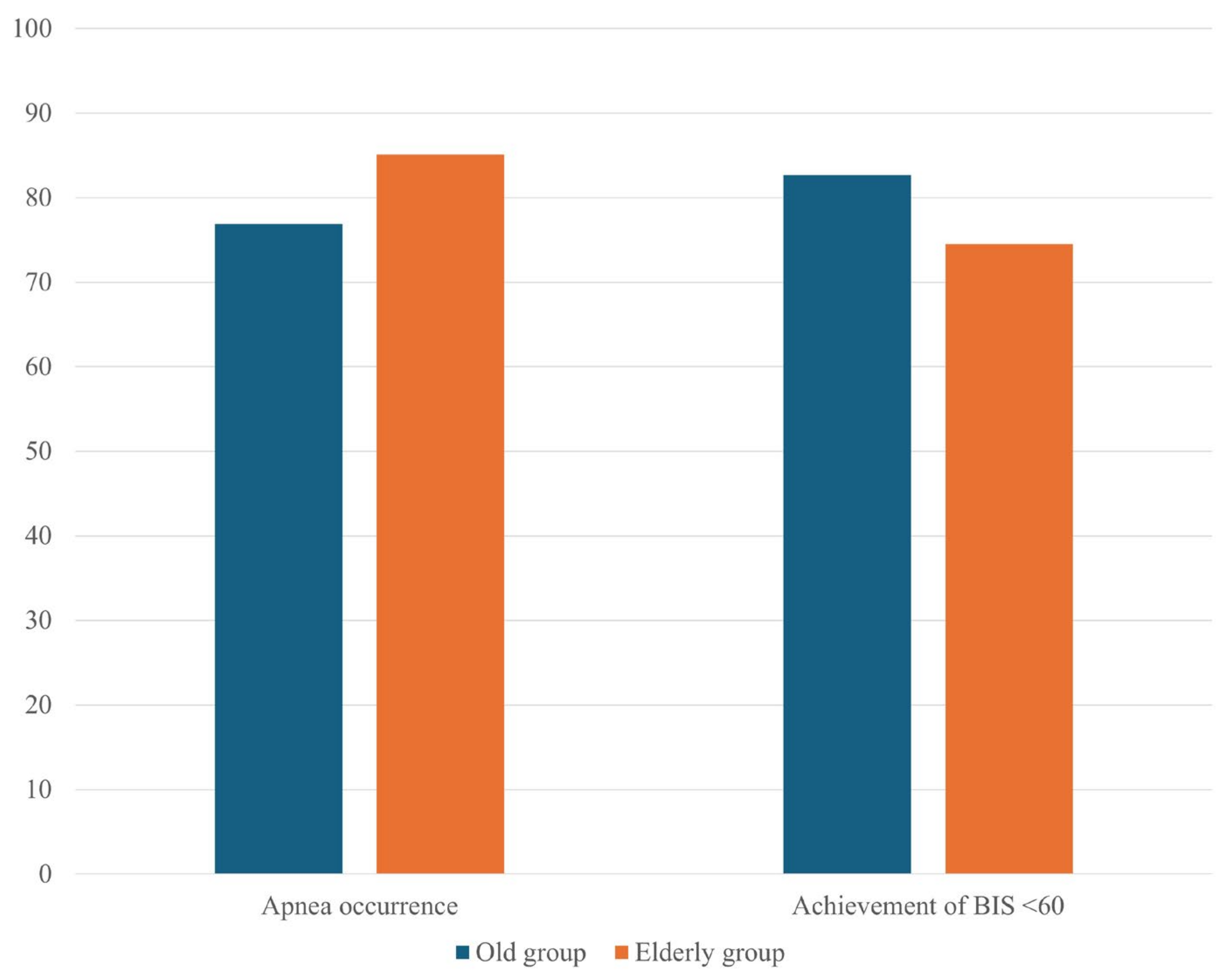
| Apnea occurrence | 40 (76.9%) | 40 (85.1%) | 0.302 |
| Time to apnea onset (s) | 99.8 ± 14.0 | 100.2 ± 19.9 | 0.923 |
| Achievement of BIS < 60 | 43 (82.7%) | 35 (74.5%) | 0.318 |
| Time to BIS < 60 (s) | 316.3 ± 486.5 | 358.8 ± 469.8 | 0.698 |
| 2. Awake variables in general anesthesia | |||
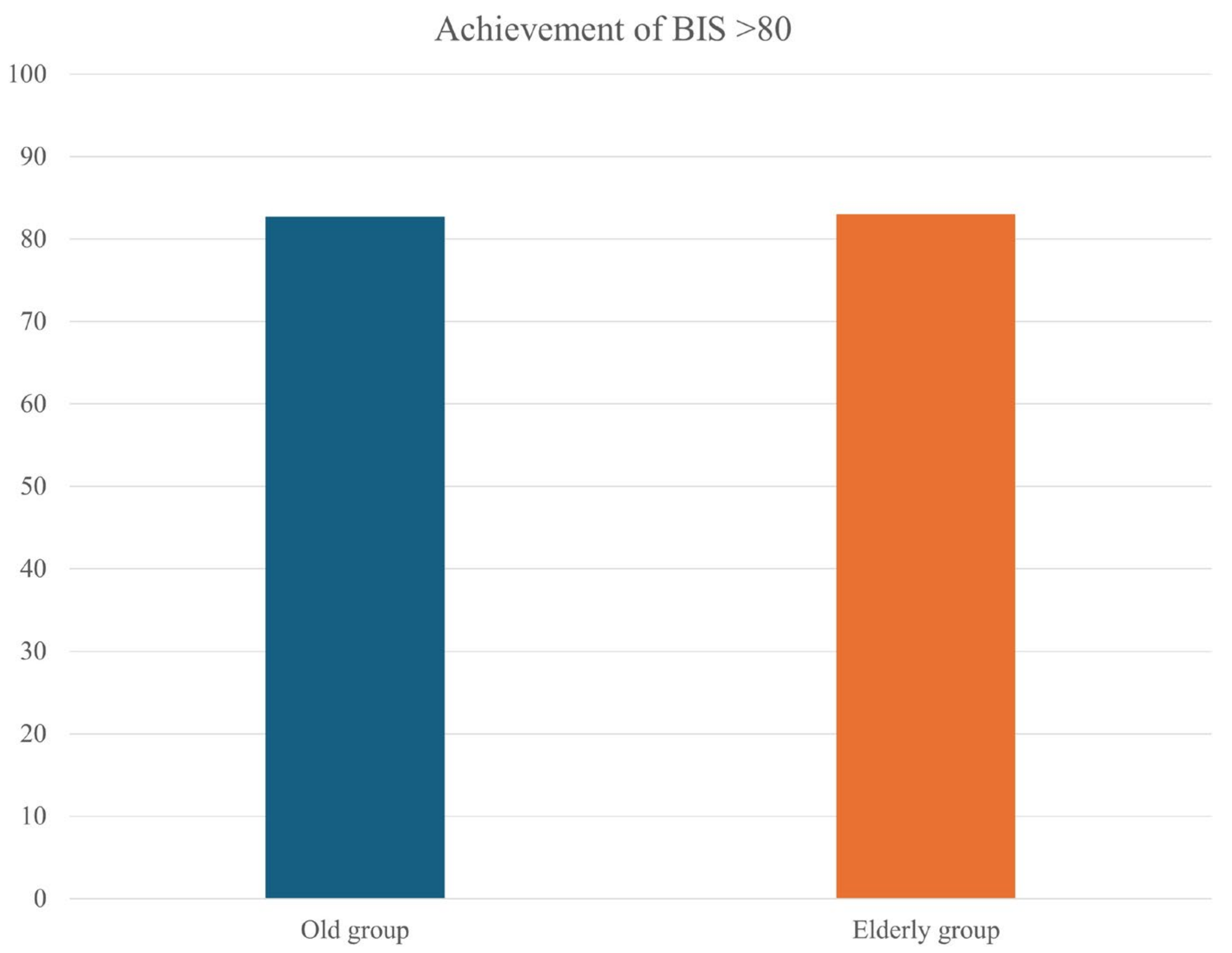
| Achievement of BIS > 80 | 43 (82.7%) | 39 (83.0%) | 0.97 |
| Time to BIS > 80 (s) | 277.7 ± 234.2 | 267.7 ± 214.9 | 0.842 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chae, M.S.; Lee, N.; Koh, H.J. Age-Related Response to Remimazolam among Older Patients Undergoing Orthopedic Surgery: A Single-Center Prospective Observational Study. Medicina 2024, 60, 1616. https://doi.org/10.3390/medicina60101616
Chae MS, Lee N, Koh HJ. Age-Related Response to Remimazolam among Older Patients Undergoing Orthopedic Surgery: A Single-Center Prospective Observational Study. Medicina. 2024; 60(10):1616. https://doi.org/10.3390/medicina60101616
Chicago/Turabian StyleChae, Min Suk, Nuri Lee, and Hyun Jung Koh. 2024. "Age-Related Response to Remimazolam among Older Patients Undergoing Orthopedic Surgery: A Single-Center Prospective Observational Study" Medicina 60, no. 10: 1616. https://doi.org/10.3390/medicina60101616
APA StyleChae, M. S., Lee, N., & Koh, H. J. (2024). Age-Related Response to Remimazolam among Older Patients Undergoing Orthopedic Surgery: A Single-Center Prospective Observational Study. Medicina, 60(10), 1616. https://doi.org/10.3390/medicina60101616