
The Early Hematological Profile and Its Variations: A Useful Tool in the Prediction of Intraventricular Hemorrhage in Extremely Preterm Infants

 , ,
, ,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group: Inclusion and Exclusion Criteria
2.2. Data Collection
2.3. Clinical Suspicion of IVH
2.4. Cranial Ultrasound (CUS)
2.5. Blood Sample Collection (Laboratory Data)
2.5.1. Blood Gases
2.5.2. Complete Blood Count
2.6. Ethics Approval
2.7. Statistical Analysis
3. Results
3.1. Blood Gases at Birth
3.2. Red Blood Cell Lineage
- Comparison between EP infants without IVH and those with IVH, irrespective of severity
- Comparison between preterm infants with mild IVH and those with severe IVH
3.3. White Blood Cell Lineage
3.4. Platelet Lineage
3.5. Univariate Analysis for AUC Evaluation of Hematological Parameters and Other Neonatal Factors Associated with IVH Risk in Extremely Preterm Infants
3.6. Multivariate Analysis to Evaluate the Chance of IVH Occurrence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rocha, G.; Pereira, S.; Antunes-Sarmento, J.; Flôr-de-Lima, F.; Soares, H.; Guimarães, H. Early anemia and neonatal morbidity in extremely low birth-weight preterm infants. J. Matern. Fetal Neonatal Med. 2021, 34, 3697–3703. [Google Scholar] [CrossRef] [PubMed]
- Howarth, C.; Banerjee, J.; Aladangady, N. Red Blood Cell Transfusion in Preterm Infants: Current Evidence and Controversies. Neonatology 2018, 114, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Reduction of Infection in Chinese Neonatal Intensive Care Units Using the Evidence-based Practice for Improving Quality Study Group. Incidence and risk factors of severe intraventricular hemorrhage in very low and extremely low birth weight infants: A multi-center study. Zhonghua Er Ke Za Zhi 2019, 57, 258–264. [Google Scholar]
- Mukerji, A.; Shah, V.; Shah, P.S. Periventricular/intraventricular hemorrhage and neurodevelopmental outcomes: A meta-analysis. Pediatrics 2015, 136, 1132–1143. [Google Scholar] [CrossRef] [PubMed]
- Pascal, A.; Govaert, P.; Oostra, A.; Naulaers, G.; Ortibus, E.; Van den Broeck, C. Neurodevelopmental outcome in very preterm and very-low-birthweight infants born over the past decade: A meta-analytic review. Dev. Med. Child. Neurol. 2018, 60, 342–355. [Google Scholar] [CrossRef] [PubMed]
- Szpecht, D.; Nowak, I.; Kwiatkowska, P.; Szymankiewicz, M.; Gadzinowski, J. Intraventricular hemorrhage in neonates born from 23 to 26 weeks of gestation: Retrospective analysis of risk factors. Adv. Clin. Exp. Med. 2017, 26, 89–94. [Google Scholar] [CrossRef]
- Park, Y.S. Perspectives: Understanding the Pathophysiology of Intraventricular Hemorrhage in Preterm Infants and Considering of the Future Direction for Treatment. J. Korean Neurosurg. Soc. 2023, 66, 298–307. [Google Scholar] [CrossRef]
- Christensen, R.D.; Del Vecchio, A.; Henry, E. Expected erythrocyte, platelet and neutrophil values for term and preterm neonates. J. Matern. Fetal Neonatal Med. 2012, 25 (Suppl. S5), 77–79. [Google Scholar] [CrossRef]
- Christensen, R.D.; Henry, E.; Jopling, J.; Wiedmeier, S.E. The CBC: Reference ranges for neonates. Semin. Perinatol. 2009, 33, 3–11. [Google Scholar] [CrossRef]
- Henry, E.; Christensen, R.D. Reference Intervals in Neonatal Hematology. Clin. Perinatol. 2015, 42, 483–497. [Google Scholar] [CrossRef]
- Roudil, P.; Vasselon, C.; Trombert-Paviot, B.; Berger, C.; Patural, H. Blood parameters of preterm neonates: Postnatal evolution according to gestational age. Int. J. Lab. Hematol. 2017, 39, 317–328. [Google Scholar] [CrossRef]
- Karagol, B.S.; Calisici, E.; Zeybek, C.; Unay, B.; Yuksel, S. The impact of initial hematocrit values after birth on peri-/intraventricular hemorrhage in extremely low birth weight neonates. Childs Nerv. Syst. 2022, 38, 109–114. [Google Scholar] [CrossRef]
- Dekom, S.; Vachhani, A.; Patel, K.; Barton, L.; Ramanathan, R.; Noori, S. Initial hematocrit values after birth and peri/intraventricular hemorrhage in extremely low birth weight infants. J. Perinatol. 2018, 38, 1471–1475. [Google Scholar] [CrossRef] [PubMed]
- Meyer, M.P.; O’Connor, K.L.; Meyer, J.H. Thresholds for blood transfusion in extremely preterm infants: A review of the latest evidence from two large clinical trials. Front. Pediatr. 2022, 10, 957585. [Google Scholar] [CrossRef] [PubMed]
- Bell, E.F. Red cell transfusion thresholds for preterm infants: Finally some answers. Arch. Dis. Child. Fetal Neonatal Ed. 2022, 107, 126–130. [Google Scholar] [CrossRef]
- Hemmati, F.; Sharma, D.; Namavar Jahromi, B.; Salarian, L.; Farahbakhsh, N. Delayed cord clamping for prevention of intraventricular hemorrhage in preterm neonates: A randomized control trial. J. Matern. Fetal Neonatal Med. 2022, 35, 3633–3639. [Google Scholar] [CrossRef] [PubMed]
- Ballard, J.L.; Khoury, J.C.; Wedig, K.; Wang, L.; Eilers-Walsman, B.L.; Lipp, R. New Ballard Score, expanded to include extremely premature infants. J. Pediatr. 1991, 119, 417–423. [Google Scholar] [CrossRef]
- Parodi, A.; Govaert, P.; Horsch, S.; Bravo, M.C.; Ramenghi, L.A.; eurUS.brain Group. Cranial ultrasound findings in preterm germinal matrix haemorrhage, sequelae, and outcome. Pediatr. Res. 2020, 87 (Suppl. S1), 13–24. [Google Scholar] [CrossRef]
- Papile, L.A.; Burstein, J.; Burstein, R.; Koffler, H. Incidence and evolution of subependymal and intraventricular hemorrhage: A study of infants with birth weights less than 1500 gm. J. Pediatr. 1978, 92, 529–534. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, A.; Conte, M.; Scarafile, R.; Riegler, L.; Cocchia, R.; Pezzullo, E.; Cavallaro, M.; Carbone, A.; Natale, F.; Russo, M.G.; et al. Transcranial Doppler ultrasound: Physical principles and principal applications in neurocritical care unit. J. Cardiovasc. Echogr. 2016, 26, 28–41. [Google Scholar] [CrossRef]
- Mohammad, K.; Scott, J.N.; Leijser, L.M.; Zein, H.; Afifi, J.; Piedboeuf, B.; de Vries, L.S.; van Wezel-Meijler, G.; Lee, S.K.; Shah, P.S. Consensus Approach for Standardizing the Screening and Classification of Preterm Brain Injury Diagnosed with Cranial Ultrasound: A Canadian Perspective. Front. Pediatr. 2021, 9, 618236. [Google Scholar] [CrossRef] [PubMed]
- Räisänen, S.; Gissler, M.; Saari, J.; Kramer, M.; Heinonen, S. Contribution of risk factors to extremely, very, and moderately preterm births—Register-based analysis of 1,390,742 singleton births. PLoS ONE 2013, 8, e60660. [Google Scholar] [CrossRef] [PubMed]
- Siffel, C.; Kistler, K.; Sarda, S. Global incidence of intraventricular hemorrhage among extremely preterm infants: A systematic literature review. J. Perinat. Med. 2021, 49, 1017–1026. [Google Scholar] [CrossRef] [PubMed]
- Morgan, A.S.; Mendonça, M.; Thiele, N.; David, A.L. Management and outcomes of extreme preterm birth. BMJ 2022, 376, e055924. [Google Scholar] [CrossRef] [PubMed]
- Bell, E.F.; Hintz, S.R.; Hansen, N.I.; Bann, C.M.; Wyckoff, M.H.; DeMauro, S.B.; Walsh, M.C.; Vohr, B.R.; Stoll, B.J.; Carlo, W.A.; et al. Mortality, In-Hospital Morbidity, Care Practices, and 2-Year Outcomes for Extremely Preterm Infants in the US, 2013–2018. JAMA 2022, 327, 248–263. [Google Scholar] [CrossRef] [PubMed]
- Su, B.H.; Hsieh, W.S.; Hsu, C.H.; Chang, J.H.; Lien, R.; Lin, C.H.; Premature Baby Foundation of Taiwan (PBFT). Neonatal outcomes of extremely preterm infants from taiwan: Comparison with Canada, Japan, and the USA. Pediatr. Neonatol. 2015, 56, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Yuan, L.; Wang, J.; Li, Q.; Yang, C.; Gao, X.; Chen, S.; Han, S.; Liu, J.; Wu, H.; et al. Mortality and Morbidity of Infants Born Extremely Preterm at Tertiary Medical Centers in China From 2010 to 2019. JAMA Netw. Open 2021, 4, e219382. [Google Scholar] [CrossRef] [PubMed]
- Hosono, S.; Mugishima, H.; Kitamura, T.; Inami, I.; Fujita, H.; Hosono, A.; Minato, M.; Okada, T.; Takahashi, S.; Harada, K. Effect of hemoglobin on transfusion and neonatal adaptation in extremely low-birthweight infants. Pediatr. Int. 2008, 50, 306–311. [Google Scholar] [CrossRef]
- Fogarty, M.; Osborn, D.A.; Askie, L.; Seidler, A.L.; Hunter, K.; Lui, K.; Simes, J.; Tarnow-Mordi, W. Delayed vs early umbilical cord clamping for preterm infants: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2018, 218, 1–18. [Google Scholar] [CrossRef]
- Strauss, R.G.; Mock, D.M.; Johnson, K.J.; Cress, G.A.; Burmeister, L.F.; Zimmerman, M.B.; Bell, E.F.; Rijhsinghani, A. A randomized clinical trial comparing immediate versus delayed clamping of the umblical cord in preterm infants: Short-term clinical and laboratory endpoints. Transfusion 2008, 48, 658–665. [Google Scholar] [CrossRef]
- Aboalqez, A.; Deindl, P.; Ebenebe, C.U.; Singer, D.; Blohm, M.E. Iatrogenic Blood Loss in Very Low Birth Weight Infants and Transfusion of Packed Red Blood Cells in a Tertiary Care Neonatal Intensive Care Unit. Children 2021, 8, 847. [Google Scholar] [CrossRef]
- Scholkmann, F.; Ostojic, D.; Isler, H.; Bassler, D.; Wolf, M.; Karen, T. Reference Ranges for Hemoglobin and Hematocrit Levels in Neonates as a Function of Gestational Age (22–42 Weeks) and Postnatal Age (0–29 Days): Mathematical Modeling. Children 2019, 6, 38. [Google Scholar] [CrossRef] [PubMed]
- Jopling, J.; Henry, E.; Wiedmeier, S.E.; Christensen, R.D. Reference ranges for hematocrit and blood hemoglobin concentration during the neonatal period: Data from a multihospital health care system. Pediatrics 2009, 123, e333–e337. [Google Scholar] [CrossRef] [PubMed]
- Esan, A.J. Hematological differences in newborn and aging: A review study. Hematol. Transfus. Int. J. 2016, 3, 178–190. [Google Scholar]
- Christensen, R.D.; Jopling, J.; Henry, E.; Wiedmeier, S.E. The erythrocyte indices of neonates defined using data from over 12,000 patients in a multihospital health care system. J. Perinatol. 2008, 28, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Nunes, M.F.; Oliveira, A.M.; Conceicao, S.M.; Medrado, F.E. Erythrocyte Indices and Serum Ferritin in Newborns. Braz. J. Hematol. Hemother. 2010, 32, 365–370. [Google Scholar] [CrossRef]
- Putbrese, B.; Kennedy, A. Findings and differential diagnosis of fetal intracranial haemorrhage and fetal ischaemic brain injury: What is the role of fetal MRI? Br. J. Radiol. 2017, 90, 20160253. [Google Scholar] [CrossRef] [PubMed]
- Gilard, V.; Tebani, A.; Bekri, S.; Marret, S. Intraventricular Hemorrhage in Very Preterm Infants: A Comprehensive Review. J. Clin. Med. 2020, 9, 2447. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Fernandez, J.; Ochoa, J.J.; Latunde-Dada, G.O.; Diaz-Castro, J. Iron Deficiency and Iron Homeostasis in Low Birth Weight Preterm Infants: A Systematic Review. Nutrients 2019, 11, 1090. [Google Scholar] [CrossRef]
- Ochoa, J.J.; Contreras-Chova, F.; Muñoz, S.; Araujo-Nepomuceno, E.; Bonillo, A.; Molina-Carballo, A.; Muñoz-Hoyos, A. Fluidity and oxidative stress in erythrocytes from very low birth weight infants during their first 7 days of life. Free Radic. Res. 2007, 41, 1035–1040. [Google Scholar] [CrossRef]
- Cavaliere, T. Red blood cell indices: Implications for practice. Newborn Infant Nurs. Rev. 2004, 4, 231–239. [Google Scholar] [CrossRef]
- Elmoneim, A.A.; Zolaly, M.; El-Moneim, E.A.; Sultan, E. Prognostic significance of early platelet count decline in preterm newborns. Indian. J. Crit. Care Med. 2015, 19, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, S.; Olmez, I.; Bhutada, A.; Rastogi, D. Drop in platelet counts in extremely preterm neonates and its association with clinical outcomes. J. Pediatr. Hematol. Oncol. 2011, 33, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Go, H.; Ohto, H.; Nollet, K.E.; Takano, S.; Kashiwabara, N.; Chishiki, M.; Maeda, H.; Imamura, T.; Kawasaki, Y.; Momoi, N.; et al. Using Platelet Parameters to Anticipate Morbidity and Mortality Among Preterm Neonates: A Retrospective Study. Front. Pediatr. 2020, 8, 90. [Google Scholar] [CrossRef] [PubMed]
- Cekmez, F.; Tanju, I.A.; Canpolat, F.E.; Aydinoz, S.; Aydemir, G.; Karademir, F.; Sarici, S.U. Mean platelet volume in very preterm infants: A predictor of morbidities? Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.C.; Catalano, R.; Profit, J.; Gould, J.B.; Lee, H.C. Impact of antenatal steroids on intraventricular hemorrhage in very-low-birth weight infants. J. Perinatol. 2016, 36, 352e6. [Google Scholar] [CrossRef] [PubMed]
- Gamaleldin, I.; Harding, D.; Siassakos, D.; Draycott, T.; Odd, D. Significant intraventricular hemorrhage is more likely in very preterm infants born by vaginal delivery: A multi-centre retrospective cohort study. J. Matern. Fetal Neonatal Med. 2019, 32, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Humberg, A.; Härtel, C.; Paul, P.; Hanke, K.; Bossung, V.; Hartz, A.; Fasel, L.; Rausch, T.K.; Rody, A.; Herting, E.; et al. Delivery mode and intraventricular hemorrhage risk in very-low-birth-weight infants: Observational data of the German Neonatal Network. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 212, 144–149. [Google Scholar] [CrossRef] [PubMed]
- da Costa, C.S.; Czosnyka, M.; Smielewski, P.; Austin, T. Optimal mean arterial blood pressure in extremely preterm infants within the first 24 hours of life. J. Pediatr. 2018, 203, 242–248. [Google Scholar] [CrossRef]
- Eriksen, V.R.; Hahn, G.H.; Greisen, G. Dopamine therapy is associated with impaired cerebral autoregulation in preterm infants. Acta Paediatr. 2014, 103, 1221e6. [Google Scholar] [CrossRef]
- Sankaran, J.; Brandsma, E.; Kushnir, A. Effect of administration of normal saline bolus on intraventricular hemorrhage in preterm neonates. Pediatrics 2018, 14, 517. [Google Scholar] [CrossRef]
- Farag, M.M.; Gouda, M.H.; Almohsen, A.M.A.; Khalifa, M.A. Intraventricular hemorrhage prediction in premature neonates in the era of hemodynamics monitoring: A prospective cohort study. Eur. J. Pediatr. 2022, 181, 4067–4077. [Google Scholar] [CrossRef]
- Depala, K.S.; Chintala, S.; Joshi, S.; Budhani, S.; Paidipelly, N.; Patel, B.; Rastogi, A.; Madas, N.; Vejju, R.; Mydam, J. Clinical Variables Associated with Grade III and IV Intraventricular Hemorrhage (IVH) in Preterm Infants Weighing Less Than 750 Grams. Cureus 2023, 15, e40471. [Google Scholar] [CrossRef]
- Al-Mouqdad, M.M.; Abdelrahim, A.; Abdalgader, A.T.; Alyaseen, N.; Khalil, T.M.; Taha, M.Y.; Asfour, S.S. Risk factors for intraventricular hemorrhage in premature infants in the central region of Saudi Arabia. Int. J. Pediatr. Adolesc. Med. 2021, 8, 76–81. [Google Scholar] [CrossRef]
- Weinstein, R.M.; Parkinson, C.; Everett, A.D.; Graham, E.M.; Vaidya, D.; Northington, F.J. A predictive clinical model for moderate to severe intraventricular hemorrhage in very low birth weight infants. J. Perinatol. 2022, 42, 1374–1379. [Google Scholar] [CrossRef]
- Bersani, I.; Pluchinotta, F.; Dotta, A.; Savarese, I.; Campi, F.; Auriti, C.; Chuklantseva, N.; Piersigilli, F.; Gazzolo, F.; Varrica, A.; et al. Early predictors of perinatal brain damage: The role of neurobiomarkers. Clin. Chem. Lab. Med. 2020, 58, 471–486. [Google Scholar] [CrossRef] [PubMed]
- Berger, R.P.; Pak, B.J.; Kolesnikova, M.D.; Fromkin, J.; Saladino, R.; Herman, B.E.; Pierce, M.C.; Englert, D.; Smith, P.T.; Kochanek, P.M. Derivation and Validation of a Serum Biomarker Panel to Identify Infants with Acute Intracranial Hemorrhage. JAMA Pediatr. 2017, 171, e170429. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
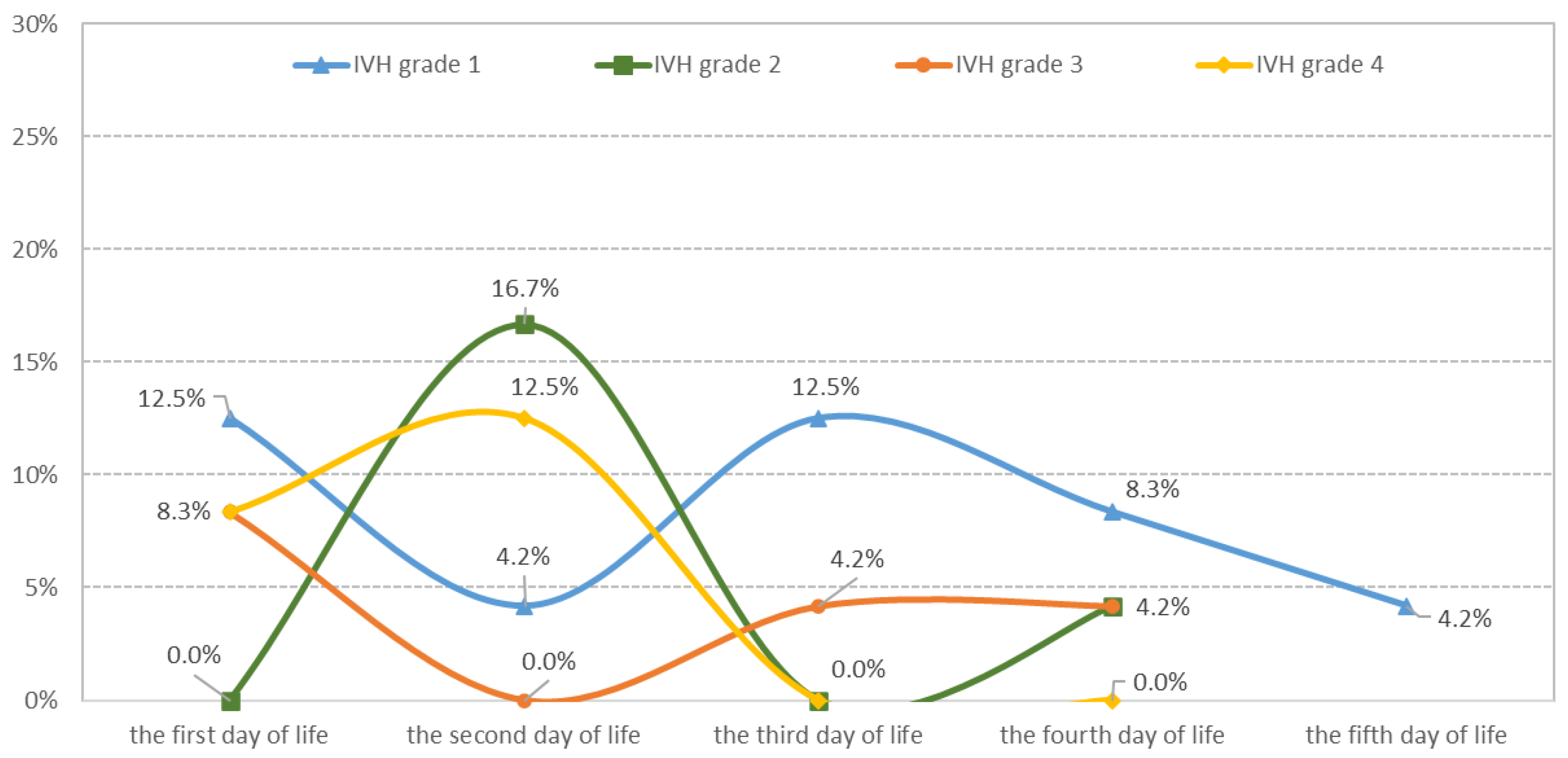
| Day of Life | Number of Cases | Percent of n = 134 (All Groups) | Percent of n = 48 (Cases with IVH) |
|---|---|---|---|
| DOL 1 | 14 | 10.45 | 29.2% |
| DOL 2 | 16 | 11.94 | 33.3% |
| DOL 3 | 8 | 5.97 | 16.7% |
| DOL 4 | 8 | 5.97 | 16.7% |
| DOL 5 | 2 | 1.50 | 4.2% |
| Without IVH | 86 | 64.18 |
| Clinical Characteristics | Control Group (without IVH) No = 86 | Study Group with IVH (All Grades) n = 48 | p-Value * | Mild IVH Subgroup (Grade 1–2) n = 30 | Severe IVH Subgroup (Grade 3–4) n = 18 | p-Value * |
|---|---|---|---|---|---|---|
| GA §, weeks, median (quartile) | 27 (25–28) | 27 (26.5–28) | 0.695 | 27 (27–28) | 27 (24–28) | 0.371 |
| BW § (g), median (quartile) | 870 (700–1000) | 835 (650–975) | 0.171 | 900 (800–980) | 800 (600–820) | 0.019 * |
| Male gender ‡, n (%) | 32 (37.2) | 30 (62.5) | 0.004 * | 20 (66.7) | 10 (55.6) | 0.441 |
| SGA ‡, n (%) | 14 (16.3) | 14 (29.2) | 0.083 | 6 (20) | 8 (44.4) | 0.073 |
| No antenatal care ‡, n (%) | 32 (37.2) | 12 (25) | 0.149 | 6 (20) | 6 (33.3) | 0.306 |
| No ACT ‡, n (%) | 38 (44.2) | 30 (62.5) | 0.041 * | 14 (46.7) | 16 (88.9) | 0.002 |
| Vaginal delivery ‡, n (%) | 44 (51.2) | 38 (79.2) | 0.001 * | 24 (80) | 14 (77.8) | 0.854 |
| IVH, n (%) | - | 48 (100) | - | - | - | - |
| grade 1 | - | 20 (41.7) | - | - | - | - |
| grade 2 | - | 10 (20.8) | - | - | - | - |
| grade 3 | - | 8 (16.7) | - | - | - | - |
| grade 4 | - | 10 (20.8) | - | - | - | - |
| Apgar 1 min §, median (quartile) | 7 (4–8) | 5 (3–7) | 0.043 * | 6 (4–8) | 5 (2–5) | 0.007 * |
| Apgar 5 min §, median (quartile) | 8 (6–8) | 7 (5–8) | 0.115 | 8 (6–9) | 5 (5–7) | 0.004 * |
| DCC ‡, n (%) | 20 (23.3) | 3 (6.3) | 0.0023 * | 3 (10) | - | - |
| PBCC ‡, n (%) | 39 (45.3) | 25 (52.1) | 0.0521 | 19 (63.3) | 6 (33.3) | 0.002 * |
| ICC ‡, n (%) | 18 (20.9) | 20 (41.7) | 0.0267 * | 8 (26.7) | 12 (66.7) | 0.001 * |
| RDS ‡, n (%) | ||||||
| mild | 10 (11.6) | 0 (0) | 0.018 * | 0 (0) | 0 (0) | 0.238 |
| moderate | 38 (44.2) | 18 (37.5) | 0.021 * | 14 (46.7) | 4 (22.2) | 0.014 * |
| severe | 38 (44.2) | 30 (62.5) | 0.003 * | 16 (53.3) | 14 (77.8) | 0.025 * |
| Surfactant ‡, n (%) | 50 (58.1) | 24 (50) | 0.363 | 12 (40) | 12 (66.7) | 0.073 |
| CPAP ‡, n (%) | 60 (69.8) | 16 (33.3) | <0.001 * | 16 (53.3) | 0 (0) | <0.001 * |
| MV ‡, n (%) | 26 (30.2) | 26 (54.2) | 0.006 * | 10 (33.3) | 16 (88.9) | <0.001 * |
| HFOV ‡, n (%) | 8 (9.3) | 12 (25) | 0.014 * | 4 (13.3) | 8 (44.4) | 0.015 * |
| Hypercapnia ‡, n (%) | 12 (13.9) | 24 (50) | <0.001 * | 8 (26.7) | 16 (88.9) | <0.001 * |
| Hypotension ‡, n (%) | 14 (16.3) | 22 (45.8) | <0.001 * | 6 (20) | 16 (88.9) | <0.001 * |
| PDA ‡, n (%) | 62 (72.1) | 30 (62.5) | 0.251 | 18 (60) | 12 (66.7) | 0.644 |
| RCT ‡, days 4–7 | - | 20 (41.7) | - | 2 (6.7) | 18 (100) | <0.001 * |
| NICU §, days, median (quartile) | 21 (12–26) | 17 (14–23) | 0.298 | 20 (14–24) | 15 (8–17) | 0.002 * |
| Days at discharge §, median (quartile) | 50 (38–65) | 36 (21–64) | 0.008 * | 52 (36–64) | 23 (8–42) | 0.011 * |
| Death ‡, n (%) | 4 (4.7) | 10 (20.8) | 0.003 | 2 (6.7) | 8 (44.4) | 0.001 * |
| Blood Gases at Birth and Hematological Parameters | Control Group (without IVH) No = 86 | Study Group with IVH (All Grades) n = 48 | p-Value | Mild IVH Subgroup (Grade 1 and 2) n = 30 | Severe IHV Subgroup (Grade 3 and 4) n = 18 | p-Value |
|---|---|---|---|---|---|---|
| At birth (cord blood gases), median (quartile) | ||||||
| pH | 7.28 (7.22–7.33) | 7.21 (7.09–7.27) | 0.0008 * | 7.26 (7.11–7.35) | 7.15 (7.07–7.20) | 0.0072 * |
| Base excess—BE, mmol/L | −4.9 (−7.5–−3.6) | −8.15 (−12.7–−5.9) | 0.0066 * | −6 (−8.3–−5.6) | −10.6 (−12.7–−9.1) | 0.0032 * |
| Lactate, mmol/L | 2.6 (1.7–3.8) | 4.7 (2.6–8.35) | 0.0003 * | 3 (2–8.1) | 5.3 (3.9–8.6) | 0.0187 * |
| Red blood cell lineage, median (quartile) | ||||||
| HGB DOL1, g/dL | 15.9 (13.9–16.5) | 14.1 (13.4–15.1) | 0.0312 * | 14.7 (13.7–15.3) | 13.1 (11.9–13.9) | 0.0524 |
| HGB DOL4, g/dL | 14.2 (12.7–14.5) | 11.7 (9.6–12.3) | <0.001 * | 12.4 (11.8–13.7) | 7.3 (8.4–9.8) | <0.001 * |
| HGB difference between DOL1 and DOL4 | 1.7 (0.9–2.8) | 2.45 (2.1–4) | <0.001 * | 2.3 (2.2–3.6) | 5.8 (2–6.5) | 0.0029 * |
| HCT DOL1, % | 51.2 (47.9–52.4) | 43.8 (40.1–47.1) | 0.0172 * | 44.5 (42.2–46.5) | 38.4 (37.1–42.6) | 0.0561 |
| HCT DOL4, % | 45.1 (40.1–43.8) | 35.2 (30.8–35.9) | <0.001 * | 36.4 (34.8–37.8) | 28.5 (25.4–29.8) | <0.001 * |
| HCT difference between DOL1 and DOL4 | 6.1 (5.9–7.3) | 8.6 (7.3–10.6) | <0.001 * | 8.1 (7.9–9.1) | 9.9 (8.9–10.2) | 0.0239 * |
| ERY DOL1, 106/ µL | 4.91 (3.82–5.34) | 3.99 (3.34–4.52) | 0.0251 * | 4.21 (3.43–4.44) | 3.84 (3.56–4.48) | 0.0586 |
| ERY DOL4, ×106/ µL | 3.97 (3.29–3.98) | 3.02 (2.67–3.41) | <0.001 * | 3.29 (2.67–3.82) | 2.73 (2.46–02.92) | 0.0093 * |
| ERY difference between DOL1 and DOL4 | 0.94 (0.72–1.18) | 0.97 (0.83–1.21) | 0.0122 * | 0.92 (0.52–1.24) | 1.11 (0.96–1.72) | 0.0216 * |
| MCV DOL1, µm3 | 112.3 (109.7–116.4) | 114.3 (108.8–118.5) | 0.3729 | 116.3 (111.2–118.5) | 110.1 (100.6–118.2) | 0.1353 |
| MCV DOL4, µm3 | 105.4 (100.8–109.1) | 102.9 (95.4–108.1) | 0.0278 * | 104.9 (94.6–108.8) | 100 (96.2–102.2) | 0.2464 |
| MCV difference between DOL1 and DOL4 | 7.5 (2.4–11.9) | 8.35 (6.05–16.25) | 0.0146 * | 8.4 (7.5–17.2) | 8.1 (4.4–15.3) | 0.3943 |
| MCH DOL1, pg | 38.6 (37–39.5) | 31.8 (36.3–40.1) | 0.1875 | 39.2 (37.9–40.5) | 35.6 (34.3–36.9) | <0.001 * |
| MCH DOL4, pg | 36.7 (34.8–40.1) | 34.2 (31.6–37.3) | <0.001 * | 35.2 (31.8–39.2) | 31.6 (30.7–33.6) | 0.0005 * |
| MCH difference between DOL1 and DOL4 | 1.4 (−2–3.2) | 3.7 (1.9–5.7) | 0.0002 * | 3.2 (−0.2–5.8) | 4 (2.5–4) | 0.7982 |
| MCHC DOL1, g/dL | 34 (33.6–34.9) | 34.1 (32.4–34.6) | 0.0717 | 34.3 (33.3–34.8) | 32.4 (32.2–34.1) | 0.0041 * |
| MCHC DOL4, g/dL | 34.8 (33.5–36.3) | 34.7 (34.1–35.3) | 0.3158 | 35.1 (34.3–35.9) | 33.9 (33.4–34.3) | 0.0001 * |
| MCHC difference between DOL1 and DOL4 | −0.3 (−2.1–0.30) | −1 (−1.9–0.1) | 0.5576 | −1 (−2–0) | −0.2 (−1.9–0.2) | 0.3272 |
| White blood cell lineage, median (quartile) | ||||||
| WBC DOL1, ×103/µL | 13.63 (10.3–22.38) | 15.09 (9.19–21.07) | 0.5713 | 17.9 (13.63–20.2) | 14.56 (6.3–21.94) | 0.2167 |
| WBC DOL4, ×103/µL | 13.26 (9.9–16.47) | 12.68 (11.4–16.9) | 0.5401 | 12.67 (9.8–16.9) | 16 (11.4–17.5) | 0.1867 |
| WBC difference between DOL1 and DOL4 | 1.5 (−2.53–5.48) | 2.16 (−2.27–6.72) | 0.5525 | 2.16 (1–7.5) | −2.94 (−5.1–4.9) | 0.0191 * |
| ANC DOL1, ×103/µL | 5.5 (2.9–9.5) | 7.4 (3.4–9.3) | 0.2536 | 7.8 (3.83–10.6) | 4.3 (3.06–8.31) | 0.0152 * |
| ANC DOL4, ×103/µL | 4.53 (2.97–7.7) | 5 (2.25–7.73) | 0.8382 | 5.62 (2.35–7.990 | 4.3 (1.8–5) | 0.0332 * |
| ANC difference between DOL1 and DOL 4 | 0.6 (−2.14–3.57) | 1.37 (0.11–2.05) | 0.2734 | 1.48 (−0.08–2.6) | 1.26 (1.21–1.9) | 0.9660 |
| I/T ratio DOL1 | 0.14 (0.09–0.19) | 0.13 (0.09–018) | 0.3485 | 0.14 (0.1–0.17) | 0.10 (0.06–0.18) | 0.3710 |
| I/T ratio DOL4 | 0.18 (0.12–0.20) | 0.14 (0.07–0.18) | 0.0007 | 0.10 (0.07–0.17) | 0.14 (0.12–0.18) | 0.2501 |
| I/T ratio difference between DOL1 and DOL4 | −0.04 (−0.06–0.04) | 0.01 (−004–0.08) | 0.0042 | 0.02 (−0.04–0.10) | −0.01 (−0.04–0.06) | 0.036 8 * |
| Platelet lineage, median (quartile) | ||||||
| PLT DOL1, ×103/µL | 210 (178–272) | 203 (153–302) | 0.6722 | 274 (161–346) | 184 (145–247) | 0.0609 |
| PLT DOL4, ×103/µL | 258 (178–320) | 201 (132–279) | 0.0098 * | 256 (113–331) | 166 (134–174) | 0.0106 * |
| PLT difference between DOL1 and DOL 4 | −27 (−85–22) | 43.5 (−17.5–65) | 0.0004 * | 29 (−75–59) | 50 (2–113) | 0.0966 |
| MPV DOL1, μm3 | 10.1 (9.7–10.7) | 10.1 (9.5–11.2) | 0.9334 | 9.7 (9.4–11.2) | 10.4 (9.9–11.4) | 0.0752 |
| MPV DOL4, μm3 | 10.7 (10.3–11.3) | 11.3 (10.9–11.8) | 0.0009 * | 11.3 (11–12.2) | 10.9 (10.5–11.8) | 0.1729 |
| MPV difference between DOL1 and DOL4 | −0.6 (−1–−0.3) | −1.3 (−1.6–−0.4) | 0.0139 | −1.4 (−1.8–−0.9) | −0.4 (−1.4–0) | 0.0413 |
| PCT DOL1, % | 0.22 (0.19–0.27) | 0.20 (0.15–0.32) | 0.3931 | 0.26 (0.18–0.33) | 0.19 (0.13–0.23) | 0.1182 |
| PCT DOL4, % | 0.27 (0.20–0.32) | 0.28 (0.22–0.32) | 0.8623 | 0.28 (0.14–0.34) | 0.27 (0.22–0.31) | 0.8313 |
| PCT difference between DOL1 and DOL4 | −0.04 (−0.1–0.03) | −0.02 (−0.09–0.02) | 0.6994 | −0.01 (−0.09–0.04) | −0.04 (−0.12–0) | 0.0991 |
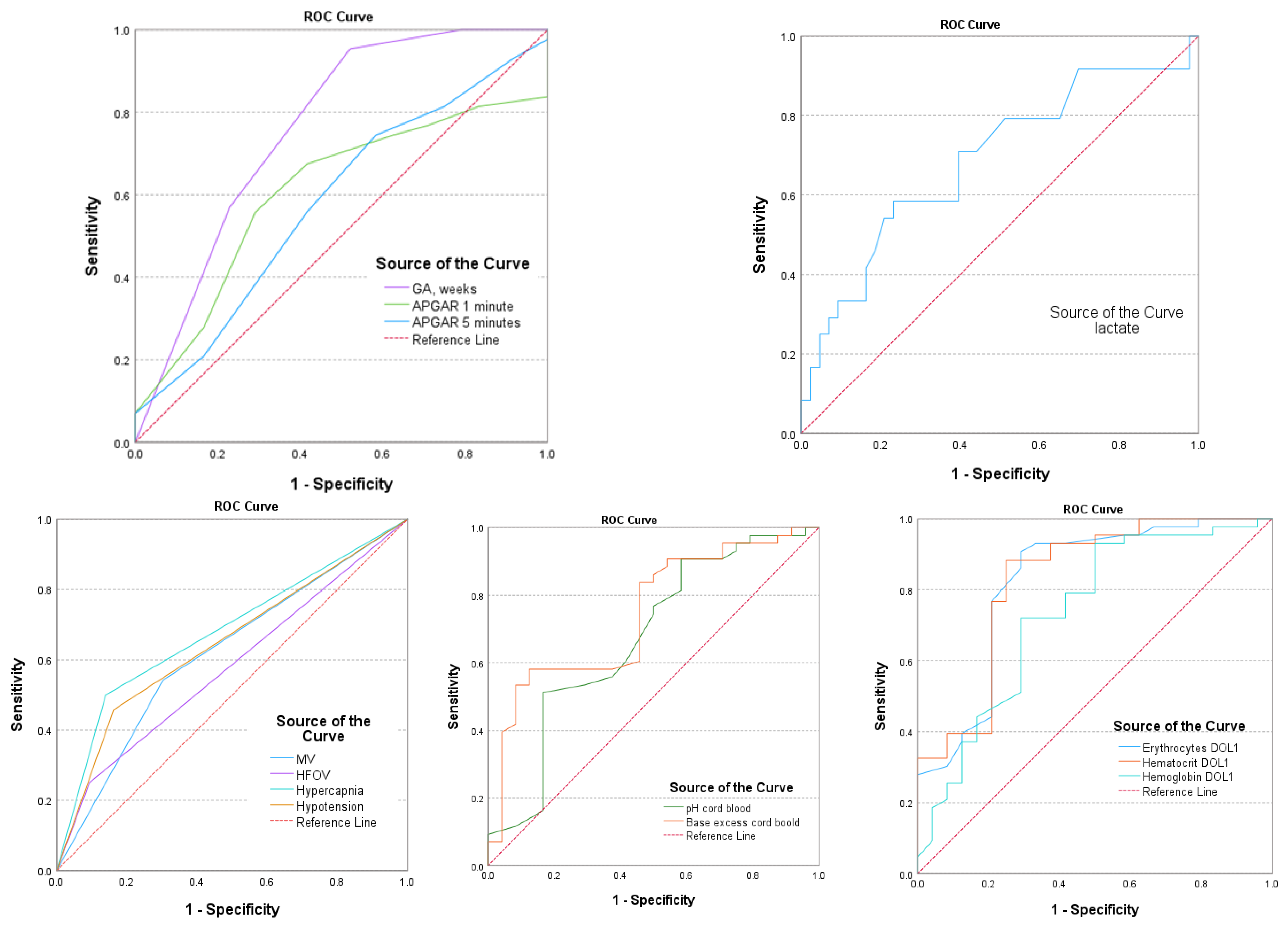
| Univariate Analysis | AUC (95% Confidence Interval) | Std. Error | p-Value | Se | Sp | Cut-Off Levels |
|---|---|---|---|---|---|---|
| GA, weeks | 0.760 (0.669–0.851) | 0.046 | 0.001 * | 86.5 | 83.4 | 26 |
| Apgar 1 min | 0.606 (0.508–0.703) | 0.050 | 0.043 | 78.4 | 68.7 | 5 |
| Apgar 5 min | 0.582 (0.482–0.683) | 0.051 | 0.115 | 65.3 | 54.7 | 6 |
| MV, yes | 0.620 (0.519–0.720) | 0.051 | 0.022 * | 82.9 | 81.6 | - |
| HFOV, yes | 0.578 (0.474–0.683) | 0.053 | 0.133 | 62.1 | 50.3 | - |
| Hypercapnia, yes | 0.680 (0.581–0.780) | 0.051 | 0.001 * | 87.1 | 82.8 | - |
| Hypotension, yes | 0.648 (0.547–0.749) | 0.052 | 0.005 * | 75.6 | 77.5 | - |
| pH | 0.673 (0.575–0.772) | 0.050 | 0.001 * | 55.8 | 52.9 | 7.09 |
| Base excess—BE, mmol/L | 0.742 (0.656–0.829) | 0.044 | <0.001 * | 68.2 | 77.8 | −8.23 |
| Lactate, mmol/L | 0.686 (0.588–0.783) | 0.050 | <0.001 * | 74.1 | 69.4 | 4.8 |
| HGB DOL1, g/dL | 0.806 (0.721–0.958) | 0.023 | 0.002 * | 89.6 | 88.6 | 13.9 |
| HCT DOL1, % | 0.922 (0.841–0.985) | 0.019 | <0.001 * | 88.4 | 91.3 | 42.6 |
| ERY DOL1, 106/µL | 0.895 (0.796–0.963) | 0.035 | 0.001 * | 89.6 | 90.4 | 3.82 |
| β | S.E. | p-Value | OR Exp(B) | 95% CI for EXP(B) | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Neonatal Parameters | ||||||
| Gestational age | β1: 3.002 | 0.002 | 0.017 * | 3.002 | 2.684 | 4.236 |
| Hypercapnia | β2: 1.564 | 0.506 | 0.002 * | 4.780 | 2.774 | 4.879 |
| Hypotension | β3: 1.581 | 0.670 | 0.018 * | 4.860 | 2.308 | 5.062 |
| BE | β4: −0.250 | 0.106 | 0.018 * | 1.779 | 1.634 | 2.958 |
| Constant | −5.572 | 2.161 | 0.010 * | 0.004 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cucerea, M.; Moscalu, M.; Simon, M.; Ognean, M.L.; Mitranovici, M.-I.; Chiorean, D.M.; Marian, R. The Early Hematological Profile and Its Variations: A Useful Tool in the Prediction of Intraventricular Hemorrhage in Extremely Preterm Infants. Medicina 2024, 60, 410. https://doi.org/10.3390/medicina60030410
Cucerea M, Moscalu M, Simon M, Ognean ML, Mitranovici M-I, Chiorean DM, Marian R. The Early Hematological Profile and Its Variations: A Useful Tool in the Prediction of Intraventricular Hemorrhage in Extremely Preterm Infants. Medicina. 2024; 60(3):410. https://doi.org/10.3390/medicina60030410
Chicago/Turabian StyleCucerea, Manuela, Mihaela Moscalu, Marta Simon, Maria Livia Ognean, Melinda-Ildiko Mitranovici, Diana Maria Chiorean, and Raluca Marian. 2024. "The Early Hematological Profile and Its Variations: A Useful Tool in the Prediction of Intraventricular Hemorrhage in Extremely Preterm Infants" Medicina 60, no. 3: 410. https://doi.org/10.3390/medicina60030410