
Reproductive Outcomes in Young Women with Early-Stage Cervical Cancer Greater than 2 cm Undergoing Fertility-Sparing Treatment: A Systematic Review

 ,
,  , ,
, ,  , , ,
, , ,  ,
,
Abstract
1. Introduction
Objectives
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Search Strategy
2.4. Study Selection
2.5. Data Extraction
2.6. Assessment of Risk of Bias
2.7. Outcome Measures and Data Synthesis
3. Results
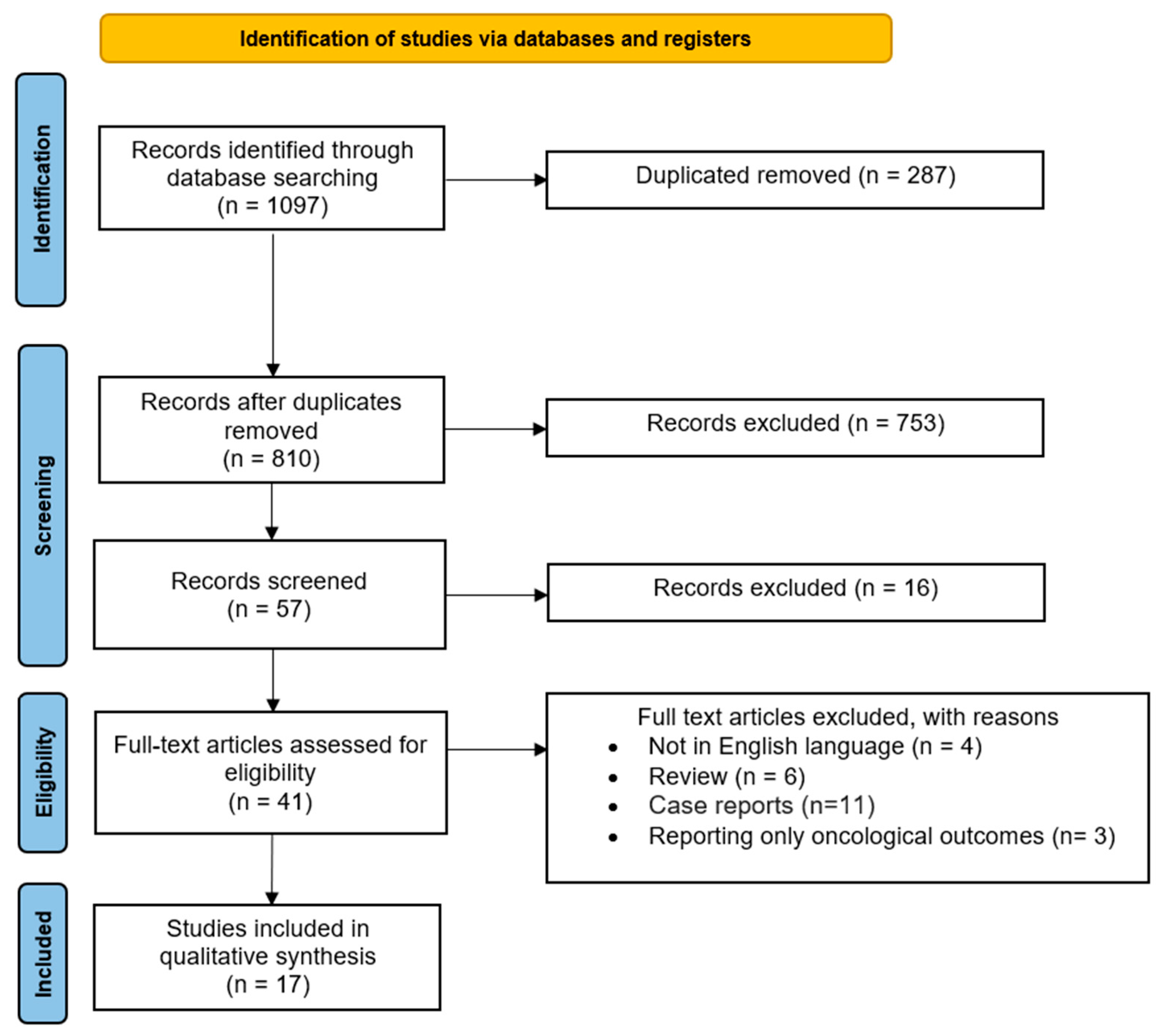
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias of Included Studies
3.4. Synthesis of the Results
3.4.1. Trachelectomy
3.4.2. Conization
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Sonoda, Y.; Abu-Rustum, N.R.; Gemignani, M.L.; Chi, D.S.; Brown, C.L.; Poynor, E.A.; Barakat, R.R. A Fertility-Sparing Alternative to Radical Hysterectomy: How Many Patients May Be Eligible? Gynecol. Oncol. 2004, 95, 534–538. [Google Scholar] [CrossRef] [PubMed]
- Plante, M. Evolution in Fertility-Preserving Options for Early-Stage Cervical Cancer: Radical Trachelectomy, Simple Trachelectomy, Neoadjuvant Chemotherapy. Int. J. Gynecol. Cancer 2013, 23, 982–989. [Google Scholar] [CrossRef]
- Theofanakis, C.; Koulakmanidis, A.-M.; Prodromidou, A.; Haidopoulos, D.; Rodolakis, A.; Thomakos, N. Fertility-Sparing Treatment for Young Patients with Early-Stage Cervical Cancer: A Dawn of a New Era. Front. Surg. 2022, 9, 867993. [Google Scholar] [CrossRef]
- Koh, W.-J.; Abu-Rustum, N.R.; Bean, S.; Bradley, K.; Campos, S.M.; Cho, K.R.; Chon, H.S.; Chu, C.; Clark, R.; Cohn, D.; et al. Cervical Cancer, Version 3.2019, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2019, 17, 64–84. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wu, X.; Li, X.; Ju, X. Abdominal Radical Trachelectomy: Is It Safe for IB1 Cervical Cancer with Tumors ≥ 2 Cm? Gynecol. Oncol. 2013, 131, 87–92. [Google Scholar] [CrossRef] [PubMed]
- SEER Cancer Statistics Review, 1975–2018 [Internet]. 2021. Available online: https://seer.cancer.gov/csr/1975_2018/index.html (accessed on 19 March 2024).
- Wethington, S.L.; Sonoda, Y.; Park, K.J.; Alektiar, K.M.; Tew, W.P.; Chi, D.S.; Leitao, M.M.; Jewell, E.; Barakat, R.R.; Abu-Rustum, N.R. Expanding the Indications for Radical Trachelectomy: A Report on 29 Patients with Stage IB1 Tumors Measuring 2–4 Centimeters. Int. J. Gynecol. Cancer 2013, 23, 1092–1098. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Xu, H.; Zhang, L.; Qiao, Y. Cervical Cancer: Epidemiology, Risk Factors and Screening. Chin. J. Cancer Res. 2020, 32, 720–728. [Google Scholar] [CrossRef] [PubMed]
- Ghebre, R.G.; Grover, S.; Xu, M.J.; Chuang, L.T.; Simonds, H. Cervical Cancer Control in HIV-Infected Women: Past, Present and Future. Gynecol. Oncol. Rep. 2017, 21, 101–108. [Google Scholar] [CrossRef]
- Despot, A.; Fureš, R.; Despot, A.-M.; Mikuš, M.; Zlopaša, G.; D’Amato, A.; Chiantera, V.; Serra, P.; Etrusco, A.; Laganà, A.S. Reactive Oxygen Species within the Vaginal Space: An Additional Promoter of Cervical Intraepithelial Neoplasia and Uterine Cervical Cancer Development? Open Med. 2023, 18, 20230826. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated Guidance for Trusted Systematic Reviews: A New Edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical Evaluation of the Newcastle-Ottawa Scale for the Assessment of the Quality of Nonrandomized Studies in Meta-Analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Home—2020. The Centre for Evidence-Based Medicine. Available online: https://www.cebm.net/ (accessed on 20 January 2024).
- Cao, D.Y.; Yang, J.X.; Wu, X.H.; Chen, Y.L.; Li, L.; Liu, K.J.; Cui, M.H.; Xie, X.; Wu, Y.M.; Kong, B.H.; et al. Comparisons of Vaginal and Abdominal Radical Trachelectomy for Early-Stage Cervical Cancer: Preliminary Results of a Multi-Center Research in China. Br. J. Cancer 2013, 109, 2778–2782. [Google Scholar] [CrossRef] [PubMed][Green Version]
- de Vincenzo, R.; Ricci, C.; Fanfani, F.; Gui, B.; Gallotta, V.; Fagotti, A.; Ferrandina, G.; Scambia, G. Neoadjuvant Chemotherapy Followed by Conization in Stage IB2-IIA1 Cervical Cancer Larger than 2 Cm: A Pilot Study. Fertil. Steril. 2021, 115, 148–156. [Google Scholar] [CrossRef]
- Deng, X.; Zhang, Y.; Li, D.; Zhang, X.; Guo, H.; Wang, F.; Sheng, X. Abdominal Radical Trachelectomy Guided by Sentinel Lymph Node Biopsy for Stage IB1 Cervical Cancer with Tumors >2 cm. Oncotarget 2017, 8, 3422–3429. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Zhang, Y.; Chen, X.; Sun, L.; Chen, K.; Sheng, X. Surgical and Oncologic Outcomes of Radical Abdominal Trachelectomy Versus Hysterectomy for Stage IA2-IB1 Cervical Cancer. J. Minim. Invasive Gynecol. 2019, 26, 484–491. [Google Scholar] [CrossRef] [PubMed]
- Lanowska, M.; Mangler, M.; Speiser, D.; Bockholdt, C.; Schneider, A.; Köhler, C.; Vasiljeva, J.; Al-Hakeem, M.; Vercellino, G.F. Radical Vaginal Trachelectomy after Laparoscopic Staging and Neoadjuvant Chemotherapy in Women with Early-Stage Cervical Cancer over 2 Cm: Oncologic, Fertility, and Neonatal Outcome in a Series of 20 Patients. Int. J. Gynecol. Cancer 2014, 24, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Lintner, B.; Saso, S.; Tarnai, L.; Novak, Z.; Palfalvi, L.; Del Priore, G.; Smith, J.R.; Ungar, L. Use of Abdominal Radical Trachelectomy to Treat Cervical Cancer Greater than 2 Cm in Diameter. Int. J. Gynecol. Cancer 2013, 23, 1065–1070. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Zhang, Y.; Wang, S.; Guo, S.; Guo, H.; Zhang, Z.; Liu, C. Neoadjuvant Intra-Arterial Chemotherapy Followed by Total Laparoscopic Radical Trachelectomy in Stage IB1 Cervical Cancer. Fertil. Steril. 2014, 101, 812–817. [Google Scholar] [CrossRef] [PubMed]
- Marchiolè, P.; Ferraioli, D.; Moran, E.; Mammoliti, S.; Tigaud, J.-D.; Beurrier, F.; Chopin, N.; Mathevet, P. NACT and Laparoscopic-Assisted Radical Vaginal Trachelectomy in Young Patients with Large (2–5 cm) High Risk Cervical Cancers: Safety and Obstetrical Outcome. Surg. Oncol. 2018, 27, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Plante, M.; Lau, S.; Brydon, L.; Swenerton, K.; LeBlanc, R.; Roy, M. Neoadjuvant Chemotherapy Followed by Vaginal Radical Trachelectomy in Bulky Stage IB1 Cervical Cancer: Case Report. Gynecol. Oncol. 2006, 101, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Rendón, G.J.; Lopez Blanco, A.; Aragona, A.; Saadi, J.M.; Di Guilmi, J.; Arab Eblen, C.; Heredia Muñoz, F.; Pareja, R. Oncological and Obstetrical Outcomes after Neo-Adjuvant Chemotherapy Followed by Fertility-Sparing Surgery in Patients with Cervical Cancer ≥2 Cm. Int. J. Gynecol. Cancer 2021, 31, 462–467. [Google Scholar] [CrossRef] [PubMed]
- Robova, H.; Halaska, M.J.; Pluta, M.; Skapa, P.; Matecha, J.; Lisy, J.; Rob, L. Oncological and Pregnancy Outcomes after High-Dose Density Neoadjuvant Chemotherapy and Fertility-Sparing Surgery in Cervical Cancer. Gynecol. Oncol. 2014, 135, 213–216. [Google Scholar] [CrossRef] [PubMed]
- Salihi, R.; Leunen, K.; Van Limbergen, E.; Moerman, P.; Neven, P.; Vergote, I. Neoadjuvant Chemotherapy Followed by Large Cone Resection as Fertility-Sparing Therapy in Stage IB Cervical Cancer. Gynecol. Oncol. 2015, 139, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Tesfai, F.M.; Kroep, J.R.; Gaarenstroom, K.; De Kroon, C.; Van Loenhout, R.; Smit, V.; Trimbos, B.; Nout, R.A.; van Poelgeest, M.I.E.; Beltman, J.J. Fertility-Sparing Surgery of Cervical Cancer >2 cm (International Federation of Gynecology and Obstetrics 2009 Stage IB1-IIA) after Neoadjuvant Chemotherapy. Int. J. Gynecol. Cancer 2020, 30, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Vercellino, G.F.; Piek, J.M.J.; Schneider, A.; Köhler, C.; Mangler, M.; Speiser, D.; Chiantera, V. Laparoscopic Lymph Node Dissection Should Be Performed before Fertility Preserving Treatment of Patients with Cervical Cancer. Gynecol. Oncol. 2012, 126, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Zusterzeel, P.L.M.; Aarts, J.W.M.; Pol, F.J.M.; Ottevanger, P.B.; van Ham, M.A.P.C. Neoadjuvant Chemotherapy Followed by Vaginal Radical Trachelectomy as Fertility-Preserving Treatment for Patients with FIGO 2018 Stage 1B2 Cervical Cancer. Oncologist 2020, 25, e1051–e1059. [Google Scholar] [CrossRef] [PubMed]
- Saito, T.; Matsuura, M.; Tamate, M.; Iwasaki, M.; Mariya, T. Radical Vaginal Trachelectomy. Surg. J. 2021, 7, S103–S107. [Google Scholar] [CrossRef] [PubMed]
- Tsafrir, Z.; Aoun, J.; Hanna, R.; Papalekas, E.; Schiff, L.; Theoharis, E.; Eisenstein, D. Robotic Trachelectomy After Supracervical Hysterectomy for Benign Gynecologic Disease. JSLS 2016, 20, e2016.00027. [Google Scholar] [CrossRef] [PubMed]
- Salvo, G.; Pareja, R.; Ramirez, P.T. Minimally Invasive Radical Trachelectomy: Considerations on Surgical Approach. Best. Pract. Res. Clin. Obstet. Gynaecol. 2021, 75, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Pecorino, B.; Laganà, A.S.; Mereu, L.; Ferrara, M.; Carrara, G.; Etrusco, A.; Di Donna, M.C.; Chiantera, V.; Cucinella, G.; Barra, F.; et al. Evaluation of Borderline Ovarian Tumor Recurrence Rate after Surgery with or without Fertility-Sparing Approach: Results of a Retrospective Analysis. Healthcare 2023, 11, 1922. [Google Scholar] [CrossRef] [PubMed]
- Etrusco, A.; Laganà, A.S.; Chiantera, V.; Mikuš, M.; Arsalan, H.M.; d’Amati, A.; Vitagliano, A.; Cicinelli, E.; Favilli, A.; D’Amato, A. Reproductive and Oncologic Outcomes in Young Women with Stage IA and Grade 2 Endometrial Carcinoma Undergoing Fertility-Sparing Treatment: A Systematic Review. Biomolecules 2024, 14, 306. [Google Scholar] [CrossRef] [PubMed]
- Gullo, G.; Etrusco, A.; Cucinella, G.; Perino, A.; Chiantera, V.; Laganà, A.S.; Tomaiuolo, R.; Vitagliano, A.; Giampaolino, P.; Noventa, M.; et al. Fertility-Sparing Approach in Women Affected by Stage I and Low-Grade Endometrial Carcinoma: An Updated Overview. Int. J. Mol. Sci. 2021, 22, 11825. [Google Scholar] [CrossRef] [PubMed]
- Etrusco, A.; Buzzaccarini, G.; Laganà, A.S.; Chiantera, V.; Vitale, S.G.; Angioni, S.; D’Alterio, M.N.; Nappi, L.; Sorrentino, F.; Vitagliano, A.; et al. Use of Diode Laser in Hysteroscopy for the Management of Intrauterine Pathology: A Systematic Review. Diagnostics 2024, 14, 327. [Google Scholar] [CrossRef] [PubMed]
- Etrusco, A.; Laganà, A.S.; Chiantera, V.; Gerli, S.; Carugno, J.; Sorrentino, F.; Riemma, G.; Vitagliano, A.; Favilli, A. Efficacy, Safety, and Feasibility of the Treatment of Intrauterine Pathologies with the Mini-Resectoscope: A Systematic Review. Int. J. Gynaecol. Obstet. 2024. [Google Scholar] [CrossRef] [PubMed]
- Mazzon, I.; Etrusco, A.; Laganà, A.S.; Chiantera, V.; Di Angelo Antonio, S.; Tosto, V.; Gerli, S.; Favilli, A. Training in Diagnostic Hysteroscopy: The “Arbor Vitae” Method. Medicina 2023, 59, 1019. [Google Scholar] [CrossRef] [PubMed]
- Tseng, J.H.; Aloisi, A.; Sonoda, Y.; Gardner, G.J.; Zivanovic, O.; Abu-Rustum, N.R.; Leitao, M.M. Long-Term Oncologic Outcomes of Uterine-Preserving Surgery in Young Women With Stage Ib1 Cervical Cancer. Int. J. Gynecol. Cancer 2018, 28, 1350–1359. [Google Scholar] [CrossRef] [PubMed]
- Gwacham, N.I.; McKenzie, N.D.; Fitzgerald, E.R.; Ahmad, S.; Holloway, R.W. Neoadjuvant Chemotherapy Followed by Fertility Sparing Surgery in Cervical Cancers Size 2–4 Cm; Emerging Data and Future Perspectives. Gynecol. Oncol. 2021, 162, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Rydzewska, L.; Tierney, J.; Vale, C.L.; Symonds, P.R. Neoadjuvant Chemotherapy plus Surgery versus Surgery for Cervical Cancer. Cochrane Database Syst. Rev. 2012, 12, CD007406. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Shi, Y.; Wang, S.; Lu, Q. Meta-Analysis Showing That Early Response to Neoadjuvant Chemotherapy Predicts Better Survival among Cervical Cancer Patients. Oncotarget 2017, 8, 59609–59617. [Google Scholar] [CrossRef] [PubMed]
- Cibula, D.; McCluggage, W.G. Sentinel Lymph Node (SLN) Concept in Cervical Cancer: Current Limitations and Unanswered Questions. Gynecol. Oncol. 2019, 152, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Ai, C.; Zhang, L.; Ding, W.; Zhong, S.; Li, Z.; Li, M.; Zhang, H.; Zhang, L.; Zhang, L.; Hu, H. A Nomogram-Based Optimized Radscore for Preoperative Prediction of Lymph Node Metastasis in Patients with Cervical Cancer after Neoadjuvant Chemotherapy. Front. Oncol. 2023, 13, 1117339. [Google Scholar] [CrossRef] [PubMed]
- Plaikner, A.; Siegler, K.; Hertel, H.; Jacob, A.; Petzel, A.; Schubert, M.; Blohmer, J.-U.; Böhmer, G.; Marnitz, S.; Ragosch, V.; et al. Fertility Sparing Therapy in Women with Lymph Node Negative Cervical Cancer >2cm—Oncologic and Fertility Outcomes of Neoadjuvant Chemotherapy Followed by Radical Vaginal Trachelectomy. Int. J. Gynecol. Cancer 2023, 33, 1542–1547. [Google Scholar] [CrossRef] [PubMed]
- Maneo, A.; Chiari, S.; Bonazzi, C.; Mangioni, C. Neoadjuvant Chemotherapy and Conservative Surgery for Stage IB1 Cervical Cancer. Gynecol. Oncol. 2008, 111, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Pareja, R.; Rendón, G.J.; Sanz-Lomana, C.M.; Monzón, O.; Ramirez, P.T. Surgical, Oncological, and Obstetrical Outcomes after Abdominal Radical Trachelectomy—A Systematic Literature Review. Gynecol. Oncol. 2013, 131, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Malmsten, C.; Hellberg, P.; Bergmark, K.; Dahm-Kähler, P. Long-Term Fertility, Oncological, and Quality-of-Life Outcomes after Trachelectomy in Early Stage Cervical Cancer. Arch. Gynecol. Obstet. 2019, 299, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Batman, S.H.; Schmeler, K.M. Fertility-Sparing and Less Radical Surgery for Cervical Cancer. Curr. Oncol. Rep. 2022, 24, 1541–1548. [Google Scholar] [CrossRef] [PubMed]
- Okugawa, K.; Kobayashi, H.; Sonoda, K.; Kaneki, E.; Kawano, Y.; Hidaka, N.; Egashira, K.; Fujita, Y.; Yahata, H.; Kato, K. Oncologic and Obstetric Outcomes and Complications during Pregnancy after Fertility-Sparing Abdominal Trachelectomy for Cervical Cancer: A Retrospective Review. Int. J. Clin. Oncol. 2017, 22, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Kasuga, Y.; Ikenoue, S.; Tanaka, M.; Ochiai, D. Management of Pregnancy after Radical Trachelectomy. Gynecol. Oncol. 2021, 162, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Rob, L.; Skapa, P.; Robova, H. Fertility-Sparing Surgery in Patients with Cervical Cancer. Lancet Oncol. 2011, 12, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Bentivegna, E.; Gouy, S.; Maulard, A.; Chargari, C.; Leary, A.; Morice, P. Oncological Outcomes after Fertility-Sparing Surgery for Cervical Cancer: A Systematic Review. Lancet Oncol. 2016, 17, e240–e253. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, P.T.; Pareja, R.; Rendón, G.J.; Millan, C.; Frumovitz, M.; Schmeler, K.M. Management of Low-Risk Early-Stage Cervical Cancer: Should Conization, Simple Trachelectomy, or Simple Hysterectomy Replace Radical Surgery as the New Standard of Care? Gynecol. Oncol. 2014, 132, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Jensen, K.E.; Hannibal, C.G.; Nielsen, A.; Jensen, A.; Nøhr, B.; Munk, C.; Kjaer, S.K. Social Inequality and Incidence of and Survival from Cancer of the Female Genital Organs in a Population-Based Study in Denmark, 1994–2003. Eur. J. Cancer 2008, 44, 2003–2017. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, K.; Meernik, C.; Wu, C.-F.; Murphy, C.C.; Baker, V.L.; Jarmon, P.; Brady, P.C.; Nitecki, R.; Nichols, H.B.; Rauh-Hain, J.A. Disparities in Fertility-Sparing Treatment and Use of Assisted Reproductive Technology After a Diagnosis of Cervical, Ovarian, or Endometrial Cancer. Obstet. Gynecol. 2023, 141, 341–353. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Year | Type | Main Outcome | Country | Patient (n) | Cervical Cancer > 2 cm, n (% of total) | Age (Median) |
|---|---|---|---|---|---|---|---|
| Cao et al. [16] | 2013 | Prospective case-control | To compare the surgical and pathologic characteristics, the prognosis, and fertility outcomes of the patients treated by VRT or ART | China | 150 | 48 (32) | 30.0 (18–39) |
| De Vincenzo et al. [17] | 2021 | Prospective observational | To evaluate the feasibility of NACT followed by CKC in patients with 2018 FIGO stage IB2–IIA1 cervical cancer who desired to maintain fertility | Italy | 13 | 9 (69.2) | 29 (23–36) |
| Deng et al. [18] | 2016 | Retrospective observational | To evaluate the safety of SLNB-guided ART by observing surgical, oncologic, and fertility outcomes in patients who wished to preserve their fertility | China | 45 | 45 (100) | 28.5 (19–40) |
| Guo et al. [19] | 2018 | Retrospective observational | To compare the surgical and oncologic outcomes between ART and RH for stage IA2–IB1 cervical cancer | China | 329 | 75 (22.8) | 31 (18–42) |
| Lanowska et al. [20] | 2013 | Retrospective observational | To assess the oncologic and fertility outcomes of treatment in patients with cervical cancer of more than 2 cm seeking parenthood | Germany | 20 | 20 (100) | 32 (26–41) |
| Li et al. [6] | 2013 | Retrospective observational | To report the surgical and oncological safety of ART for selected patients with cervical cancer ≥2 cm in size | China | 133 | 62 (46.6) | 30.4 (20–44) |
| Lintner et al. [21] | 2013 | Retrospective observational | To report ART experience in patients with a cervical cancer more than 2 cm in diameter | Hungary | 45 | 45 (100) | 32 (24–43) |
| Lu et al. [22] | 2014 | Retrospective observational | To support the feasibility and safety of intra-arterial NACT followed by total laparoscopic radical trachelectomy in stage IB1 cervical cancer with a tumor larger than 2 cm | China | 7 | 7 (100) | 28 (22–35) |
| Marchiolè et al. [23] | 2018 | Retrospective observational | To assess the oncological and reproductive outcomes of patients with early-stage large cervical cancers (2–5 cm) undergoing FST | France | 19 | 19 (100) | 28.3 (21–37) |
| Plante et al. [24] | 2006 | Case series | To present the cases of 3 young women with bulky stage IB1 cervical cancer treated with NACT followed by laparoscopic pelvic node dissection and VRT | Canada | 3 | 3 (100) | 35 (26–36) |
| Rendòn et al. [25] | 2020 | Retrospective observational | To report on the oncological and obstetrical outcomes of NACT followed by FST in patients diagnosed with cervical cancer ≥2 cm | Colombia | 25 | 25 (100) | 27 (20–37) |
| Robova et al. [26] | 2014 | Prospective observational | To assess oncological and pregnancy outcomes after high-dose density NACT and FST in cervical cancer | Czech Republic | 28 | 28 (100) | 28.6 (15–34) |
| Salihi et al. [27] | 2015 | Retrospective observational | To discuss the cases of 11 patients with cervical carcinoma stage IB treated with NACT followed by large cone resection | Belgium | 10 | 5 (50) | 31.7 (25–36) |
| Tesfai et al. [28] | 2015 | Retrospective observational | To assess the feasibility, safety, oncological, and obstetric outcomes in patients with cervical tumors >2 cm treated with NACT in preparation for ART | Netherlands | 19 | 19 (100) | 28 (19–36) |
| Vercellino et al. [29] | 2012 | Prospective observational | To assess the results of treatment of women with stage I cervical cancer >2 cm in diameter seeking fertility preservation | Germany | 18 | 6 (33.3) | 31.3 (25–38) |
| Wethington et al. [8] | 2016 | Retrospective observational | To report the author’s trachelectomy experience with cervical tumors measuring 2–4 cm | United States | 29 | 9 (31) | 31 (22–40) |
| Zusterzeel et al. [30] | 2020 | Retrospective observational | To evaluate the oncological and fertility outcomes of treatment in patients receiving an FST consisting of NACT followed by VRT | Netherlands | 18 | 14 (77.8) | 29 (23–36) |
| Author | Tumor Size (cm) | Assessment |
|---|---|---|
| Cao et al. [16] | >2 <4 | MRI or physical examination |
| De Vincenzo et al. [17] | >2 <4 | MRI and physical examination |
| Deng et al. [18] | >2 <4 | MRI |
| Guo et al. [19] | >2 <4 | No data |
| Lanowska et al. [20] | 2.1–5.0 (range) | MRI |
| Li et al. [6] | >2 <4 | MRI, physical examination, or final pathology exam |
| Lintner et al. [21] | >2 <4 (55%) <2 (45%) | CT, PET-CT, or MRI |
| Lu et al. [22] | ≥2.5 <4.0 | MRI and physical examination |
| Marchiolè et al. [23] | ≥2.9 <5.1 | MRI and physical examination |
| Plante et al. [24] | >2 <4 | MRI and physical examination |
| Rendòn et al. [25] | >2 <6 | MRI (76%), CT (12%), physical examination (12%) |
| Robova et al. [26] | >2 (no data regarding maximum size) | MRI or TV-US |
| Salihi et al. [27] | >2 <5.2 | MRI, CT or PET-CT |
| Tesfai et al. [28] | 3.5–6.0 (range) | MRI |
| Vercellino et al. [29] | 2.1–5.0 (range) | MRI, laparoscopic or hysteroscopic staging |
| Wethington et al. [8] | >2 <4 | MRI, physical examination, or pathology exam |
| Zusterzeel et al. [30] | 2.2–4.0 (range) | MRI and physical examination |
| Cao et al. [16] | Deng et al. [18] | Guo et al. [19] | Lanowska et al. [20] | Li et al. [6] | Lintner et al. [21] | Lu et al. [22] | Marchiolè et al. [23] | Plante et al. [24] | Rendòn et al. [25] | Robova et al. [26] | Tesfai et al. [28] | Vercellino et al. [29] | Wethington et al. [8] | Zusterzeel et al. [30] | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patients, n | 150 | 45 | 329 | 20 | 133 | 45 | 7 | 19 | 3 | 25 | 28 | 19 | 18 | 29 | 18 |
| Year | 2013 | 2016 | 2018 | 2013 | 2013 | 2013 | 2014 | 2018 | 2006 | 2020 | 2014 | 2015 | 2012 | 2016 | 2020 |
| Cervical cancer greater than 2 cm, n (%) | 48 (32) | 45 (100) | 75 (22.8) | 20 (100) | 62 (46.6) | 45 (100) | 7 (100) | 19 (100) | 3 (100) | 25 (100) | 28 (100) | 19 (100) | 6 (33.3) | 9 (31) | 14 (77.8) |
| Age, years (median) | 30.0 (18–39) | 28.5 (19–40) | 31(18–42) | 32 (26–41) | 30.4 (20–44) | 32 (24–43) | 28 (22–35) | 28.3 (21–37) | 35 (26–36) | 27 (20–37) | 28.6 (15–34) | 28 (19–36) | 31.3 (25–38) | 31 (22–40) | 29 (23–36) |
| FST approach employed, n (%) | ART, 24 (50) VRT, 24 (50) | ART, 45 (100) | ART, 75 (100) | VRT, 20 (100) | ART, 55 (88.7) | ART, 45 (100) | ART, 7 (100) | LARVT | VRT, 3 (100) | ART, 20 (80) | VRT, 28 (100) | ART, 16 (84.2) | VRT, 6 (100) | ART or VRT, 9 (31) | VRT, 14 (100) |
| NACT, n (%) | 0 | 0 | 0 | 20 (100) | 0 | 0 | 7 (100) | 19 (100) | 3 (100) | 25 (100) | 28 (100) | 19 (100) | 6 (100) | 0 | 14 (100) |
| NACT regimen, n (%) | - | - | - | TIP for 2 cycles, 15 (75) TIP for 3 cycles, 4 (20) TP for 2 cycles, 1 (5) | - | - | Bleomycin + cisplatin + mitomycin, 7 (100) | TIP for 4, 3 or 2 cycles, 11 (57.9) TP for 6, 4 or 3 cycles, 3 (15.8) TEP for 4 or 3 cycles, 5 (26.3) | TIP for 2 cycles, 3 (100) | TC, 8 (32) TP, 7 (28) TIP, 4 (16) Paclitaxel + cisplatin + 5- fluorouracil, 3 (12) 5- fluorouracil + ifosfamide + cisplatin, 2 (8) Vincristine + bleomycin + cisplatin, 1 (4) | Cisplatin + ifosfamide, 15 (53.6) Cisplatin + doxorubicin, 13 (46.4) | TP for 6 cycles, 11 (57.9) TP for 2 or 3 cycles, 8 (42.1) | TIP for 2 or 3 cycles, 6 (100) | - | TP for 2, 3 or 6 cycles, 14 (100) |
| Nulliparous, n (%) | 112 (74.7) | 20 (40.8) | n.d. | 17 (85) | 42 (67.7%) | n.d. | n.d. | n.d. | 2 (66.7) | n.d. | 26 (92.9) | n.d. | n.d. | 24 (83) | 14 (100) |
| Primiparous, n (%) | 38 (25.3) | 29 (59.2) | n.d. | 3 (15) | 20 (32.3%) | n.d. | n.d. | n.d. | 1 (33.3) | n.d. | 2 (7.1) | n.d. | n.d. | (17.2) | 0 |
| Attempted to conceive, n (%) | 24 (50) | 19 (42.2) | 29 (38.7) | 7 (35) | 9 (16.3) | 8 (25.8) | 4 (57.1) | 6 (31.6) | 3 | n.d. | 16 (57.1) | 15 (93.8) | 6 (100) | 2 (22.2) | 7 (50) |
| Follow-up period, months (mean or median) | VRT, 34.4 ART, 20.6 | 37 (18–76) | 75.5 (6–168) | 23.1 ± 26.6 | 30.2 | 27 | 66 (12–90) | n.d. | n.d. | 47 (13–133) | 42 (5–103) | 50 (3–144) | 31.6 | 44 (1–90) | 49.7 (11.4–110.8) |
| Pregnancies, n (%) | 3 (12.5) | 5 (26.3) | 5 (17.2) | 7 (100) | 3 (33.3) | 4 (50) | 2 (28.6) | 3 (50) | 3 (100) | 13 (56.5) | 13 (81.3) | 8 (53.3) | 1 (16.7) | 1 (50) | 6 (85.7) |
| Spontaneous pregnancies, n (%) | n.d. | 5 (100) | n.d. | 7 (100) | n.d. | n.d. | n.d. | n.d. | n.d. | n.d. | 10 (76.9) | 8 (53.3) | n.d. | 1 (100) | 2 (33.3) |
| Assisted reproductive technologies, n (%) | n.d. | 0 | n.d. | 0 | n.d. | n.d. | n.d. | n.d. | n.d. | n.d. | 3 (23.1) | 0 | n.d. | 0 | 4 (66.7) |
| Miscarriages, n (%) | 0 | 4 (80) | 6 (75) | 1 (14.3) | 2 (66.7) | 1 (25) | 1 (50) | 0 | 0 | 1 (7.7) | 3 (23.1) | 2 (25) | 0 | 1 (100) | 2 (33.3) |
| Ectopic pregnancies, n (%) | 0 | 0 | n.d. | 1 (14.3) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Twin pregnancy, n (%) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Preterm delivery, n (%) | n.d. | 0 | n.d. | 2 (28.6) | 0 | 1 (25) | 1 (50) | n.d. | 1 (33.3) | 7 (53.8) | 3 (23.1) | 0 | 0 | 0 | 0 |
| Full-term delivery (%) | n.d. | 1 (20) | n.d. | 2 (42.8) | 1 (33.3) | 2 (50) | 0 | n.d. | 2 (66.7) | 4 (30.8) | 5 | 6 (75) | 1 (100) | 0 | 3 (50) |
| Live births, n (%) | 3 (12.5) | 1 | 2 (25) | 4 (57.1) 1 ongoing pregnancy | 1 (33.3) | 3 (75) | 1 (50) | 3 (100) | 3 (100) | 11 (84.6) 1 ongoing pregnancy | 8 (61.5) 2 ongoing pregnancies | 6 (75) | 1 (100) | 0 | 3 (50) 1 ongoing pregnancy |
| PR (%) | 12.5 | 26.3 | 17.2 | 100 | 33.3 | 50 | 28.6 | 50 | 100 | 56.5 | 81.3 | 53.3 | 16.7 | 50 | 85.7 |
| MR (%) | 0 | 80 | 75 | 28.6 | 66.7 | 25 | 14.3 | 0 | 0 | 7.7 | 23.1 | 25 | 0 | 100 | 33.3 |
| LBR (%) | 100 | 20 | 25 | 57.1 | 33.3 | 75 | 14.3 | 100 | 100 | 84.6 | 61.5 | 75 | 100 | 0 | 50 |
| De Vincenzo et al. [17] | Rendòn et al. [25] | Salihi et al. [27] | |
|---|---|---|---|
| Patients, n | 13 | 25 | 10 |
| Year | 2021 | 2020 | 2015 |
| Cervical cancer greater than 2 cm, n (%) | 13 (100) | 25 (100) | 5 (50) |
| Age, years (median) | 29 (23–36) | 27 (20–37) | 31.7 (25–36) |
| FST approach employed, n (%) | Cold-knife conization, 9 (69.2) | Conization, 5 (20) | Conization, 5 (50) |
| NACT, n (%) | 13 (100) | 25 (100) | 5 (100) |
| NACT regimen, n (%) | TP for 3 cycles, 13 (100) | Carboplatin + paclitaxel, 8 (32) TP, 7 (28) TIP, 4 (16) Paclitaxel + cisplatin + 5- fluorouracil, 3 (12) 5- fluorouracil + ifosfamide + cisplatin, 2 (8) Vincristine + bleomycin + cisplatin, 1 (4) | TP or TP for 3 cycles, 1 (20) TC for 9 cycles, 4 (80) |
| Nulliparous, n (%) | 12 (92.3) | n.d. | 5 (100) |
| Primiparous, n (%) | 1 (7.7) | n.d. | 0 |
| Attempted to conceive, n (%) | 3 (33.3) | n.d. | 5 (100) |
| Follow-up period, months (mean or median) | 37 (18–76) | 47 (13–133) | 58 (13–122) |
| Pregnancies, n (%) | 2 (66.7) | 13 (56.5) | 1 (20) |
| Spontaneous pregnancies, n (%) | 2 (100) | n.d. | 1 (100) |
| Assisted reproductive technologies, n (%) | 0 | n.d. | 0 |
| Miscarriages, n (%) | 0 | 1 (7.7) | 0 |
| Ectopic pregnancies, n (%) | 0 | 0 | 0 |
| Twin pregnancy, n (%) | 0 | 0 | 0 |
| Preterm delivery, n (%) | 1 (50) | 7 (53.8) | 0 |
| Full-term delivery (%) | 1 (50) | 4 (30.8) | 1 (100) |
| Live births, n (%) | 2 (66.7) | 11 (84.6) 1 ongoing pregnancy | 1 (100) |
| PR (%) | 66.7 | 56.5 | 20 |
| MR (%) | 0 | 7.7 | 0 |
| LBR (%) | 66.7 | 84.6 | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Amato, A.; Riemma, G.; Agrifoglio, V.; Chiantera, V.; Laganà, A.S.; Mikuš, M.; Dellino, M.; Maglione, A.; Faioli, R.; Giannini, A.; et al. Reproductive Outcomes in Young Women with Early-Stage Cervical Cancer Greater than 2 cm Undergoing Fertility-Sparing Treatment: A Systematic Review. Medicina 2024, 60, 608. https://doi.org/10.3390/medicina60040608
D’Amato A, Riemma G, Agrifoglio V, Chiantera V, Laganà AS, Mikuš M, Dellino M, Maglione A, Faioli R, Giannini A, et al. Reproductive Outcomes in Young Women with Early-Stage Cervical Cancer Greater than 2 cm Undergoing Fertility-Sparing Treatment: A Systematic Review. Medicina. 2024; 60(4):608. https://doi.org/10.3390/medicina60040608
Chicago/Turabian StyleD’Amato, Antonio, Gaetano Riemma, Vittorio Agrifoglio, Vito Chiantera, Antonio Simone Laganà, Mislav Mikuš, Miriam Dellino, Annamaria Maglione, Raffaele Faioli, Andrea Giannini, and et al. 2024. "Reproductive Outcomes in Young Women with Early-Stage Cervical Cancer Greater than 2 cm Undergoing Fertility-Sparing Treatment: A Systematic Review" Medicina 60, no. 4: 608. https://doi.org/10.3390/medicina60040608
APA StyleD’Amato, A., Riemma, G., Agrifoglio, V., Chiantera, V., Laganà, A. S., Mikuš, M., Dellino, M., Maglione, A., Faioli, R., Giannini, A., Trojano, G., & Etrusco, A. (2024). Reproductive Outcomes in Young Women with Early-Stage Cervical Cancer Greater than 2 cm Undergoing Fertility-Sparing Treatment: A Systematic Review. Medicina, 60(4), 608. https://doi.org/10.3390/medicina60040608