
Breast Cancer in Patients with Previous Endometriosis Showed Low Aggressive Subtype
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
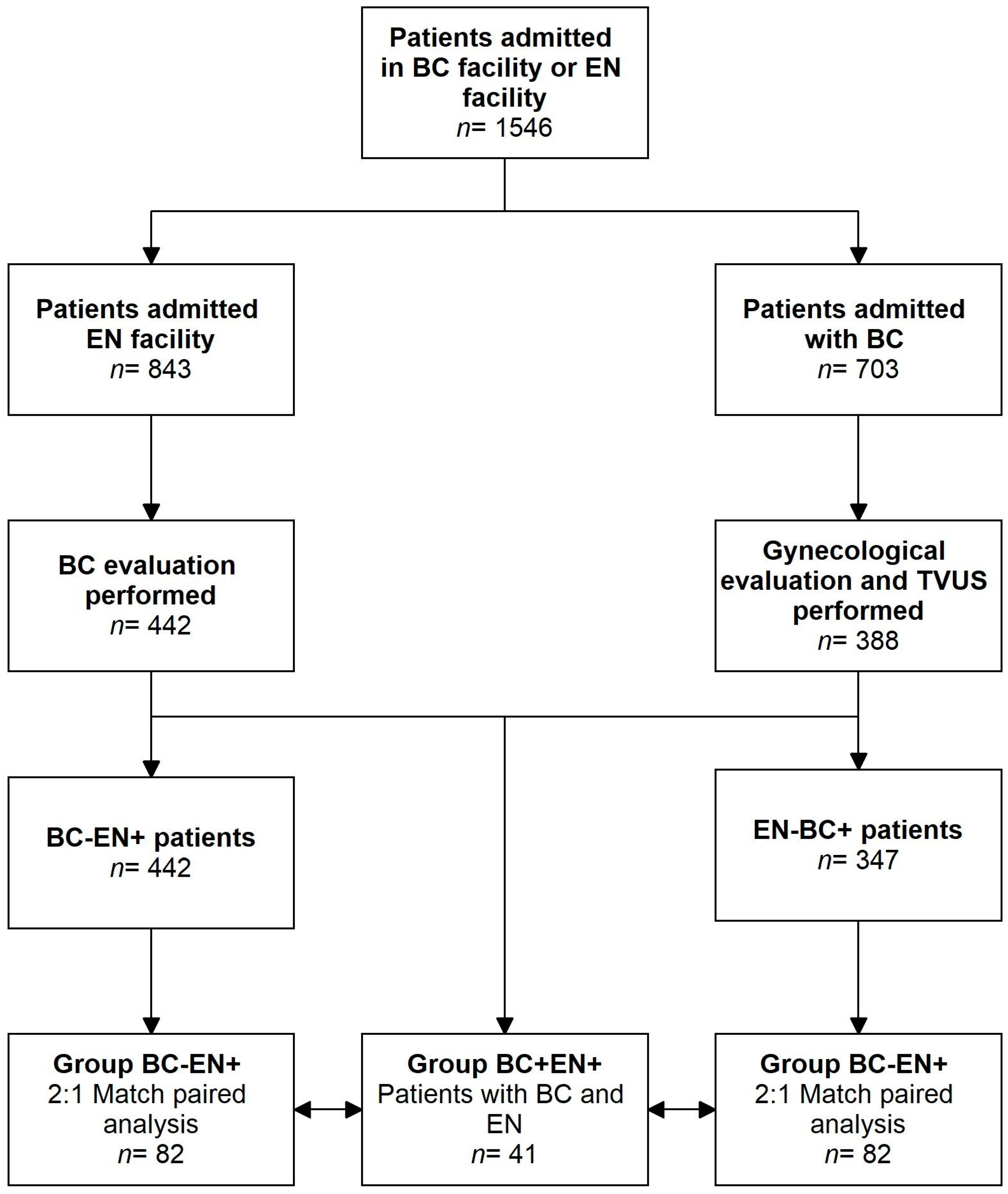
2.1. Study Design and Study Participants
- -
- History of with endometriosis and/or adenomyosis diagnosed through surgery or ultrasonographic examination in our endometriosis center who subsequently received a new BC diagnosis;
- -
- Histological diagnosis of invasive breast cancer on a surgical specimen.
2.2. Clinical Evaluation
2.3. Gynecological Unit Evaluation
2.4. Breast Unit Evaluation
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Crosignani, P.; Olive, D.; Bergqvist, A.; Luciano, A. Advances in the management of endometriosis: An update for clinicians. Hum. Reprod. Update 2006, 12, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Ozkan, S.; Murk, W.; Arici, A. Endometriosis and infertility: Epidemiology and evidence-based treatments. Ann. N. Y. Acad. Sci. 2008, 1127, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Burney, R.O.; Giudice, L.C. Pathogenesis and pathophysiology of endometriosis. Fertil. Steril. 2012, 98, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Thomas, E.J.; Campbell, I.G. Evidence that endometriosis behaves in a malignant manner. Gynecol. Obstet. Investig. 2000, 50, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Kvaskoff, M.; Mu, F.; Terry, K.L.; Harris, H.R.; Poole, E.M.; Farland, L.; Missmer, S.A. Endometriosis: A high-risk population for major chronic diseases? Hum. Reprod. Update 2015, 21, 500–516. [Google Scholar] [CrossRef]
- Sampson, J.A. Endometrial carcinoma of the ovary, arising in endometrial tissue in that organ. Arch. Surg. 1925, 10, 1–72. [Google Scholar] [CrossRef]
- Somigliana, E.; Vigano, P.; Parazzini, F.; Stoppelli, S.; Giambattista, E.; Vercellini, P. Association between endometriosis and cancer: A comprehensive review and a critical analysis of clinical and epidemiological evidence. Gynecol. Oncol. 2006, 101, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Heidemann, L.N.; Hartwell, D.; Heidemann, C.H.; Jochumsen, K.M. The relation between endometriosis and ovarian cancer—A review. Acta Obstet. Gynecol. Scand. 2014, 93, 20–23. [Google Scholar] [CrossRef] [PubMed]
- Pontikaki, A.; Sifakis, S.; Spandidos, D.A. Endometriosis and breast cancer: A survey of the epidemiological studies. Oncol. Lett. 2016, 11, 23–30. [Google Scholar] [CrossRef]
- Kalaitzopoulos, D.R.; Mitsopoulou, A.; Iliopoulou, S.M.; Daniilidis, A.; Samartzis, E.P.; Economopoulos, K.P. Association between endometriosis and gynecological cancers: A critical review of the literature. Arch. Gynecol. Obstet. 2020, 301, 355–367. [Google Scholar] [CrossRef]
- Farland, L.V.; Tamimi, R.M.; Eliassen, A.H.; Spiegelman, D.; Hankinson, S.E.; Chen, W.Y.; Missmer, S.A. Laparoscopically Confirmed Endometriosis and Breast Cancer in the Nurses’ Health Study II. Obstet. Gynecol. 2016, 128, 1025–1031. [Google Scholar] [CrossRef]
- Moseson, M.; Koenig, K.L.; Shore, R.E.; Pasternack, B.S. The influence of medical conditions associated with hormones on the risk of breast cancer. Int. J. Epidemiol. 1993, 22, 1000–1009. [Google Scholar] [CrossRef] [PubMed]
- Venn, A.; Watson, L.; Bruinsma, F.; Giles, G.; Healy, D. Risk of cancer after use of fertility drugs with in-vitro fertilisation. Lancet 1999, 354, 1586–1590. [Google Scholar] [CrossRef] [PubMed]
- Weiss, H.A.; Brinton, L.A.; Potischman, N.A.; Brogan, D.; Coates, R.J.; Gammon, M.D.; Malone, K.E.; Schoenberg, J.B. Breast cancer risk in young women and history of selected medical conditions. Int. J. Epidemiol. 1999, 28, 816–823. [Google Scholar] [CrossRef] [PubMed]
- Baron, J.A.; Weiderpass, E.; Newcomb, P.A.; Stampfer, M.; Titus-Ernstoff, L.; Egan, K.M.; Greenberg, E.R. Metabolic disorders and breast cancer risk (United States). Cancer Causes Control 2001, 12, 875–880. [Google Scholar] [CrossRef] [PubMed]
- Olson, J.E.; Cerhan, J.R.; Janney, C.A.; Anderson, K.E.; Vachon, C.M.; Sellers, T.A. Postmenopausal cancer risk after self-reported endometriosis diagnosis in the Iowa Women’s Health Study. Cancer 2002, 94, 1612–1618. [Google Scholar] [CrossRef]
- Bertelsen, L.; Mellemkjaer, L.; Frederiksen, K.; Kjaer, S.K.; Brinton, L.A.; Sakoda, L.C.; van Valkengoed, I.; Olsen, J.H. Risk for breast cancer among women with endometriosis. Int. J. Cancer 2007, 120, 1372–1375. [Google Scholar] [CrossRef] [PubMed]
- Melin, A.; Sparén, P.; Bergqvist, A. The risk of cancer and the role of parity among women with endometriosis. Hum. Reprod. 2007, 22, 3021–3026. [Google Scholar] [CrossRef] [PubMed]
- Nichols, H.B.; Visvanathan, K.; Newcomb, P.A.; Hampton, J.M.; Egan, K.M.; Titus-Ernstoff, L.; Trentham-Dietz, A. Bilateral oophorectomy in relation to risk of postmenopausal breast cancer: Confounding by nonmalignant indications for surgery? Am. J. Epidemiol. 2011, 173, 1111–1120. [Google Scholar] [CrossRef]
- Morales, L.; Alvarez-Garriga, C.; Matta, J.; Ortiz, C.; Vergne, Y.; Vargas, W.; Acosta, H.; Ramírez, J.; Perez-Mayoral, J.; Bayona, M. Factors associated with breast cancer in Puerto Rican women. J. Epidemiol. Glob. Health 2013, 3, 205–215. [Google Scholar] [CrossRef]
- Brinton, L.A.; Gridley, G.; Persson, I.; Baron, J.; Bergqvist, A. Cancer risk after a hospital discharge diagnosis of endometriosis. Am. J. Obstet. Gynecol. 1997, 176, 572–579. [Google Scholar] [CrossRef] [PubMed]
- Chuang, S.C.; Wu, G.J.; Lu, Y.S.; Lin, C.H.; Hsiung, C.A. Associations between Medical Conditions and Breast Cancer Risk in Asians: A Nationwide Population-Based Study in Taiwan. PLoS ONE 2015, 10, e0143410. [Google Scholar] [CrossRef] [PubMed]
- Mogensen, J.B.; Kjær, S.K.; Mellemkjær, L.; Jensen, A. Endometriosis and risks for ovarian, endometrial and breast cancers: A nationwide cohort study. Gynecol. Oncol. 2016, 143, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Saraswat, L.; Ayansina, D.; Cooper, K.G.; Bhattacharya, S.; Horne, A.W.; Bhattacharya, S. Impact of endometriosis on risk of further gynaecological surgery and cancer: A national cohort study. BJOG 2018, 125, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Schairer, C.; Persson, I.; Falkeborn, M.; Naessen, T.; Troisi, R.; Brinton, L.A. Breast cancer risk associated with gynecologic surgery and indications for such surgery. Int. J. Cancer 1997, 70, 150–154. [Google Scholar] [CrossRef]
- Eoh, K.J.; Han, M.; Kim, E.H.; Jung, I.; Kim, Y.T. Markedly increased risk of malignancies in women with endometriosis. Gynecol. Oncol. 2021, 161, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Dahiya, A.; Sebastian, A.; Thomas, A.; George, R.; Thomas, V.; Peedicayil, A. Endometriosis and malignancy: The intriguing relationship. Int. J. Gynaecol. Obstet. 2021, 155, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Brinton, L.A.; Westhoff, C.L.; Scoccia, B.; Lamb, E.J.; Althuis, M.D.; Mabie, J.E.; Moghissi, K.S. Causes of infertility as predictors of subsequent cancer risk. Epidemiology 2005, 16, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Gemmill, J.A.; Stratton, P.; Cleary, S.D.; Ballweg, M.L.; Sinaii, N. Cancers, infections, and endocrine diseases in women with endometriosis. Fertil. Steril. 2010, 94, 1627–1631. [Google Scholar] [CrossRef]
- Matta, J.L.; Flores, I.; Morales, L.M.; Monteiro, J.; Alvarez-Garriga, C.; Bayona, M. Women with endometriosis have a higher DNA repair capacity and diminished breast cancer risk. Mol. Cancer Biol. 2013. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4248303/ (accessed on 12 March 2024).
- Gremke, N.; Griewing, S.; Göhring, J.; Isselhard, A.; Wagner, U.; Kostev, K.; Kalder, M. Is there an association between endometriosis and subsequent breast cancer? A retrospective cohort study from Germany. Breast Cancer Res. Treat. 2023, 204, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Kok, V.C.; Tsai, H.J.; Su, C.F.; Lee, C.K. The Risks for Ovarian, Endometrial, Breast, Colorectal, and Other Cancers in Women with Newly Diagnosed Endometriosis or Adenomyosis: A Population-Based Study. Int. J. Gynecol. Cancer 2015, 25, 968–976. [Google Scholar] [CrossRef]
- Ren, W.; Chen, M.; Qiao, Y.; Zhao, F. Global guidelines for breast cancer screening: A systematic review. Breast 2022, 64, 85–99. [Google Scholar] [CrossRef]
- Becker, C.M.; Bokor, A.; Heikinheimo, O.; Horne, A.; Jansen, F.; Kiesel, L.; King, K.; Kvaskoff, M.; Nap, A.; Petersen, K.; et al. ESHRE guideline: Endometriosis. Hum. Reprod. Open 2022, 2022, hoac009. [Google Scholar] [CrossRef] [PubMed]
- Practice Committee of the American Society for Reproductive Medicine. Definitions of infertility and recurrent pregnancy loss: A committee opinion. Fertil. Steril. 2013, 99, 63. [Google Scholar] [CrossRef] [PubMed]
- Guerriero, S.; Condous, G.; van den Bosch, T.; Valentin, L.; Leone, F.P.; Van Schoubroeck, D.; Exacoustos, C.; Installé, A.J.; Martins, W.P.; Abrao, M.S.; et al. Systematic approach to sonographic evaluation of the pelvis in women with suspected endometriosis, including terms, definitions and measurements: A consensus opinion from the International Deep Endometriosis Analysis (IDEA) group. Ultrasound Obstet. Gynecol. 2016, 48, 318–332. [Google Scholar] [CrossRef]
- Exacoustos, C.; Malzoni, M.; Di Giovanni, A.; Lazzeri, L.; Tosti, C.; Petraglia, F.; Zupi, E. Ultrasound mapping system for the surgical management of deep infiltrating endometriosis. Fertil. Steril. 2014, 102, 143–150. [Google Scholar] [CrossRef]
- Van Holsbeke, C.; Van Calster, B.; Guerriero, S.; Savelli, L.; Paladini, D.; Lissoni, A.A.; Czekierdowski, A.; Fischerova, D.; Zhang, J.; Mestdagh, G.; et al. Endometriomas: Their ultrasound characteristics. Ultrasound Obstet. Gynecol. 2010, 35, 730–740. [Google Scholar] [CrossRef]
- Harmsen, M.J.; Van den Bosch, T.; de Leeuw, R.A.; Dueholm, M.; Exacoustos, C.; Valentin, L.; Hehenkamp, W.J.K.; Groenman, F.; De Bruyn, C.; Rasmussen, C.; et al. Consensus on revised definitions of Morphological Uterus Sonographic Assessment (MUSA) features of adenomyosis: Results of modified Delphi procedure. Ultrasound Obstet. Gynecol. 2022, 60, 118–131. [Google Scholar] [CrossRef]
- Giuliano, A.E.; Edge, S.B.; Hortobagyi, G.N. Eighth Edition of the AJCC Cancer Staging Manual: Breast Cancer. Ann Surg Oncol. 2018, 25, 1783–1785. [Google Scholar] [CrossRef]
- Curigliano, G.; Burstein, H.J.; Winer, E.P.; Gnant, M.; Dubsky, P.; Loibl, S.; Colleoni, M.; Regan, M.M.; Piccart-Gebhart, M.; Senn, H.J.; et al. De-escalating and escalating treatments for early-stage breast cancer: The St. Gallen International Expert Consensus Conference on the Primary Therapy of Early Breast Cancer 2017. Ann Oncol. 2017, 28, 1700–1712. [Google Scholar] [CrossRef] [PubMed]
- Ness, R.B.; Modugno, F. Endometriosis as a model for inflammation-hormone interactions in ovarian and breast cancers. Eur. J. Cancer 2006, 42, 691–703. [Google Scholar] [CrossRef] [PubMed]
- Buonomo, O.C.; Vanni, G.; Mainolfi, M.; Materazzo, M.; Pellicciaro, M.; Papi, S.; Combi, F.; Tazzioli, G. Telehealth in oncofertility and breast cancer patients during COVID-19: Preliminary results of insenoallasalute.it project. Eur. Rev. Med. Pharmacol. Sci. 2023, 27, 5327–5337. [Google Scholar] [CrossRef] [PubMed]
- Ruddy, K.J.; Vierkant, R.A.; Jahan, N.; Higgins, A.; Partridge, A.; Larson, N.; Radisky, D.C.; Couch, F.; Olson, J.; Sherman, M.E. Reproductive risk factors associated with breast cancer in young women by molecular subtype. Breast 2022, 66, 272–277. [Google Scholar] [CrossRef]
- Radecka, B.; Litwiniuk, M. Breast cancer in young women. Ginekol. Pol. 2016, 87, 659–663. [Google Scholar] [CrossRef] [PubMed]
- Nimbalkar, V.P.; Rajarajan, S.; VP, S.; Alexander, A.; Kaluve, R.; Selvam, S.; Ramesh, R.; BS, S.; Prabhu, J.S. A comparative analysis of clinicopathological features and survival between pre and postmenopausal breast cancer from an Indian cohort. Sci. Rep. 2023, 13, 3938. [Google Scholar] [CrossRef]
- Govind Babu, K.; Anand, A.; Lakshmaiah, K.C.; Lokanatha, D.; Jacob, L.A.; Suresh Babu, M.C.; Lokesh, K.N.; Rudresha, H.A.; Rajeev, L.K.; Saldanha, S.C.; et al. Correlation of BMI with breast cancer subtype and tumour size. Ecancermedicalscience 2018, 12, 845. [Google Scholar] [CrossRef]
- Iyengar, N.M.; Gucalp, A.; Dannenberg, A.J.; Hudis, C.A. Obesity and Cancer Mechanisms: Tumor Microenvironment and Inflammation. J. Clin. Oncol. 2016, 34, 4270–4276. [Google Scholar] [CrossRef]
- Shah, R.; Rosso, K.; Nathanson, S.D. Pathogenesis, prevention, diagnosis and treatment of breast cancer. World J. Clin. Oncol. 2014, 5, 283–298. [Google Scholar] [CrossRef]
- Vanni, G.; Materazzo, M.; Pellicciaro, M.; Morando, L.; Portarena, I.; Anemona, L.; D’Angelillo, M.R.; Barbarino, R.; Chiaravalloti, A.; Meucci, R.; et al. Does Age Matter? Estimating Risks of Locoregional Recurrence After Breast-conservative Surgery. In Vivo 2020, 34, 1125–1132. [Google Scholar] [CrossRef]
- Buonomo, O.C.; Caredda, E.; Portarena, I.; Vanni, G.; Orlandi, A.; Bagni, C.; Petrella, G.; Palombi, L.; Orsaria, P. New insights into the metastatic behavior after breast cancer surgery, according to well-established clinicopathological variables and molecular subtypes. PLoS ONE 2017, 12, e0184680. [Google Scholar] [CrossRef]
- Vanni, G.; Materazzo, M.; Pellicciaro, M.; Tacconi, F.; Faccini, B.A.; Longo, B.; Cervelli, V.; Buonomo, O.C. Breast cancer treatment de-escalation: Breaking the SOUND barrier. WCRJ 2023, 10, e2682. [Google Scholar] [CrossRef]
- Crabb, S.J.; Cheang, M.C.; Leung, S.; Immonen, T.; Nielsen, T.O.; Huntsman, D.D.; Bajdik, C.D.; Chia, S.K. Basal breast cancer molecular subtype predicts for lower incidence of axillary lymph node metastases in primary breast cancer. Clin. Breast Cancer 2008, 8, 249–256. [Google Scholar] [CrossRef]
- Gentilini, O.D.; Botteri, E.; Sangalli, C.; Galimberti, V.; Porpiglia, M.; Agresti, R.; Luini, A.; Viale, G.; Cassano, E.; Peradze, N.; et al. Sentinel Lymph Node Biopsy vs No Axillary Surgery in Patients with Small Breast Cancer and Negative Results on Ultrasonography of Axillary Lymph Nodes: The SOUND Randomized Clinical Trial. JAMA Oncol. 2023, 9, 1557–1564. [Google Scholar] [CrossRef]


{kind=link}
| Overall Population (n= 123) | Premenopausal Group (n= 90) | Postmenopausal Group (n= 33) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| BC+ EN+ Group (n = 41) | BC+ EN- Group (n = 82) | p-Value | BC+ EN+ Group (n = 30) | BC+ EN- Group (n = 60) | p-Value | BC+ EN+ Group (n = 11) | BC+ EN- Group (n = 22) | p-Value | |
| Age at breast cancer diagnosis (y) mean ± SD | 46.5 ± 7.3 | 46.1 ± 7.5 | 0.699 | 42.7 ± 5.0 | 43.4 ± 4.7 | 0.699 | 53.5 ± 6.6 | 54.6 ± 6.8 | 0.641 |
| BMI (kg/m2) mean ± SD | 21.4 ± 3.0 | 22.2 ± 3 | 0.525 | 22.3 ± 3.0 | 23.0 ± 4.0 | 0.521 | 22.0 ± 2.0 | 23.0 ± 3.1 | 0.116 |
| Age at menarche (yrs) mean ± SD | 12.1 ± 1.2 | 12.3 ± 1.5 | 0.310 | 12.1 ± 1.0 | 12.2 ± 1.2 | 0.627 | 12.0 ± 1.1 | 12.2 ± 1.2 | 0.984 |
| Previous hormonal treatment n (%) | 31 (76.0%) | 37 (45.0%) | 0.002 * | 14 (48.0%) | 1 (2.0%) | <0.001 * | 7 (64.0%) | 2 (9.0%) | 0.002 * |
| Pelvic surgery n (%) | 21 (53.0%) | 3 (4.0%) | <0.001 * | 9 (30.0%) | 4 (7.0%) | 0.001 * | 2 (18.0%) | 0 (0%) | 0.104 |
| Infertility n (%) | 11 (27.0%) | 4 (5.0%) | 0.001 * | 14 (47.0%) | 10 (17.0%) | 0.004 * | 2 (18.0%) | 3 (14.0%) | 1.000 |
| Nulliparous n (%) | 16 (39.0%) | 13 (16.0%) | 0.006 * | 14 (47.0%) | 10 (17.0%) | 0.004 * | 2 (18.0%) | 3 (14.0%) | 1.000 |
| Overall Population (n = 123) | Premenopausal Group (n = 90) | Postmenopausal Group (n = 33) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| BC+ EN+ Group (n = 41) | BC+ EN− Group (n = 82) | p-Value | BC+ EN+ Group (n = 30) | BC+ EN− Group (n = 60) | p-Value | BC+ EN+ Group (n = 11) | BC+ EN− Group (n = 22) | p-Value | |
| Dimension (cm) mean ± SD | 1.4 ± 1.2 | 2.0 ± 1.5 | 0.043 * | 1.5 ± 1.2 | 2.1 ± 1.7 | 0.049 * | 1.3 ± 1.0 | 1.6 ± 1.0 | 0.323 |
| Macrometastatic SLNB n (%) | 4 (9.8%) | 39 (47.6%) | <0.001 * | 2 (6.7%) | 31 (51.7%) | <0.001 * | 2 (18.2%) | 8 (36.4%) | 0.430 |
| pT n(%) | |||||||||
| pT1a | 5 (12.2%) | 5 (6.1%) | 0.036 * | 3 (10.0%) | 3 (5.0%) | 0.042 * | 2 (9.1%) | 2 (18.2%) | 0.386 |
| pT1b | 14 (11.4%) | 11 (8.9%) | 11 (36.7%) | 8 (13.3%) | 3 (27.3%) | 3 (13.6%) | |||
| pT1c | 12 (29.3%) | 32 (39.0%) | 9 (30.0%) | 19 (31.7%) | 3 (27.3%) | 13 (59.1%) | |||
| pT2 | 10 (24.4%) | 31 (37.8%) | 7 (23.3%) | 27 (45.0%) | 3 (27.3%) | 4 (18.2%) | |||
| pT3 | 0 (0.0%) | 3 (3.7%) | 0 (0.0%) | 3 (5.0%) | 3 (27.3%) | 4 (18.2%) | |||
| pN n (%) | |||||||||
| pN0 | 37 (90.2%) | 45 (54.9%) | <0.001 * | 28 (93.3%) | 29 (48.3%) | <0.001 * | 9 (81.8%) | 16 (72.7%) | 0.455 |
| pN1a | 2 (4.9%) | 27 (32.9%) | 1 (3.3%) | 22 (36.7%) | 1 (9.1%) | 5 (22.7%) | |||
| pN1b | 1 (2.4%) | 1 (1.2%) | 0 (0.0%) | 1 (1.7%) | 1 (9.1%) | 0 (0.0%) | |||
| pN2a | 0 (0.0%) | 5 (6.1%) | 0 (0.0%) | 5 (8.3%) | 0 (0.0%) | 0 (0.0%) | |||
| pN2b | 0 (0.0%) | 1 (1.2%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (4.5%) | |||
| pN3 | 1 (2.4%) | 3 (3.7%) | 1 (3.3%) | 3 (5.0%) | 0 (0.0%) | 0 (0.0%) | |||
| Histology n (%) | |||||||||
| Invasive Lobular | 9 (21.95%) | 11 (13.4%) | 0.299 | 7 (23.3%) | 7 (11.7%) | 0.216 | 2 (18.2%) | 4 (18.2%) | 1.000 |
| Invasive Ductal | 32 (78.04%) | 71 (86.6%) | 23 (73.3%) | 53 (88.3%) | 9 (81.8%) | 18 (81.8%) | |||
| Hormonal Expression n (%) | |||||||||
| ER+/PR− | 3 (7.3%) | 8 (9.8%) | 0.226 | 3 (10%) | 5 (8.3%) | 0.925 | 0 (0.0%) | 3 (13.6%) | 0.555 |
| ER+/PR+ | 36 (87.8%) | 62 (75.6%) | 25 (83.3%) | 47 (78.3%) | 11 (100%) | 15 (68.2%) | |||
| ER-/PR− | 2 (4.9%) | 12 (13.4%) | 2 (6.7%) | 8 (13.3%) | 0 (0.0%) | 4 (13.6%) | |||
| ER % mean ± SD | 83.2 ± 21.2 | 70.1 ± 34.0 | 0.010 | 82.5 ± 24.2 | 69.3 ± 32.9 | 0.035 | 85.0 ± 9.48 | 72.0 ± 37.4 | 0.139 |
| PR % mean ± SD | 54.3 ± 35.5 | 59.1 ± 39.2 | 0.505 | 56.2 ± 36.6 | 62.6 ± 39.1 | 0.457 | 49.1 ± 33.4 | 49.7 ± 38.7 | 0.961 |
| HER 2+ n (%) | 4 (9.8%) | 23 (28.0%) | 0.022 | 2 (6.7%) | 20 (33.3%) | 0.001 | 2 (18.1%) | 3 (13.6%) | 0.375 |
| KI67 % mean ± SD | 14.8 ± 10.4 | 24.4 ± 18.7 | <0.001 | 14.4 ± 10.1 | 26.4 ± 19.6 | <0.001 | 16.0 ± 11.0 | 18.0 ± 14.0 | 0.626 |
| Immunohistochemical subtypes n (%) | |||||||||
| Luminal A | 30 (73.2%) | 33 (40.2%) | 0.017 | 22 (73.3%) | 23 (38.3%) | 0.018 | 8 (72.7%) | 10 (45.5%) | 0.371 |
| Luminal B (Her 2−) | 5 (12.2%) | 17 (20.7%) | 4 (13.3%) | 12 (20.0%) | 1 (9.1%) | 5 (22.7%) | |||
| Luminal B (Her 2+) | 4 (9.8%) | 19 (23.2%) | 2 (6.7%) | 17 (28.3%) | 2 (18.2%) | 2 (9%) | |||
| Her 2+ | 0 | 4 (4.9%) | 0 | 3 (5.0%) | 0 | 1 (4.5%) | |||
| Triple − | 2 (4.9%) | 9 (11%) | 2 (6.7%) | 5 (8.3%) | 0 | 4 (18.2%) | |||
| Grading n (%) | |||||||||
| G1 | 18 (43.9%) | 12 (14.6%) | <0.001 | 15 (50.0%) | 8 (13.3%) | <0.001 | 3 (27.3%) | 4 (18.2%) | 0.288 |
| G2 | 20 (48.8%) | 40 (48.8%) | 12 (40.0%) | 27 (45.0%) | 8 (72.7%) | 13 (59.1%) | |||
| G3 | 3 (7.3%) | 30 (36.6%) | 3 (10.0%) | 25 (41.7%) | 0 | 5 (22.7%) | |||
| Overall Population (n = 123) | ||||
| OR | Sign. | Wald | 95%CI | |
| Age at breast cancer diagnosis | 0.816 | 0.040 | 4.199 | 0.671–0.991 |
| Age at menopause | 1.925 | 0.270 | 0.998 | 0.532–6.961 |
| Hormonal therapy | 0.501 | 0.107 | 2.592 | 0.216–1.162 |
| Endometriosis | 3.203 | 0.012 | 6.240 | 1.285–7.986 |
| Premenopausal Group (n = 90) | ||||
| OR | Sign. | Wald | 95%CI | |
| Age at breast cancer diagnosis | 0.822 | 0.325 | 0.969 | 0.556–1.215 |
| Age at menopause | 1.103 | 0.605 | 0.267 | 0.761–1.599 |
| Hormonal therapy | 0.568 | 0.243 | 1.363 | 0.220–1.468 |
| Endometriosis | 3.882 | 0.012 | 6.368 | 1.354–11.135 |
| Postmenopausal Group (n = 33) | ||||
| OR | Sign. | Wald | 95%CI | |
| Age at breast cancer diagnosis | 0.803 | 0.166 | 1.921 | 0.589–1.095 |
| Age at menopause | 1.138 | 0.493 | 0.470 | 0.787–1.645 |
| Hormonal therapy | 0.332 | 0.252 | 1.310 | 0.050–2.197 |
| Endometriosis | 1.772 | 0.556 | 0.347 | 0.264–11.884 |
| Premenopausal Group (n = 90) | |||
|---|---|---|---|
| BC+EN+ Group (n = 30) | BC-EN+ Group (n = 60) | p-Value | |
| Age (y) mean ± SD | 42.7 ± 5.0 | 42.1 ± 5.5 | 0.617 |
| BMI (kg/m2) mean ± SD | 22.3 ± 6.0 | 22.6 ± 4.2 | 0.778 |
| Age at Menarche (y) mean ± SD | 12.2 ± 1.1 | 12.6 ± 1.6 | 0.230 |
| Previous hormonal treatment n (%) | 23 (77.0%) | 48 (80%) | 0.743 |
| Infertility yes n (%) | 9 (30%) | 18 (30%) | 1.000 |
| ART yes n (%) | 7 (23.0%) | 11 (18%) | 0.576 |
| Nulliparous yes n (%) | 14 (47%) | 25 (58%) | 0.326 |
| Endometriosis type n (%) | |||
| Endometrioma | 16 (53%) | 33 (55%) | 0.850 |
| Posterior DIE | 17 (57%) | 51 (85%) | 0.003 |
| Anterior DIE | 2 (7%) | 2 (3%) | 0.382 |
| Adenomyosis | 13 (43%) | 39 (65%) | 0.048 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vanni, G.; Selntigia, A.; Marsella, V.E.; Russo, C.; Pellicciaro, M.; Materazzo, M.; Rizzo, G.; Buonomo, O.C.; Exacoustos, C. Breast Cancer in Patients with Previous Endometriosis Showed Low Aggressive Subtype. Medicina 2024, 60, 625. https://doi.org/10.3390/medicina60040625
Vanni G, Selntigia A, Marsella VE, Russo C, Pellicciaro M, Materazzo M, Rizzo G, Buonomo OC, Exacoustos C. Breast Cancer in Patients with Previous Endometriosis Showed Low Aggressive Subtype. Medicina. 2024; 60(4):625. https://doi.org/10.3390/medicina60040625
Chicago/Turabian StyleVanni, Gianluca, Aikaterini Selntigia, Valentina Enrica Marsella, Consuelo Russo, Marco Pellicciaro, Marco Materazzo, Giuseppe Rizzo, Oreste Claudio Buonomo, and Caterina Exacoustos. 2024. "Breast Cancer in Patients with Previous Endometriosis Showed Low Aggressive Subtype" Medicina 60, no. 4: 625. https://doi.org/10.3390/medicina60040625