
Can Older Adult Patients with Hip Fractures Have Their Discharge Destination Predicted by Physical Performance Measures?


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Demographic and Disease-Related Characteristics Data
2.3. Performance-Based Physical Function
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cooper, C.; Cole, Z.A.; Holroyd, C.R.; Earl, S.C.; Harvey, N.C.; Dennison, E.M.; Melton, L.J.; Cummings, S.R.; Kanis, J.A.; IOF CSA Working Group on Fracture Epidemiology. Secular trends in the incidence of hip and other osteoporotic fractures. Osteoporos. Int. 2011, 22, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Brauer, C.A.; Coca-Perraillon, M.; Cutler, D.M.; Rosen, A.B. Incidence and mortality of hip fractures in the United States. JAMA 2009, 302, 1573–1579. [Google Scholar] [CrossRef]
- Gjertsen, J.E.; Baste, V.; Fevang, J.M.; Furnes, O.; Engesæter, L.B. Quality of life following hip fractures: Results from the Norwegian hip fracture register. BMC Musculoskelet. Disord. 2016, 17, 265. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.Y.; Graham, J.E.; Karmarkar, A.M.; Reistetter, T.A.; Protas, E.J.; Ottenbacher, K.J. FIM motor scores for classifying community discharge after inpatient rehabilitation for hip fracture. PM&R. 2014, 6, 493–497. [Google Scholar] [CrossRef]
- Hayashi, H.; Iwai, M.; Matsuoka, H.; Nakashima, D.; Nakamura, S.; Kubo, A.; Tomiyama, N. Factors affecting the discharge destination of hip fracture patients who live alone and have been admitted to an inpatients rehabilitation unit. J. Phys. Ther. Sci. 2016, 28, 1228–1232. [Google Scholar] [CrossRef]
- Beckmann, M.; Bruun-Olsen, V.; Pripp, A.H.; Bergland, A.; Smith, T.; Heiberg, K.E. Recovery and prediction of physical function 1 year following hip fracture. Physiother. Res. Int. 2022, 27, e1947. [Google Scholar] [CrossRef]
- Song, Y.J. The South Korean health care system. Jmaj 2009, 52, 206–209. [Google Scholar]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.M.; Sundararajan, V. Updating and validating the Charlson Comorbidity Index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Koval, K.J.; Aharonoff, G.B.; Rosenberg, A.D.; Bernstein, R.L.; Zuckerman, J.D. Functional outcome after hip fracture. Effect of general versus regional anesthesia. Clin. Orthop. Relat. Res. 1998, 348, 37–41. [Google Scholar] [CrossRef]
- Smith, P.S.; Hembree, J.A.; Thompson, M.E. Berg balance scale and functional reach: Determining the best clinical tool for individuals post acute stroke. Clin. Rehabil. 2004, 18, 811–818. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Andrews, A.W.; Thomas, M.W. Walking speed: Reference values and correlates for older adults. J. Orthop. Sports Phys. Ther. 1996, 24, 86–90. [Google Scholar] [CrossRef]
- Freter, S.H.; Fruchter, N. Relationship between timed ‘up and go’ and gait time in an elderly orthopaedic rehabilitation population. Clin. Rehabil. 2000, 14, 96–101. [Google Scholar] [CrossRef]
- Morri, M.; Natali, E.; Tosarelli, D. At discharge gait speed and independence of patients provides a challenges for rehabilitation after total joint arthroplasty: An observational study. Arch. Physiother. 2016, 6, 6. [Google Scholar] [CrossRef]
- Kline Mangione, K.; Craik, R.L.; Lopopolo, R.; Tomlinson, J.D.; Brenneman, S.K. Predictors of gait speed in patients after hip fracture. Physiother. Can. 2008, 60, 10–18. [Google Scholar] [CrossRef]
- Kubota, M.; Uchida, K.; Kokubo, Y.; Shimada, S.; Matsuo, H.; Yayama, T.; Miyazaki, T.; Takeura, N.; Yoshida, A.; Baba, H. Changes in gait pattern and hip muscle strength after open reduction and internal fixation of acetabular fracture. Arch. Phys. Med. Rehabil. 2012, 93, 2015–2021. [Google Scholar] [CrossRef]
- Baudendistel, S.T.; Schmitt, A.C.; Stone, A.E.; Raffegeau, T.E.; Roper, J.A.; Hass, C.J. Faster or longer steps: Maintaining fast walking in older adults at risk for mobility disability. Gait Posture 2021, 89, 86–91. [Google Scholar] [CrossRef]
- Tyler, T.F.; Nicholas, S.J.; Mullaney, M.J.; McHugh, M.P. The role of hip muscle function in the treatment of patellofemoral pain syndrome. Am. J. Sports Med. 2006, 34, 630–636. [Google Scholar] [CrossRef]
- Ganderton, C.; Pizzari, T.; Harle, T.; Cook, J.; Semciw, A. Gluteus medius, gluteus minimus and tensor fascia latae are overactive during gait in post-menopausal women with greater trochanteric pain syndrome. J. Sci. Med. Sport 2017, 20, e72. [Google Scholar] [CrossRef]
- Salarian, A.; Zampieri, C.; Horak, F.B.; Carlson-Kuhta, P.; Nutt, J.G.; Aminian, K. Analyzing 180 degrees turns using an inertial system reveals early signs of progression of Parkinson’s disease. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2009, 2009, 224–227. [Google Scholar] [CrossRef]
- Wu, J.Q.; Mao, L.B.; Wu, J. Efficacy of balance training for hip fracture patients: A meta-analysis of randomized controlled trials. J. Orthop. Surg. Res. 2019, 14, 83. [Google Scholar] [CrossRef]
- Lee, S.Y.; Jung, S.H.; Lee, S.U.; Ha, Y.C.; Lim, J.Y. Effect of Balance Training After Hip Fracture Surgery: A Systematic Review and Meta-analysis of Randomized Controlled Studies. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 74, 1679–1685. [Google Scholar] [CrossRef] [PubMed]
- Parkkari, J.; Kannus, P.; Palvanen, M.; Natri, A.; Vainio, J.; Aho, H.; Vuori, I.; Järvinen, M. Majority of hip fractures occur as a result of a fall and impact on the greater trochanter of the femur: A prospective controlled hip fracture study with 206 consecutive patients. Calcif. Tissue Int. 1999, 65, 183. [Google Scholar] [CrossRef] [PubMed]
- Wolfson, L. Gait and balance dysfunction: A model of the interaction of age and disease. Neuroscientist 2001, 7, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Hillsdon, M.; Foster, C. What are the health benefits of muscle and bone strengthening and balance activities across life stages and specific health outcomes? J. Frailty Sarcopenia Falls 2018, 3, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Bobić Lucić, L.; Grazio, S. Impact of Balance Confidence on Daily Living Activities of Older People with Knee Osteoarthritis with Regard to Balance, Physical Function, Pain, and Quality of Life—A Preliminary Report. Clin. Gerontol. 2018, 41, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Dunsky, A. The Effect of Balance and Coordination Exercises on Quality of Life in Older Adults: A Mini-Review. Front. Aging Neurosci. 2019, 11, 318. [Google Scholar] [CrossRef] [PubMed]
- Proske, U.; Gandevia, S.C. The proprioceptive senses: Their roles in signaling body shape, body position and movement, and muscle force. Physiol. Rev. 2012, 92, 1651–1697. [Google Scholar] [CrossRef] [PubMed]
- Riemen, A.H.; Hutchison, J.D. The multidisciplinary management of hip fractures in older patients. Orthop. Trauma 2016, 30, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Seitz, D.P.; Gill, S.S.; Gruneir, A.; Austin, P.C.; Anderson, G.M.; Bell, C.M.; Rochon, P.A. Effects of dementia on postoperative outcomes of older adults with hip fractures: A population-based study. J. Am. Med. Dir. Assoc. 2014, 15, 334–341. [Google Scholar] [CrossRef]
- Tsuda, Y.; Kawano, H.; Tanaka, S.; Yasunaga, H.; Horiguchi, H.; Ogawa, S. Association between dementia and postoperative complications after hip fracture surgery in the elderly: Analysis of 87,654 patients using a national administrative database. Arch. Orthop. Trauma Surg. 2015, 135, 1511. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | Home Group (n = 99) | Facility Group (n = 51) | p-Value |
|---|---|---|---|
| Age (years) | 77.4 ± 11.6 | 81.1 ± 7.7 | 0.024 * |
| Sex, males/females | 23 (23.2)/76 (76.8) | 8 (15.7)/43 (84.3) | 0.666 |
| BMI (Kg/m2) | 22.4 ± 3.5 | 21.8 ± 4.1 | 0.357 |
| Type of insurance | 0.205 | ||
| Medical aid program | 11 (11.1) | 10 (19.6) | |
| Health insurance program | 88 (88.9) | 41 (80.4) | |
| Fracture side | 0.478 | ||
| Right | 48 (48.5) | 22 (43.1) | |
| Left | 51 (51.5) | 29 (56.9) | |
| Fracture type | 0.234 | ||
| Femur neck | 40 (40.4) | 23 (45.1) | |
| Intertrochateric | 40 (40.4) | 24 (47.1) | |
| Subtrochanteric | 19 (19.2) | 9 (17.6) | |
| Operation type | 0.465 | ||
| Bipolar hemiarthroplasty | 13 (13.1) | 11 (21.6) | |
| Total hip replacement arthroplasty | 20 (20.2) | 11 (21.6) | |
| Reduction and internal fixation | 64 (64.6) | 29 (56.9) | |
| Charlson Comorbidity Index | 2.43 ± 1.32 | 3.02 ± 1.41 | 0.015 * |
| Time from surgery to RM transfer (days) | 21.1 ± 5.7 | 21.8 ± 6.2 | 0.511 |
| Hospitalization period at RM (days) | 11.7 ± 2.9 | 14.0 ± 6.1 | 0.003 ** |
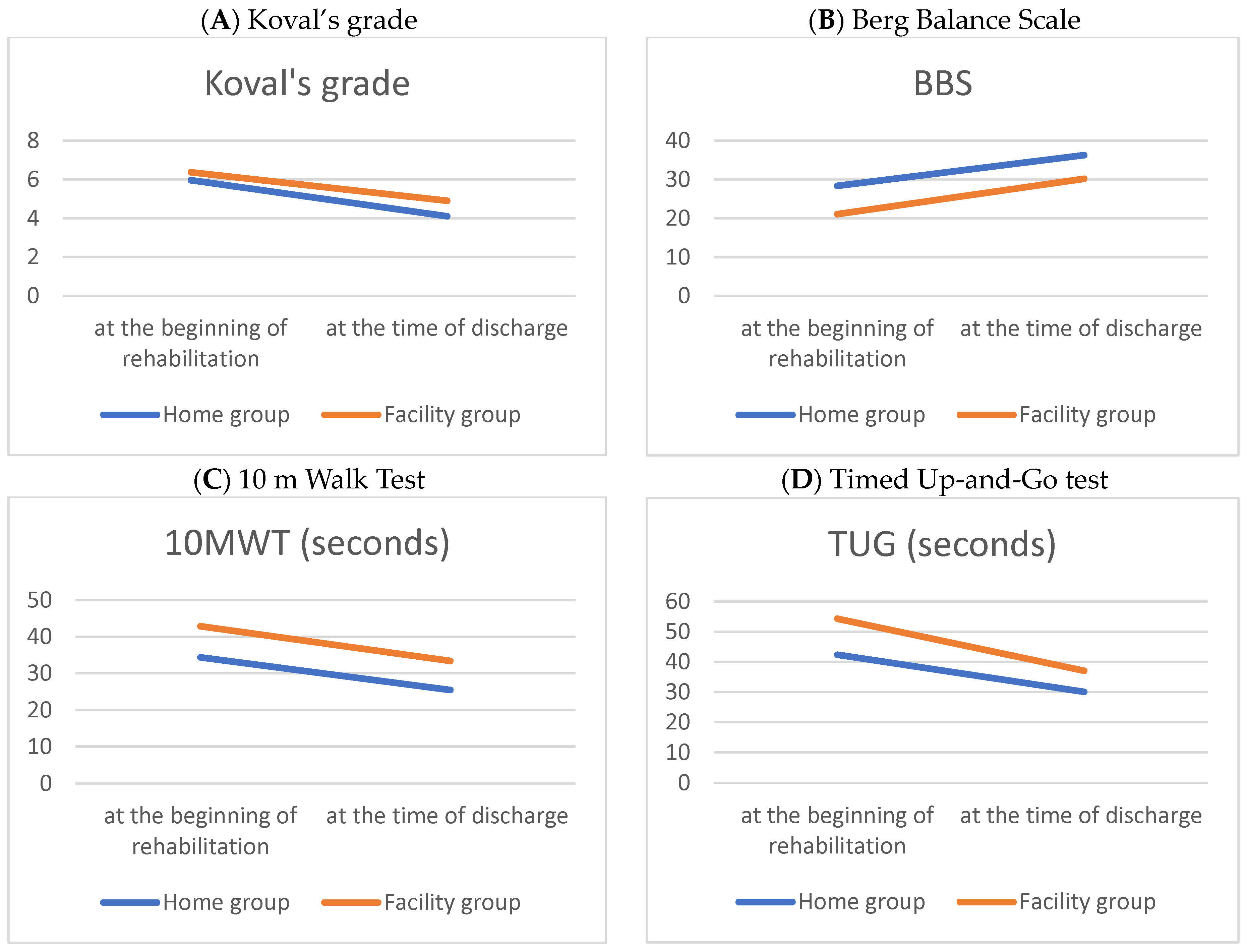
| Variables | Home Group (n = 99) | Facility Group (n = 51) | p-Value |
|---|---|---|---|
| Pre-Koval’s grade | 1.77 ± 1.48 | 2.57 ± 1.80 | 0.009 ** |
| Koval’s grade 1 | 5.96 ± 0.81 | 6.37 ± 0.70 | 0.003 ** |
| BBS 1 | 28.36 ± 13.42 | 21.06 ± 13.55 | 0.003 ** |
| 10MWT (S) 1 | 34.37 ± 20.19 | 42.87 ± 25.99 | 0.005 ** |
| TUG (S) 1 | 42.38 ± 28.69 | 54.31 ± 28.61 | 0.004 ** |
| Koval’s grade 2 | 4.10 ± 1.87 | 4.90 ± 1.51 | 0.001 ** |
| BBS 2 | 36.27 ± 12.21 | 30.18 ± 11.58 | 0.005 ** |
| 10MWT (S) 2 | 25.45 ± 15.60 | 33.40 ± 14.94 | 0.004 ** |
| TUG (S) 2 | 30.07 ± 14.90 | 37.06 ± 14.91 | 0.009 ** |
| Variables | Home Group (n = 99) | Facility Group (n = 51) | p-Value |
|---|---|---|---|
| ΔKoval’s grade | −1.78 ± 1.77 | −1.30 ± 1.39 | 0.163 |
| ΔBBS | 7.91 ± 7.04 | 9.12 ± 8.10 | 0.362 |
| Δ10MWT (S) | −10.50 ± 13.56 | −11.15 ± 25.12 | 0.882 |
| ΔTUG (S) | −13.28 ± 24.50 | −20.37 ± 27.35 | 0.040 * |
| Variables | B | S.E. | Wald | p | Odds Ratio | 95% CI |
|---|---|---|---|---|---|---|
| preKoval’s grade | 0.196 | 0.082 | 5.684 | 0.017 * | 1.309 | 1.035–1.428 |
| BBS (S) 1 | −0.036 | 0.011 | 10.925 | 0.001 ** | 0.965 | 0.944–0.985 |
| 10MWT (S) 1 | 0.026 | 0.009 | 8.905 | 0.003 ** | 1.026 | 1.009–1.043 |
| TUG (S) 1 | 0.016 | 0.005 | 8.278 | 0.004 ** | 1.035 | 1.008–1.058 |
| BBS (S) 2 | −0.039 | 0.014 | 7.345 | 0.007 ** | 0.962 | 0.935–0.989 |
| 10MWT (S) 2 | 0.035 | 0.014 | 6.205 | 0.013 * | 1.036 | 1.007–1.064 |
| TUG (S) 2 | 0.044 | 0.013 | 10.883 | 0.001 ** | 1.045 | 1.018–1.073 |
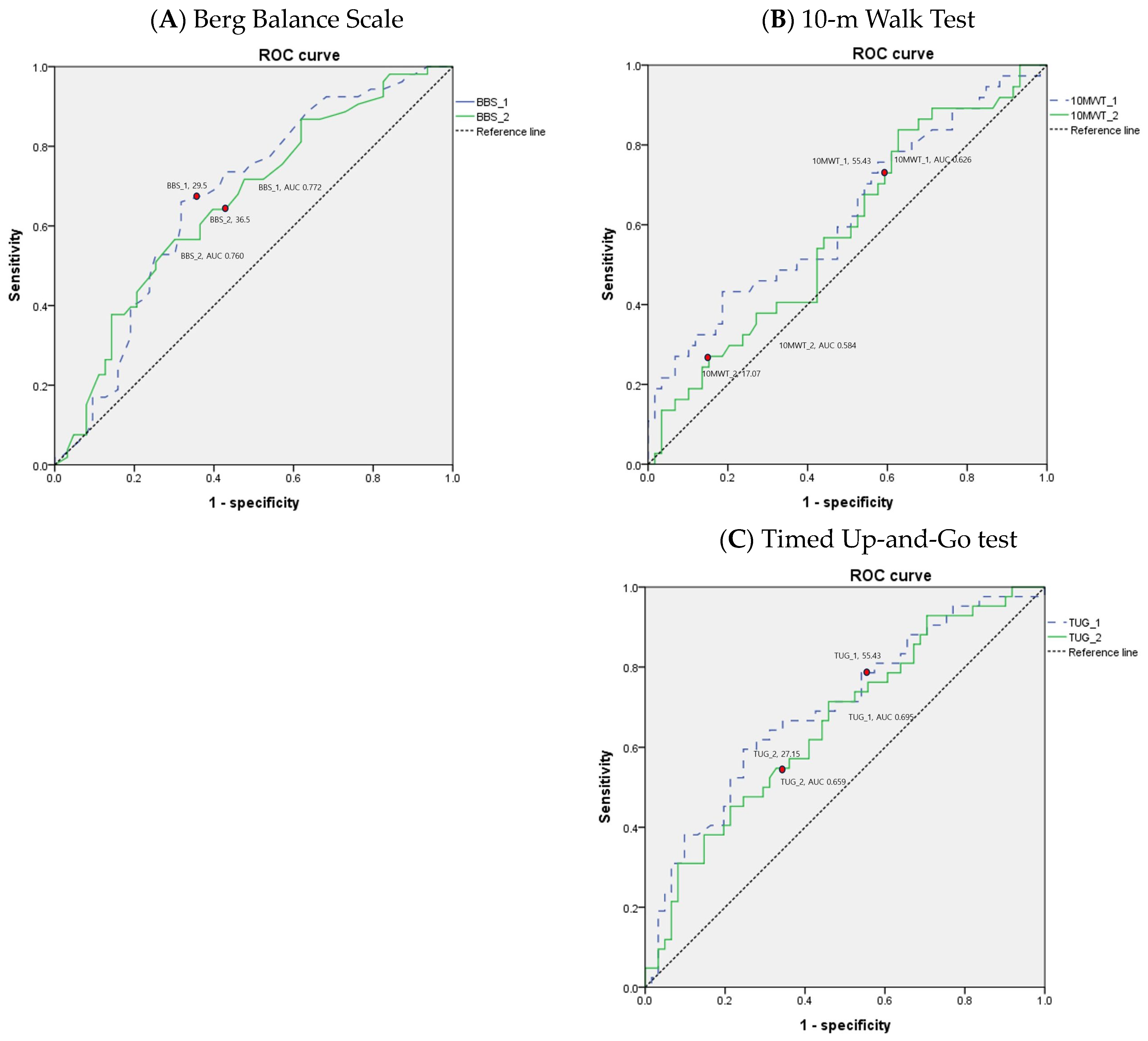
| Variables | Cutoff | Sensitivity (%) | Specificity (%) | AUC | PPV | NPV | p-Value |
|---|---|---|---|---|---|---|---|
| BBS 1 | ≤26 | 64.5 | 60.3 | 0.626 | 54.5 | 69.7 | 0.001 ** |
| BBS 2 | ≤31 | 56.6 | 69.8 | 0.660 | 61.2 | 65.7 | 0.002 ** |
| 10MWT (S) 1 | >53.09 | 33.3 | 87.9 | 0.632 | 62.9 | 68.1 | 0.003 ** |
| 10MWT (S) 2 | >17.03 | 88.2 | 36.1 | 0.648 | 53.6 | 78.6 | 0.005 ** |
| TUG (S) 1 | >55.91 | 55.6 | 76.8 | 0.670 | 60.6 | 72.9 | <0.001 ** |
| TUG (S) 2 | >27.1 | 76.0 | 54.1 | 0.699 | 57.6 | 73.3 | <0.001 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seok, M.-A.; Choi, J.-H.; Roh, Y.-H.; Lee, S.-Y.; Lee, H.-J. Can Older Adult Patients with Hip Fractures Have Their Discharge Destination Predicted by Physical Performance Measures? Medicina 2024, 60, 1017. https://doi.org/10.3390/medicina60071017
Seok M-A, Choi J-H, Roh Y-H, Lee S-Y, Lee H-J. Can Older Adult Patients with Hip Fractures Have Their Discharge Destination Predicted by Physical Performance Measures? Medicina. 2024; 60(7):1017. https://doi.org/10.3390/medicina60071017
Chicago/Turabian StyleSeok, Min-A, Jun-Hwan Choi, Young-Ho Roh, So-Young Lee, and Hyun-Jung Lee. 2024. "Can Older Adult Patients with Hip Fractures Have Their Discharge Destination Predicted by Physical Performance Measures?" Medicina 60, no. 7: 1017. https://doi.org/10.3390/medicina60071017
APA StyleSeok, M.-A., Choi, J.-H., Roh, Y.-H., Lee, S.-Y., & Lee, H.-J. (2024). Can Older Adult Patients with Hip Fractures Have Their Discharge Destination Predicted by Physical Performance Measures? Medicina, 60(7), 1017. https://doi.org/10.3390/medicina60071017