
Intraoperative and Postoperative Outcomes of Pfannenstiel and Midline Skin Incisions in Placenta Accreta Spectrum Disorders: Single-Center Experience
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
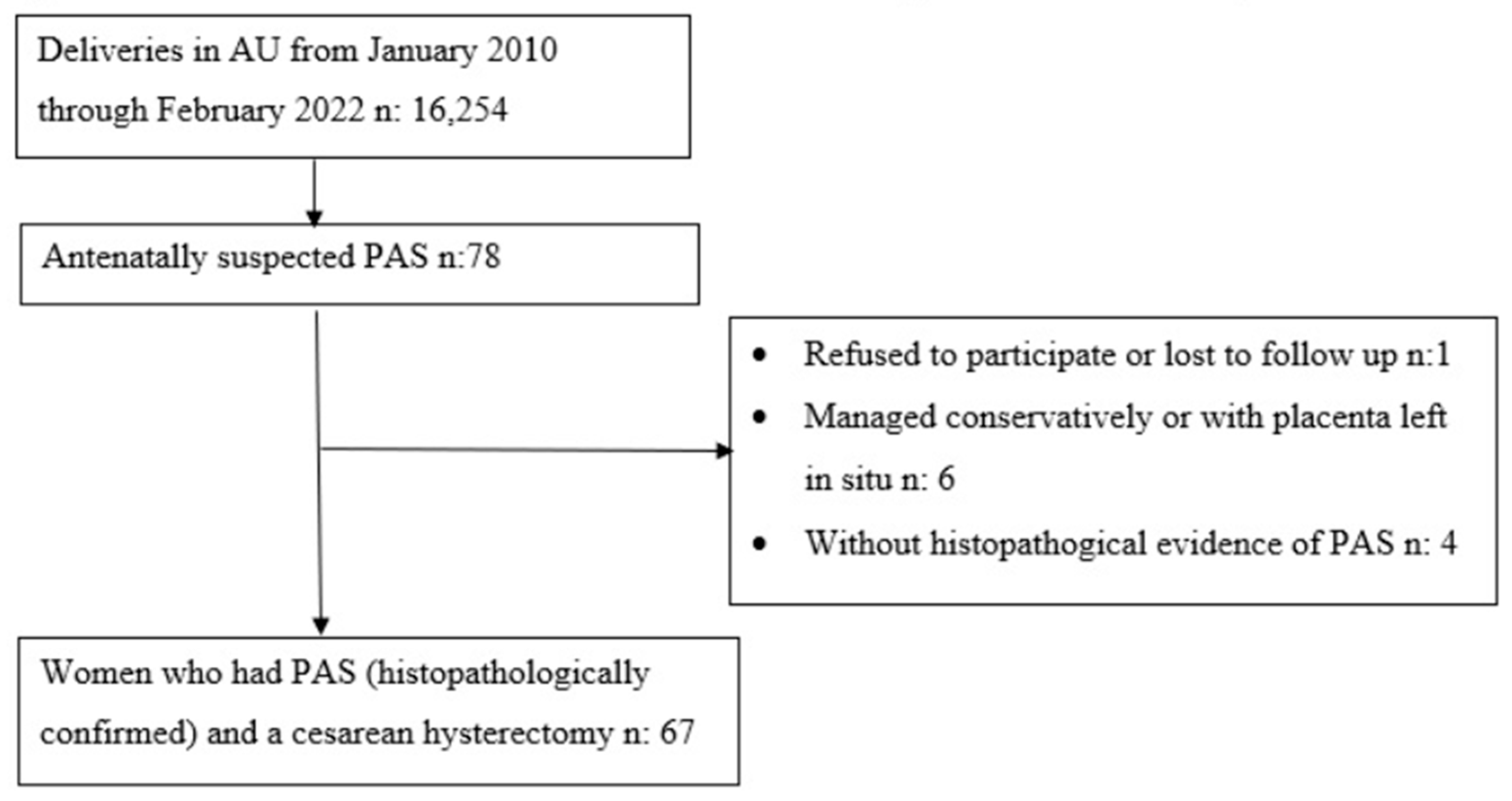
2.1. Study Design and Population
2.2. Data Collection
2.3. Preoperative Management
2.4. Intraoperative and Postoperative Management
2.5. Types of Incisions
2.5.1. Pfannenstiel Group
2.5.2. Midline Group
2.6. Ethical Considerations
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jauniaux, E.; Collins, S.; Burton, G.J. Placenta accreta spectrum: Pathophysiology and evidence-based anatomy for prenatal ultrasound imaging. Am. J. Obstet. Gynecol. 2018, 218, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Einerson, B.D.; Kennedy, A.; Silver, R.M.; Branch, D.W.; Comstock, J.; Woodward, P.J. Ultrasonography of the Explanted Uterus in Placenta Accreta Spectrum: Correlation with Intraoperative Findings and Gross Pathology. Obstet. Gynecol. 2023, 141, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Jauniaux, E.; Chantraine, F.; Silver, R.M.; Langhoff-Roos, J. FIGO consensus guidelines on placenta accreta spectrum disorders: Epidemiology. Int. J. Gynaecol. Obstet. 2018, 140, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Silver, R.M.; Landon, M.B.; Rouse, D.J.; Leveno, K.J.; Spong, C.Y.; Thom, E.A.; Moawad, A.H.; Caritis, S.N.; Harper, M.; Wapner, R.J.; et al. Maternal morbidity associated with multiple repeat cesarean deliveries. Obstet. Gynecol. 2006, 107, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- D’Antonio, F.; Iacovella, C.; Bhide, A. Prenatal identification of invasive placentation using ultrasound: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2013, 42, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Collins, S.L.; Alemdar, B.; van Beekhuizen, H.J.; Bertholdt, C.; Braun, T.; Calda, P.; Delorme, P.; Duvekot, J.J.; Gronbeck, L.; Kayem, G.; et al. Evidence-based guidelines for the management of abnormally invasive placenta: Recommendations from the International Society for Abnormally Invasive Placenta. Am. J. Obstet. Gynecol. 2019, 220, 511–526. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, J.M.; Barton, J.R.; Donaldson, E.S. The management of placenta percreta: Conservative and operative strategies. Am. J. Obstet. Gynecol. 1996, 175, 1632–1638. [Google Scholar] [CrossRef]
- Shamshirsaz, A.A.; Fox, K.A.; Salmanian, B.; Diaz-Arrastia, C.R.; Lee, W.; Baker, B.W.; Ballas, J.; Chen, Q.; Van Veen, T.R.; Javadian, P.; et al. Maternal morbidity in patients with morbidly adherent placenta treated with and without a standardized multidisciplinary approach. Am. J. Obstet. Gynecol. 2015, 212, 218.e1–218.e9. [Google Scholar] [CrossRef] [PubMed]
- Stanleigh, J.; Michaeli, J.; Armon, S.; Khatib, F.; Zuckerman, B.; Shaya, M.; Ioscovitch, A.; Shenfeld, O.; Greenblat, D.; Farkash, R.; et al. Maternal and neonatal outcomes following a proactive peripartum multidisciplinary management protocol for placenta creta spectrum as compared to the urgent delivery. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 237, 139–144. [Google Scholar] [CrossRef]
- Crocetto, F.; Esposito, R.; Saccone, G.; Della Corte, L.; Sarno, L.; Morlando, M.; Maruotti, G.M.; Migliorini, S.; D’alessandro, P.; Arduino, B.; et al. Use of routine ureteral stents in cesarean hysterectomy for placenta accreta. J. Matern.-Fetal Neonatal Med. 2021, 34, 386–389. [Google Scholar] [CrossRef]
- D’antonio, F.; Iacovelli, A.; Liberati, M.; Leombroni, M.; Murgano, D.; Cali, G.; Khalil, A.; Flacco, M.E.; Scutiero, G.; Iannone, P.; et al. Role of interventional radiology in pregnancy complicated by placenta accreta spectrum disorder: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2019, 53, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.; Jauniaux, E.; Hobson, S.; Papillon-Smith, J.; Belfort, M.A. FIGO consensus guidelines on placenta accreta spectrum disorders: Nonconservative surgical management. Int. J. Gynaecol. Obstet. 2018, 140, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Szlachta-McGinn, A.; Mei, J.; Tabsh, K.; Afshar, Y. Transverse versus vertical skin incision for planned cesarean hysterectomy: Does it matter? BMC Pregnancy Childbirth 2020, 20, 65. [Google Scholar] [CrossRef] [PubMed]
- Soyer-Caliskan, C.; Celik, S.; Basbug, A.; Hatirnaz, S.; Guclu, M.; Akbaba, E.; Celik, H.; Guleryuz, S.; Tinelli, A. Morbidly adherent placenta and cesarean section methods. A retrospective comparative multicentric study on two different skin and uterine incision. Ginekol. Pol. 2021, 92, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Akbaba, E. Can high transverse skin incision (Modified Maylard) be a new alternative in placenta accreta spectrum management with cesarean hysterectomy? CEOG 2021, 48, 686–690. [Google Scholar]
- Sentilhes, L.; Seco, A.; Azria, E.; Beucher, G.; Bonnet, M.-P.; Branger, B.; Carbillon, L.; Chiesa, C.; Crenn-Hebert, C.; Dreyfus, M.; et al. Conservative management or cesarean hysterectomy for placenta accreta spectrum: The PACCRETA prospective study. Am. J. Obstet. Gynecol. 2022, 226, 839.e1–839.e24. [Google Scholar] [CrossRef] [PubMed]
- Silver, R.M.; Fox, K.A.; Barton, J.R.; Abuhamad, A.Z.; Simhan, H.; Huls, C.K.; Belfort, M.A.; Wright, J.D. Center of excellence for placenta accreta. Am. J. Obstet. Gynecol. 2015, 212, 561–568. [Google Scholar] [CrossRef]
- Cheng, H.; Clymer, J.W.; Chen, B.P.H.; Sadeghirad, B.; Ferko, N.C.; Cameron, C.G.; Hinoul, P. Prolonged operative duration is associated with complications: A systematic review and meta-analysis. J. Surg. Res. 2018, 229, 134–144. [Google Scholar] [CrossRef]
- Wylie, B.J.; Gilbert, S.; Landon, M.B.; Spong, C.Y.; Rouse, D.J.; Leveno, K.J.; Varner, M.W.; Caritis, S.N.; Meis, P.J.; Wapner, R.J.; et al. Comparison of transverse and vertical skin incision for emergency cesarean delivery. Obstet. Gynecol. 2010, 115, 1134–1140. [Google Scholar] [CrossRef]
- Camuzcuoglu, A.; Vural, M.; Hilali, N.G.; Incebiyik, A.; Yuce, H.H.; Kucuk, A.; Camuzcuoglu, H. Surgical management of 58 patients with placenta praevia percreta. Wien. Klin. Wochenschr. 2016, 128, 360–366. [Google Scholar] [CrossRef]
- Wax, J.R.; Pinette, M.G.; Cartin, A.; Blackstone, J. Gravid uterus exteriorization at cesarean delivery for prenatally diagnosed placenta previa-accreta. Am. J. Perinatol. 2004, 21, 311–313. [Google Scholar] [CrossRef] [PubMed]
- Rauf, M.; Ebru, C.; Sevil, E.; Selim, B. Conservative management of post-partum hemorrhage secondary to placenta previa–accreta with hypogastric artery ligation and endo-uterine hemostatic suture. J. Obstet. Gynaecol. Res. 2017, 43, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.R.; Goodfellow, P.B. Transverse verses midline incisions for abdominal surgery. Cochrane Database Syst. Rev. 2005, 2005, CD005199. [Google Scholar] [PubMed]
- Raghavan, R.; Arya, P.; Arya, P.; China, S. Abdominal incisions and sutures in obstetrics and gynaecology. Obstet. Gynaecol. 2014, 16, 13–18. [Google Scholar] [CrossRef]
- Hempel, S.; Kalauch, A.; Oehme, F.; Wolk, S.; Welsch, T.; Weitz, J.; Distler, M. Wound complications after primary and repeated midline, transverse and modified Makuuchi incision: A single-center experience in 696 patients. Medicine 2021, 100, e25989. [Google Scholar] [CrossRef] [PubMed]
- Seiler, C.M.; Deckert, A.; Diener, M.K.; Knaebel, H.P.; Weigand, M.A.; Victor, N.; Büchler, M.W. Midline versus transverse incision in major abdominal surgery: A randomized, double-blind equivalence trial (POVATI: ISRCTN60734227). Ann. Surg. 2009, 249, 913–920. [Google Scholar] [CrossRef] [PubMed]
- Proske, J.M.; Zieren, J.; Müller, J.M. Transverse versus midline incision for upper abdominal surgery. Surg. Today 2005, 35, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Halm, J.A.; Lip, H.; Schmitz, P.I.; Jeekel, J. Incisional hernia after upper abdominal surgery: A randomised controlled trial of midline versus transverse incision. Hernia 2009, 13, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Luthra, G.; Gawade, P.; Starikov, R.; Markenson, G. Uterine incision-to-delivery interval and perinatal outcomes in transverse versus vertical incisions in preterm cesarean deliveries. J. Matern.-Fetal Neonatal Med. 2013, 26, 1788–1791. [Google Scholar] [CrossRef]
- Braun, T.; Weizsäcker, K.; Muallem, M.Z. Abnormally invasive placenta (AIP): Pre-cesarean amnion drainage to facilitate exteriorization of the gravid uterus through a transverse skin incision. J. Perinat. Med. 2018, 47, 12–15. [Google Scholar] [CrossRef]

{kind=link}
| Maternal Characteristics | Pfannenstiel Group (n: 49) | Midline Group (n: 18) | p-Value |
|---|---|---|---|
| Number of patients, n (%) | 49 (73.1%) | 18 (26.9%) | |
| Maternal age (years), Mean (±SD) | 33.4 (4.29) | 35.2 (4.38) | 0.642 |
| Gravida, Mean (±SD) | 3.69 (1.44) | 3.77 (1.21) | 0.574 |
| Parity, Mean (±SD) | 2.18 (1.23) | 2.11 (1.07) | 0.976 |
| Previous C/S, Mean (±SD) | 1.91 (0.67) | 2.05 (1.20) | 0.877 |
| Notable pre-existing condition ª, n (%) | 11 (22.4%) | 12 (66.7%) | 0.001 |
| BMI (kg/m²), Mean (±SD) | 31.0 (6.03) | 29.9 (4.06) | 0.694 |
| BMI ≥ 30 kg/m2, n (%) | 24 (49.0%) | 10 (55.6) | 0.633 |
| GA at diagnosis, Mean (±SD) | 29.1 (4.54) | 25.2 (4.22) | 0.890 |
Placenta localization, n (%)
| 41 (83.7%) 8 (16.3%) | 13 (72.2%) 5 (27.8%) | 0.312 |
At the last ultrasound examination
| 46 (93.9%) 3 (6.1%) | 17 (94.4%) 1 (5.6%) | 1.000 |
| 21 (42.9%) | 2 (11.1%) | 0.020 |
| GA of the first episode of antepartum hemorrhage (week), Median (min–max) | 30 (20–37) | 27 (26–28) | 0.225 |
| Hospitalized during pregnancy, n (%) | 39 (79.6%) | 17 (94.4%) | 0.264 |
| Number of days of hospitalization during pregnancy, Mean (±SD) | 8.5 (9.75) | 10 (7.7) | 0.165 |
Reasons for hospitalization, n (%)
| 38 (77.6%) 5 (10.2%) 0 (0%) 6 (12.2%) | 7 (38.9%) 1 (5.6%) 8 (44.4%) 2 (11.2%) | NA |
| Antenatal PPROM, n (%) | 4 (8.2%) | 0 (0%) | 0.211 |
| Preoperative (emergency) hemorrhage, n (%) | 14 (71.4%) | 0 (0%) | 0.014 |
| Emergency surgery, n (%) | 23 (46.9%) | 1 (5.6%) | 0.002 |
| Pfannenstiel Group (n: 49) | Midline Group (n: 18) | p-Value | |
|---|---|---|---|
| GA at delivery (week), Median (min–max) | 35 (24–40) | 34 (29–34) | 0.041 |
| Total time of surgery (minute), Mean (±SD) | 119.51 (42.89) | 168.66 (47.15) | 0.551 |
| Total hysterectomy, n (%) Subtotal hysterectomy, n (%) | 47 (95.9%) 2 (4.1%) | 16 (88.9%) 2 (11.1%) | 0.282 |
| Hypogastric artery ligation, n (%) | 30 (61.2%) | 0 (0%) | 0.000 |
| Salpingectomy, n (%) | 23 (46.9%) | 15 (83.3%) | 0.008 |
| Bladder injury, n (%) | 18 (36.7%) | 3 (16.7%) | 0.117 |
| Another tissue injury (ureter, bowel), n (%) | 0 (0%) | 0 (0%) | NA |
| Other surgeons present at surgery (urologist), n (%) | 5 (10.2%) | 3 (16.7%) | 0.672 |
| Number of patients with drainage tube, n (%) | 44 (89.8%) | 17 (94.4%) | 0.555 |
| Drainage tube days, Median (min–max) | 3 (0–8) | 2 (0–9) | 0.692 |
| Admission to ICU, n (%) | 17 (37.7) | 4 (22.2%) | 0.329 |
| Days in ICU, Median (min–max) | 1 (1–8) | 1 (1–1) | 0.635 |
| Number of patients using opiate, n (%) | 28 (57.1%) | 15 (83.3%) | 0.470 |
| Opiate dose (mg), Median (min–max) | 100 (50–100) | 100 (50–200) | 0.761 |
| Relap, n (%) | 5 (10.2%) | 0 (0%) | 0.159 |
| Relap time (after first surgery) (hours), Mean (±SD) | 10.2 (5.6) | - | NA |
| Length of hospital stay (days), Median (min–max) | 5 (3–18) | 5 (2–25) | 0.678 |
Postoperative complications, n (%)
| 48 (98%) 0 (0%) 1 (2%) | 16 (88.9%) 2 (11.1%) 0 (0%) | 0.052 |
Pathology report, n (%)
| 43 (87.8%) 3 (6.1%) 3 (6.1%) | 8 (44.4%) 0 (0%) 10 (55.6%) | 0.000 |
| Dissatisfaction with the incision, n (%) | 1 (2%) | 6 (33.3%) | 0.001 |
| Vaginal dryness after surgery, n (%) | 3 (6.1%) | 5 (27.8%) | 0.028 |
| Pfannenstiel Group (n: 49) | Midline Group (n: 18) | p-Value | |
|---|---|---|---|
| Number of patients receiving RBC, n (%) | 45 (91.8%) | 14 (77.8%) | 0.196 |
| Units of RBC, Median (min–max) | 4 (0–22) | 2.5 (0–7) | 0.056 |
| Patients at >4 units of packed RBCs transfused, n (%) | 26 (53.1%) | 6 (33.3%) | 0.152 |
| Number of patients receiving FFP, n (%) | 32 (65.3%) | 13 (72.2%) | 0.593 |
| Units of FFP, Median (min–max) | 2 (0–17) | 1 (0–7) | 0.426 |
| Crystalloid (mL), Median (min–max) | 3000 (1000–6000) | 3000 (2000–5000) | 0.364 |
| Colloid (mL), Median (min–max) | 500 (0–1000) | 500 (0–500) | 0.128 |
| Pfannenstiel Group (n: 49) Mean ± SD | Midline Group (n: 18) Mean ± SD | p-Value | |
|---|---|---|---|
Hb (g/dL)
| 11.03 ± 0.98 8.50 ± 1.36 2.53 ± 1.70 | 10.72 ± 1.25 8.84 ± 1.30 1.87 ± 1.60 | 0.593 0.483 0.689 |
Htc (%)
| 33.18 ± 3.27 25.26 ± 3.72 7.92 ± 4.78 | 32.31 ± 3.13 26.30 ± 3.79 6.00 ± 4.76 | 0.852 0.808 0.732 |
WBC (103/mL)
| 9530 ± 2814 12,940 ± 5828 −3410 ± 5740 | 9207 ± 2423 12,462 ± 3318 −3255 ± 4294 | 0.886 0.310 0.457 |
Platelet (103/mL)
| 219.61 ± 73.88 174.59 ± 73.56 45.02 ± 80.28 | 278.54 ± 59.88 134.54 ± 28.17 144.04 ± 71.33 | 0.429 0.738 0.001 |
| Pfannenstiel Group (n: 49) | Midline Group (n: 18) | p-Value | |
|---|---|---|---|
| Delivery time (minute), Mean (±SD) | 8.6 (0.8) | 7.7 (1.06) | 0.859 |
| Birth weight (grams), Mean (±SD) | 2538 (775) | 2587 (455) | 0.077 |
| APGAR 1 min, Median (min–max) APGAR 5 min, Median (min–max) | 8 (0–9)9 (0–10) | 7 (1–9)8.5 (6–10) | 0.417 |
| Admission to NICU, n (%) | 17 (34.7%) | 4 (22.2%) | 0.329 |
| Days in NICU (days), Median (min–max) | 1 (1–8) | 1 (1–1) | 0.635 |
Reason for admission to NICU
| 11 (22.4%) 4 (8.2%) 4 (8.2%) | 9 (50%) 1 (5.6%) 1 (5.6%) | 0.065 |
| Studies | Number of Patients, n (%) | Previous C/S | Antepartum Hemorrhage | Preoperative (Emergency) Hemorrhage, n (%) | Emergency Surgery (%) | GA at Delivery (Week) | Total Time of Surgery (Minute) | Hysterectomy | Bladder Injury, n (%) | Hypogastric Artery Ligation, n (%) | Relaparotomy, n (%) | Length of Hospital Stay (days) | Dissatisfaction with the Incision, n (%) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Soyer-Çalışkan et al. [14] | Transverse Group | 81 (69.8%) | 2 (1–4) b | 35.46 (1.98) a | 91.23 (16.53) a | 66 (81.5%) | 9 (11.1%) | 0 (0%) | 5 (3–8) b | |||||
| Vertical Group | 35 (30.2%) | 2 (1–6) b | 34.23 (2.82) a | 100.44 (18.35) a | 29 (82.9%) | 13 (37.1%) | 2 (5.7%) | 4 (3–8) b | ||||||
| p-Value | 0.014 | 0.024 | 0.010 | 0.860 c | 0.001 | 0.030 | 0.111 | |||||||
| Akbaba [15] | High Transverse Group | 24 (54.5%) | 2.1 (0.7) a | 34.4 (3.5) a | 101.5 (8.2) a | 24 (100%) | 5.5 (1.1) a | 3 (12.4%) | ||||||
| Vertical Group | 20 (45.5%) | 1.9 (0.7) a | 34.3 (3.7) a | 129.8 (7.7) a | 20 (100%) | 8.0 (1.1) a | 13 (65%) | |||||||
| p-Value | 0.23 | 0.96 | 0.04 | 0.03 | 0.01 | |||||||||
| Our Study | Pfannenstiel Group | 49 (73.1%) | 1.91 (0.67) a | 21 (42.9%) | 14 (71.4%) | 23 (46.9%) | 35 (24–40) b | 119.51 (42.89) a | 49 (100%) | 18 (36.7%) | 30 (61.2%) | 5 (10.2%) | 5 (3–18) b | 1 (2%) |
| Midline Group | 18 (26.9%) | 2.05 (1.20) a | 2 (11.1%) | 0 (0%) | 1 (5.6%) | 34 (29–34) b | 168.66 (47.15) a | 18 (100%) | 3 (16.7%) | 0 (0%) | 0 (0%) | 5 (2–25) b | 6 (33.3%) | |
| p-Value | 0.877 | 0.020 | 0.014 | 0.002 | 0.041 | 0.551 | 1.000 | 0.117 | 0.000 | 0.159 | 0.678 | 0.001 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kandemir, H.; Kirtis, E.; Bulbul, G.A.; Dogan, S.; Mendilcioglu, I.; Sanhal, C.Y.; Sakinci, M.; Dogan, N.U. Intraoperative and Postoperative Outcomes of Pfannenstiel and Midline Skin Incisions in Placenta Accreta Spectrum Disorders: Single-Center Experience. Medicina 2024, 60, 1102. https://doi.org/10.3390/medicina60071102
Kandemir H, Kirtis E, Bulbul GA, Dogan S, Mendilcioglu I, Sanhal CY, Sakinci M, Dogan NU. Intraoperative and Postoperative Outcomes of Pfannenstiel and Midline Skin Incisions in Placenta Accreta Spectrum Disorders: Single-Center Experience. Medicina. 2024; 60(7):1102. https://doi.org/10.3390/medicina60071102
Chicago/Turabian StyleKandemir, Hulya, Emine Kirtis, Gul Alkan Bulbul, Selen Dogan, Inanc Mendilcioglu, Cem Yasar Sanhal, Mehmet Sakinci, and Nasuh Utku Dogan. 2024. "Intraoperative and Postoperative Outcomes of Pfannenstiel and Midline Skin Incisions in Placenta Accreta Spectrum Disorders: Single-Center Experience" Medicina 60, no. 7: 1102. https://doi.org/10.3390/medicina60071102
APA StyleKandemir, H., Kirtis, E., Bulbul, G. A., Dogan, S., Mendilcioglu, I., Sanhal, C. Y., Sakinci, M., & Dogan, N. U. (2024). Intraoperative and Postoperative Outcomes of Pfannenstiel and Midline Skin Incisions in Placenta Accreta Spectrum Disorders: Single-Center Experience. Medicina, 60(7), 1102. https://doi.org/10.3390/medicina60071102