
The Application of Robotics in Cardiac Rehabilitation: A Systematic Review
 , , ,
, , ,
Abstract
:1. Introduction
2. Methodology
2.1. Objective
2.2. Design
2.3. Study Protocol
2.4. Search Strategy
2.5. Inclusion and Exclusion Criteria
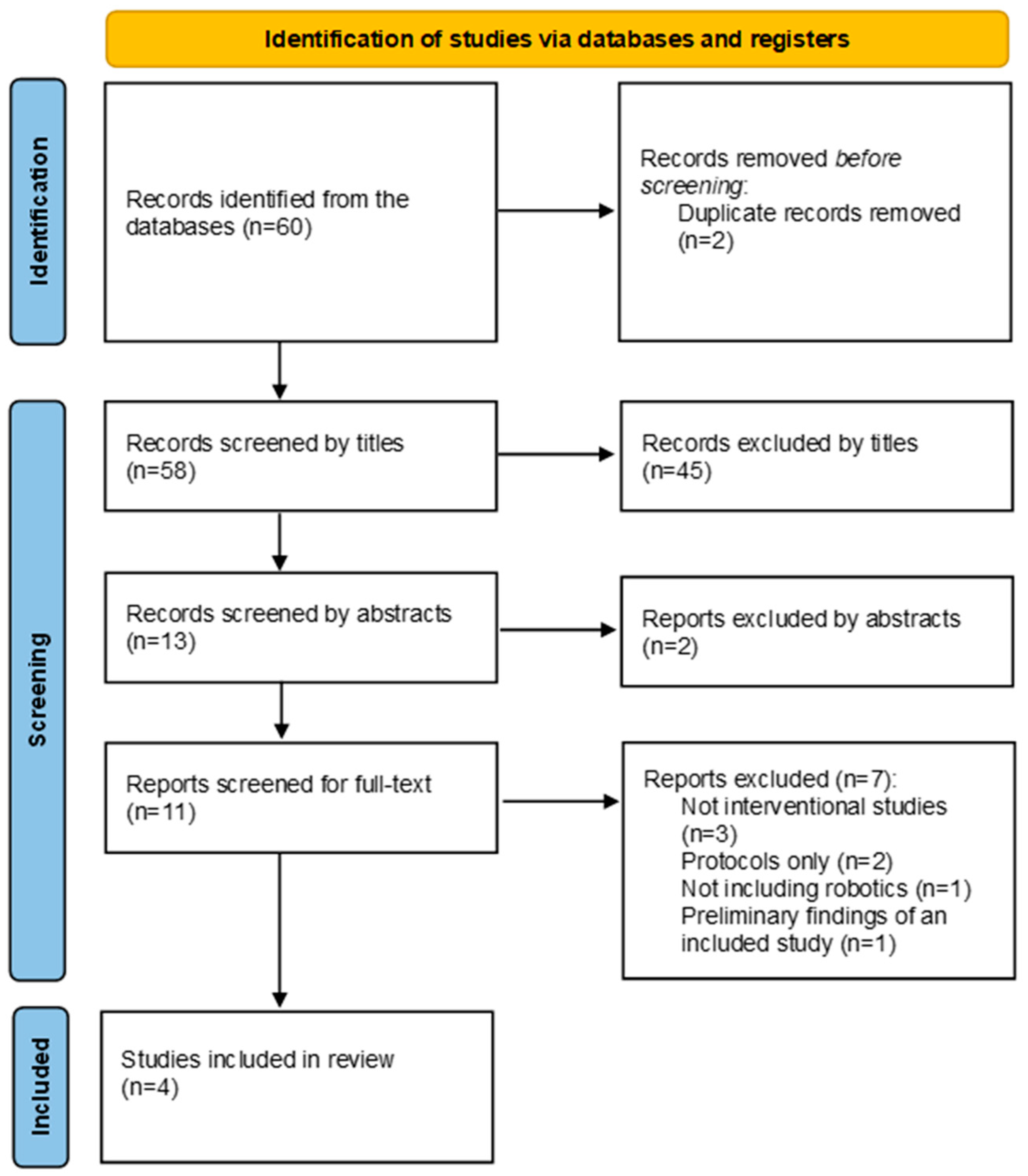
2.6. Study Selection
2.7. Data Extraction
2.8. The Quality Assessment and Risk of Bias of the Included Trials
3. Results
3.1. Study Characteristics
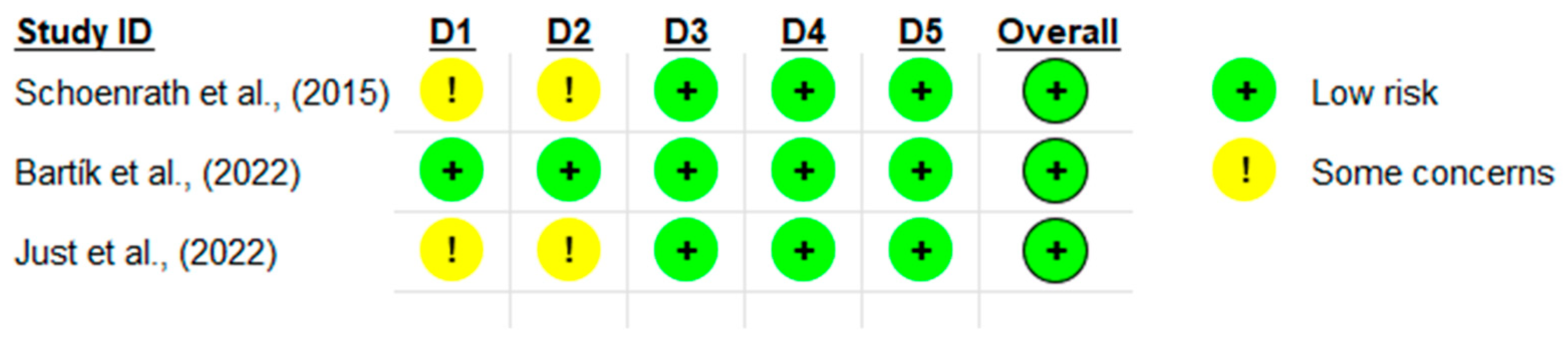
3.2. Quality Assessment
3.3. Robotics Used
3.4. Intervention Prescription: FITT
3.5. Effects of Robotics on Peak Oxygen Consumption (VO2 Peak) and Ejection Fraction (EF)
3.6. Effects of Robotic Interventions on Exercise Capacity
3.7. Effects of Robotic Interventions on Quality of Life (QOL) and Physical Functioning
3.8. Safety of Robotic Interventions (Adverse Events)
4. Discussion
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Cardiovascular Diseases (CVDs): Key Facts 2017. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 20 June 2024).
- Kim, H.-S.; Kwon, I.H.; Cha, W.C. Future and development direction of digital healthcare. Healthc. Inform. Res. 2021, 27, 95. [Google Scholar] [CrossRef] [PubMed]
- Meskó, B.; Drobni, Z.; Bényei, É.; Gergely, B.; Győrffy, Z. Digital health is a cultural transformation of traditional healthcare. Mhealth 2017, 3, 38. [Google Scholar] [CrossRef] [PubMed]
- Jat, A.S.; Grønli, T.-M. Smart watch for smart health monitoring: A literature review. In Proceedings of the International Work-Conference on Bioinformatics and Biomedical Engineering, Gran Canaria, Spain, 27–30 June 2022; pp. 256–268. [Google Scholar]
- Aburub, A.; Darabseh, M.Z.; Badran, R.; Eilayyan, O.; Shurrab, A.a.M.; Degens, H. The Effects of Digital Health Interventions for Pulmonary Rehabilitation in People with COPD: A Systematic Review of Randomized Controlled Trials. Medicina 2024, 60, 963. [Google Scholar] [CrossRef] [PubMed]
- Widmer, R.J.; Allison, T.G.; Lerman, L.O.; Lerman, A. Digital health intervention as an adjunct to cardiac rehabilitation reduces cardiovascular risk factors and rehospitalizations. J. Cardiovasc. Transl. Res. 2015, 8, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Frederix, I.; Vanhees, L.; Dendale, P.; Goetschalckx, K. A review of telerehabilitation for cardiac patients. J. Telemed. Telecare 2015, 21, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, M.; Kan, L. Digital technology and the future of health systems. Health Syst. Reform. 2019, 5, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Oldenburg, J.; Chase, D.; Christensen, K.T.; Tritle, B. Engage!: Transforming Healthcare through Digital Patient Engagement; CRC Press: Boca Raton, FL, USA, 2020. [Google Scholar]
- Bunting, J.; Withers, T.; Heneghan, N.; Greaves, C. Digital interventions for promoting exercise adherence in chronic musculoskeletal pain: A systematic review and meta-analysis. Physiotherapy 2021, 111, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Céspedes, N.; Irfan, B.; Senft, E.; Cifuentes, C.A.; Gutierrez, L.F.; Rincon-Roncancio, M.; Belpaeme, T.; Múnera, M. A socially assistive robot for long-term cardiac rehabilitation in the real world. Front. Neurorobotics 2021, 15, 633248. [Google Scholar] [CrossRef] [PubMed]
- Fazekas, G. Robotics in rehabilitation: Successes and expectations. Int. J. Rehabil. Res. 2013, 36, 95–96. [Google Scholar] [CrossRef]
- Guo, Y.; Gu, X.; Yang, G.-Z. Human–Robot Interaction for Rehabilitation Robotics; Springer: Berlin/Heidelberg, Germany, 2021. [Google Scholar]
- Erol, D.; Mallapragada, V.; Sarkar, N.; Uswatte, G.; Taub, E. Autonomously adapting robotic assistance for rehabilitation therapy. In Proceedings of the First IEEE/RAS-EMBS International Conference on Biomedical Robotics and Biomechatronics, Pisa, Italy, 20–22 February 2006; IEEE: Piscataway, NJ, USA, 2006; pp. 567–572. [Google Scholar]
- García-Bravo, S.; Cuesta-Gómez, A.; Campuzano-Ruiz, R.; López-Navas, M.J.; Domínguez-Paniagua, J.; Araújo-Narváez, A.; Barreñada-Copete, E.; García-Bravo, C.; Flórez-García, M.T.; Botas-Rodríguez, J. Virtual reality and video games in cardiac rehabilitation programs. A systematic review. Disabil. Rehabil. 2021, 43, 448–457. [Google Scholar] [CrossRef]
- Chang, W.H.; Kim, Y.-H. Robot-assisted therapy in stroke rehabilitation. J. Stroke 2013, 15, 174. [Google Scholar] [CrossRef] [PubMed]
- Mekki, M.; Delgado, A.D.; Fry, A.; Putrino, D.; Huang, V. Robotic rehabilitation and spinal cord injury: A narrative review. Neurotherapeutics 2018, 15, 604–617. [Google Scholar] [CrossRef] [PubMed]
- Payedimarri, A.B.; Ratti, M.; Rescinito, R.; Vanhaecht, K.; Panella, M. Effectiveness of platform-based robot-assisted rehabilitation for musculoskeletal or neurologic injuries: A systematic review. Bioengineering 2022, 9, 129. [Google Scholar] [CrossRef] [PubMed]
- EM MEDICA. Effects of robot-assisted gait training on postural instability in Parkinson’s disease: A systematic review. Eur. J. Phys. Rehabil. Med. 2021, 57, 472–477. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Macedo, L.G.; Elkins, M.R.; Maher, C.G.; Moseley, A.M.; Herbert, R.D.; Sherrington, C. There was evidence of convergent and construct validity of Physiotherapy Evidence Database quality scale for physiotherapy trials. J. Clin. Epidemiol. 2010, 63, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Yamato, T.P.; Maher, C.; Koes, B.; Moseley, A. The PEDro scale had acceptably high convergent validity, construct validity, and interrater reliability in evaluating methodological quality of pharmaceutical trials. J. Clin. Epidemiol. 2017, 86, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Auais, M.A.; Eilayyan, O.; Mayo, N.E. Extended exercise rehabilitation after hip fracture improves patients’ physical function: A systematic review and meta-analysis. Phys. Ther. 2012, 92, 1437–1451. [Google Scholar] [CrossRef]
- Hashimoto, K.; Hirashiki, A.; Ozaki, K.; Kawamura, K.; Sugioka, J.; Tanioku, S.; Sato, K.; Ueda, I.; Itoh, N.; Nomoto, K.; et al. Benefits of a Balance Exercise Assist Robot in the Cardiac Rehabilitation of Older Adults with Cardiovascular Disease: A Preliminary Study. J. Cardiovasc. Dev. Dis. 2022, 9, 191. [Google Scholar] [CrossRef]
- Schoenrath, F.; Markendorf, S.; Brauchlin, A.E.; Seifert, B.; Wilhelm, M.J.; Czerny, M.; Riener, R.; Falk, V.; Schmied, C.M. Robot-Assisted Training Early after Cardiac Surgery. J. Card. Surg. 2015, 30, 574–580. [Google Scholar] [CrossRef]
- Bartík, P.; Vostrý, M.; Hudáková, Z.; Šagát, P.; Lesňáková, A.; Dukát, A. The Effect of Early Applied Robot-Assisted Physiotherapy on Functional Independence Measure Score in Post-Myocardial Infarction Patients. Healthcare 2022, 10, 937. [Google Scholar] [CrossRef] [PubMed]
- Just, I.A.; Fries, D.; Loewe, S.; Falk, V.; Cesarovic, N.; Edelmann, F.; Feuerstein, A.; Haufe, F.L.; Xiloyannis, M.; Riener, R.; et al. Movement therapy in advanced heart failure assisted by a lightweight wearable robot: A feasibility pilot study. ESC Heart Fail. 2022, 9, 1643–1650. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Search Strategy | Search Strategy |
|---|---|
| P (population) | The keywords to be used are the following: S1 = “cardiovascular diseases” OR “CVD” OR “cardiac diseases” OR “coronary heart diseases” OR “cardiac surgeries” OR “heart diseases” OR “cardiac disorders’’ OR “heart disorders” OR “heart failure” OR “myocardial ischemia” OR “MI” |
| I (Intervention) | S2 = “robotics” OR “robot” OR “robots” OR “socially assistive robotics” OR “social robots” AND “physiotherapy” OR “physiotherapist” OR “rehabilitation” OR “cardiac rehabilitation” OR “cardiovascular rehabilitation” OR “cardiac rehab” OR “cardiovascular rehab” OR “cardiac physiotherapy” OR “cardiovascular physiotherapy” |
| C (comparison) | The comparison was not limited to any intervention and even included single-arm longitudinal studies where found. |
| O (outcome measures) | Outcome measures were not limited to any keywords |
| S (study design) | Randomized controlled trials, controlled clinical trials, or longitudinal interventional trials |
| Combined final search | S1 AND S2 |
| Author (Year) | Trial Location | Study Design | Sample Size | Age Years (Mean ± SD) | Technology Utilized | Physical Capacity | Exercise Prescription | Primary Outcome | Secondary Outcome | Key Findings |
|---|---|---|---|---|---|---|---|---|---|---|
| Schoenrath et al., (2015) [25] | Switzerland | RCT | Robot-assist Group: 10 participants Conventional Group: 20 participants | 60.3 ± 11.2 | Lokomat® system |
| Duration of treatment and follow up: 1 month. Both groups received standard respiratory training Robot-assist Group: F: 3×/week. I: RPE scale (6–20); target exertion 11–12 T: Two to three exercise sets of 6–10 quadricep resistance exercises for both lower extremities. T: 40 min/session Conventional Group F: 5×/week. T: Training trunk stability and walking T: 10–30 min/session. |
|
|
|
| Bartík et al., (2022) [26] | Czech Republic | RCT | Experimental group: 46 participants Control group: 46 participants F:M = 42:50 | 60.9 ± 2.32 | Motomed letto/Thera Trainer tigo |
| Duration of treatment and follow up: 14 days (28 sessions) Both groups received an early intensive physiotherapy program F: 7×/week (2×/day) I: depended on patient’s condition T: Active assistant ROM exercises in different positions (standing, sitting, lying in a supine position) T: 45 min/session. Intervention group (IG) T: active-assisted and active repetitive analytical movements of the upper and lower limbs exercise in different positions (on the bed, sitting, standing). Mobilization, short walk, short walk up and down the stairs, and robot-assisted training with repetitive movements T: 45 min/session Control group (CG) T: active-assisted and active repetitive analytical movements of upper and lower limb exercise on the bed, sitting, standing. Mobilization, short walk, short walk up and down the stairs T: 45 min/session |
|
| |
| Hashimoto et al., (2022) [24] | Japan | A single arm longitudinal study | 52 participants (one group) F:M = 24:28 Assessed at baseline and after 4 months | 76.9 ± 6.8 | The BEAR | VO2 peak | Duration of intervention and follow up: 4 months (16 session) F: 1×/week I: Depended on patient condition T: balance and aerobic exercise T: 21 min/session |
|
| |
| Just et al., (2022) [27] | Switzerland | Cross-over trial | Standard group (G1): 10 participants. REU (G2): 10 participants. F:M = 4:16 | 49.4 ± 11.0 | The Myosuit | Vital signs |
G1 T: Performed a single session of timed walking for 6 min, standing, sitting down and standing up from a chair, and climbing stairs. For standing, a static mode of the Myosuit G2 T: Single standardized REU with dynamic walking, resistance exercise of upper body, and dynamic and static balance training T: 60 min/session |
|
|
|
| Author (Year) | 1. Eligibility Criteria Were Specified | 2. Subjects Were Randomly Allocated to Groups | 3. Allocation Was Concealed | 4. The Groups Were Similar at Baseline Regarding Prognostic Indicators | 5. There Was Blinding of All Subjects | 6. There Was Blinding of All Therapists Who Administered the Therapy | 7. There Was Blinding of All Assessors Who Measured at Least One Key Outcome | 8. Measures of at Least One Key Outcome Were Obtained from More Than 85% of the Subjects | 9. All Subjects for Whom Outcome Measures Were Available Received the Treatment or Control Condition as Allocated | 10. The Results of between-Group Statistical Comparisons Are Reported for at Least One Key Outcome | 11. Point Measures and Measures of Variability for at Least One Key Outcome Were Reported | Total PEDro Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Schoenrath et al., (2015) [25] | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Bartík et al., (2022) [26] | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 8 |
| Just et al., (2022) [27] | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aburub, A.; Darabseh, M.Z.; Badran, R.; Shurrab, A.M.; Amro, A.; Degens, H. The Application of Robotics in Cardiac Rehabilitation: A Systematic Review. Medicina 2024, 60, 1161. https://doi.org/10.3390/medicina60071161
Aburub A, Darabseh MZ, Badran R, Shurrab AM, Amro A, Degens H. The Application of Robotics in Cardiac Rehabilitation: A Systematic Review. Medicina. 2024; 60(7):1161. https://doi.org/10.3390/medicina60071161
Chicago/Turabian StyleAburub, Aseel, Mohammad Z. Darabseh, Rahaf Badran, Ala’a M. Shurrab, Anwaar Amro, and Hans Degens. 2024. "The Application of Robotics in Cardiac Rehabilitation: A Systematic Review" Medicina 60, no. 7: 1161. https://doi.org/10.3390/medicina60071161