
Intravital Position Study of the Clinical Anatomy of the Middle Lobe and Superior Poles of the Thyroid Gland

 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
5.1. Implications
- Neck flexion reduces the distance from the center of the jugular notch of the sternum to the superior poles and lateral points of the outer edge of the middle parts of the thyroid lobes in all study groups by 78.4 mm to the maximum in endomorphic men and 44.1 mm to the minimum in ectomorphic men.
- Neck extension increases the distance from the center of the jugular notch to the superior pole and lateral points of the outer edge of the middle parts of the thyroid lobes by 100.1 mm maximum in endomorphic males and 73.8 mm minimum in ectomorphic males.
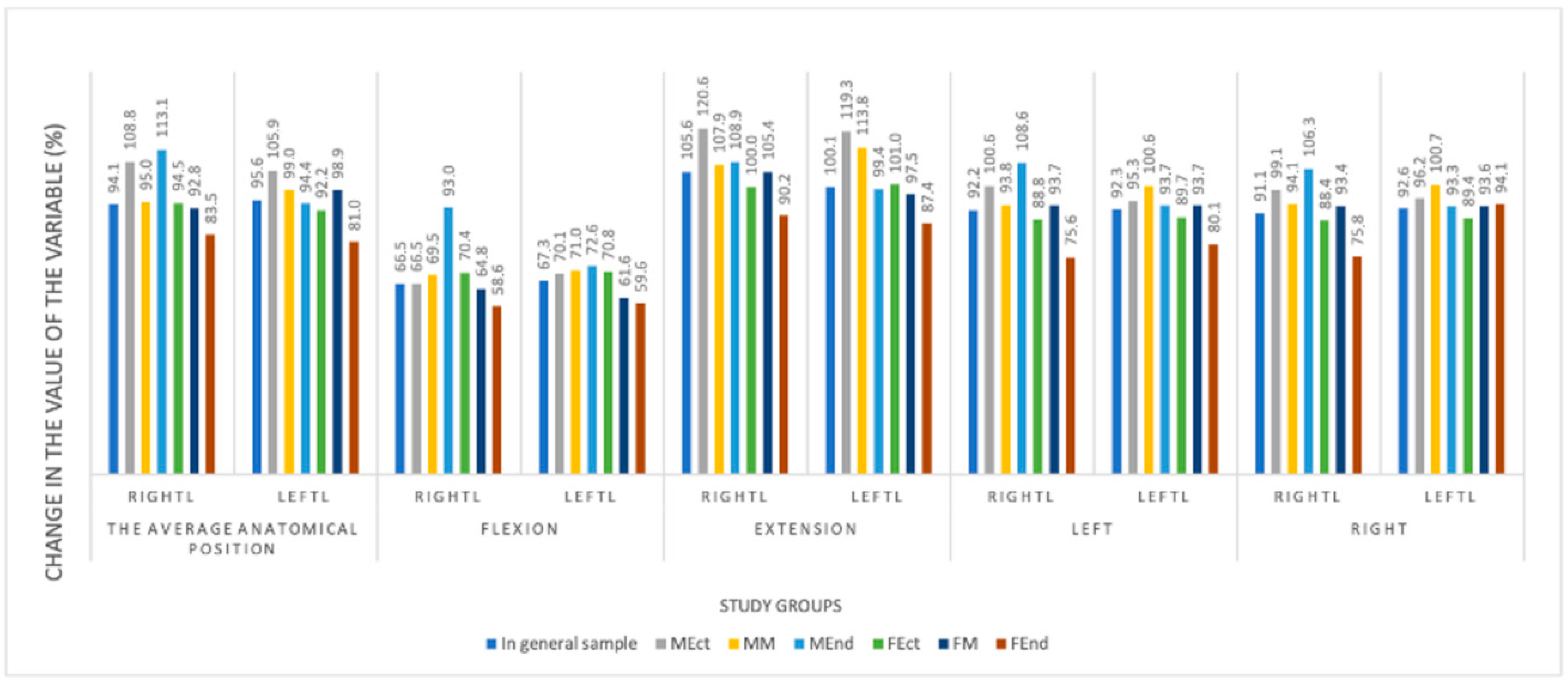
- The distance from the reference point of the sternum notch to the lateral points of the outer edge of the middle parts of the thyroid lobes decreases as much as possible when bending the neck in ectomorph males (by 42.1% on the left and 42.8% on the right). This distance is maximized when the neck is extended in male endomorphs on the right by 22% and on the left by 27.1%.
- The maximum distance from the reference point of the sternum notch to the superior pole of the thyroid gland decreases with neck flexion in ectomorph males by 38.9% on the right and mesomorph females by 37.8% on the left. Most of all, this distance increases in male ectomorphs on the right and left by 13.3%.
- Head rotations lead to a decrease in the distance from the center of the jugular notch of the sternum to the superior pole of the right and left thyroid lobes. When the head was rotated to the right, the maximum changes were observed in male ectomorphs—a decrease of 8.3% on the right and 8.6% on the left. When rotating the head to the left, the maximum changes were also recorded in the group of male-ectomorphs—a decrease of 9.5% on the left and 7.3% on the right.
5.2. Limitations
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Trunin, E.M.; Dydykin, S.S.; Tatarkin, V.V.; Vasiliev, Y.L.; Movchan, K.N.; Bakunov, A.M.; Mustafina, E.A.; Resnyanskaya, E.D. Surgical cervicology as an independent section of surgery-utopia or the near future. Oper. Surg. Clin. Anat. (Pirogov Sci. J.) 2023, 2, 55–64. [Google Scholar]
- Chaplygina, E.V.; Kuchieva, M.B.; Kalashaov, B.M. Anatomical variability of the cervical spine in age, gender and type aspects. Opportunities and prospects for studying. Mod. Probl. Sci. Educ. 2021, 3, 170–177. [Google Scholar] [CrossRef]
- Kalashov, B.M.; Chaplygina, E.V.; Kaplunova, O.A.; Kuchieva, M.B. Anatomical variability of the cervical spine according to MRI data in normal and some pathological conditions. Volgogr. Sci. Med. J. 2022, 1, 17–21. [Google Scholar]
- Babich, A.I.; Kazantseva, E.V. Topographic and anatomical features of the neck and thyroid gland. Bull. Med. Inst. “Reaviz”: Rehabil. Dr. Health 2022, 2, 56. [Google Scholar]
- Scott, B.; Wong, R.J. Step-by-Step Thyroidectomy-Incision, Nerve Identification, Parathyroid Preservation, and Gland Removal. Otolaryngol. Clin. N. Am. 2024, 57, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Trunin, E.M.; Tatarkin, V.V.; Smirnov, A.A.; Klitsenko, O.A.; Rybakov, V.A. Miniaccess in the surgical treatment of papillary thyroid cancer. Int. Sci. Res. J. 2016, 46, 131–137. [Google Scholar] [CrossRef]
- Trunin, E.M.; Tatarkin, V.V.; Chernyshev, M.D.; Brovin, D.A.; Movchan, K.N.; Vasiliev, Y.L.; Otochkin, V.V.; Bakunov, A.M.; Resnyanskaya, E.; Babaytseva, A.E.; et al. Method for Performing Surgical Operations on the Skin of the Patient. The Thyroid. The Thyroid Gland Patent number RU2798713, 23 June 2023. [Google Scholar]
- Serpell, J.W.; Grodski, S.F.; O’Donell, C. Does neck extension elevate the thyroid gland cephalad to potentially improve access during thyroidectomy? ANZ J. Surg. 2003, 73, 887–889. [Google Scholar] [CrossRef]
- Busarin, D.N.; Kazantseva, E.V.; Starchik, D.A. Constitutional features of men and women when using different somatotyping schemes. Quest. Morphol. XXI Century 2021, 7, 68–76. [Google Scholar]
- Trunin, E.M.; Tatarkin, V.V.; Chernyshev, M.D.; Brovin, D.A.; Shulga, V.P.; Bakunov, A.M.; Mustafina, E.A.; Shakhabadinov, V.Y.; Eremina, A.A.; Podezhikh, S.; et al. Device for Fixing the Patient’s Head When Performing Magnetic Resonance Imaging of the Neck. Patent number RU217872, 21 April 2023. [Google Scholar]
- Trunin, E.M.; Tatarkin, V.V.; Shchegolev, A.I.; Timokhov, G.V.; Petrov, S.V.; Stetsik, E.O.; Nechkin, D.K.; Chernyshev, M.D.; Vasiliev, Y.L.; Bakunov, A.M.; et al. Decision-Making Assistant in Choosing the Optimal Personalized Minimally Invasive Access to the Thyroid Gland. Patent number RU2024663047, 3 June 2024. [Google Scholar]
- Chaplygina, E.V.; Kaplunova, O.A.; Kuchieva, M.B.; Kalashaov, B.M. Angular parameters of cervical lordosis in people with different neck shapes. Morfol. Vedom.–Morphol. Newsl. 2023, 31, 702. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Snoey, E.R.; Clements, R.C.; Hern, H.G.; Price, D. Effect of head rotation on vascular anatomy of the neck: An ultrasound study. J. Emerg. Med. 2006, 31, 283–286. [Google Scholar] [CrossRef] [PubMed]
- Hwang, K.; Huan, F.; Ki, S.H.; Nam, Y.S.; Han, S.H. Location of the mandibular branch of the facial nerve according to the neck position. J. Craniofacial Surg. 2012, 23, 1488–1490. [Google Scholar] [CrossRef] [PubMed]
- Takenaka, I.; Aoyama, K.; Iwagaki, T. Combining head-neck position and head-down tilt to prevent pulmonary aspiration of gastric contents during induction of anaesthesia: A volunteer and manikin study. Eur. J. Anaesthesiol. 2012, 29, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Tong, B.; Fang, R.; Smith, B.L. Study of the head and neck position in microlaryngoscopy using magnetic resonance imaging. Eur. Arch. Otorhinolaryngol. 2013, 270, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.D.; Kumar, G.; Kanona, H.; Jovaisa, T.; Kaddour, H. Endotracheal tube positioning during neck extension in thyroidectomy. J. Laryngol. Otol. 2015, 129, 996–999. [Google Scholar] [CrossRef] [PubMed]
- Mavrocordatos, P.; Bissonnette, B.; Ravussin, P. Effects of neck position and head elevation on intracranial pressure in anaesthetized neurosurgical patients: Preliminary results. J. Neurosurg. Anesthesiol. 2000, 12, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Popescu, M.; Terzea, D.C.; Carsote, M.; Ghenea, A.E.; Costache, A.; Popescu, I.A.S.; Biciuşcă, V.; Busuioc, C.J.; Ghemigian, A.M. COVID-19 infection: From stress-related cortisol levels to adrenal glands infarction. Rom. J. Morphol. Embryol. 2022, 63, 39–48. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scan Plane | Parameters | ||||
|---|---|---|---|---|---|
| FOV * | Slice Thickness | Spacing | Slices | TR * | |
| 3 Pl Loc * | 25 | 5 | 5 | 15 | - |
| Sag T2 * | 25 | 4 | 1 | 23 | 3835 |
| Cor T2 * | 25 | 4 | 1.5 | 14 | 2200 |
| Ax T2 * | 25 | 4 | 1.5 | 20 | 2650 |
| Title 1 | Gender | Ectomorph | Mesomorph | Endomorph | In the General Sample |
|---|---|---|---|---|---|
| Average anatomical position Me (LQ; HQ) * | male | 77.3 (74.2; 80.4) | 75.2 (72.4; 78.0) | 82.4 (79.3; 85.5) | 73.0 (66.7; 78.0) |
| female | 67.5 (65.1; 69.9) | 71.9 (69.0; 74.8) | 61.1 (58.2; 64.0) | ||
| Flexion Me (LQ; HQ) | male | 44.1 (41.0; 47.2) | 53.9 (51.1; 56.8) | 78.4 (75.3; 81.5) | 51.2 (45.1; 55.7) |
| female | 52.4 (50.0; 54.8) | 51.3 (48.4; 54.2) | 44.4 (41.5; 47.3) | ||
| Extension Me (LQ; HQ) | male | 73.8 (70.7; 76.9) | 87.0 (84.1; 89.8) | 100.1 (97.0; 103.2) | 82.0 (74.0; 86.8) |
| female | 75.7 (73.3; 78.2) | 82.1 (79.2; 85.0) | 74.2 (71.3; 77.1) | ||
| Left rotation Me (LQ; HQ) | male | 71.6 (68.5; 74.7) | 75.2 (72.3; 78.0) | 69.7 (66.6; 72.8) | 68.0 (64.0; 72.5) |
| female | 64.8 (62.3; 67.2) | 71.9 (69.0; 74.8) | 53.9 (51.0; 56.8) | ||
| Right rotation Me (LQ; HQ) | male | 70.8 (67.7; 73.9) | 76.2 (73.4; 79.0) | 70.1 (67.0; 73.2) | 68.4 (63.8; 72.7) |
| female | 65.1 (62.7; 67.5) | 71.4 (68.5; 74.3) | 53.4 (50.5; 56.3) |
| Title 1 | Gender | Ectomorph | Mesomorph | Endomorph | In the General Sample |
|---|---|---|---|---|---|
| Average anatomical position Me (LQ; HQ) * | male | 76.7 (73.2; 80.2) | 73.2 (70.0; 76.4) | 70.0 (66.5; 73.6) | 69.0 (65.1; 73.1) |
| female | 67.4 (64.7; 70.2) | 69.4 (66.1; 72.6) | 55.8 (52.5; 59.1) | ||
| Flexion Me (LQ; HQ) | male | 44.8 (41.3; 48.3) | 54.7 (51.6; 57.9) | 70.3 (66.7; 73.8) | 46.7 (44.0; 59.0) |
| female | 52.2 (49.5; 55.0) | 48.0 (44.7; 51.2) | 42.5 (39.2; 45.8) | ||
| Extension Me (LQ; HQ) | male | 71.6 (68.1; 75.1) | 82.5 (79.3; 85.7) | 89.9 (86.4; 93.4) | 77.1 (71.6; 85.6) |
| female | 74.8 (72.1; 77.6) | 79.5 (76.2; 82.8) | 69.6 (66.4; 72.9) | ||
| Left rotation Me (LQ; HQ) | male | 63.0 (59.5; 66.5) | 77.1 (73.9; 80.3) | 79.6 (76.1; 83.1) | 64.9 (58.9; 78.8) |
| female | 65.6 (62.9; 68.4) | 68.0 (64.7; 71.2) | 50.9 (47.7; 54.2) | ||
| Right rotation Me (LQ; HQ) | male | 62.7 (59.2; 66.2) | 76.0 (72.8; 79.2) | 79.6 (76.1; 83.1) | 65.0 (58.9; 77.3) |
| female | 65.4 (62.7; 68.2) | 68.0 (64.7; 71.3) | 51.9 (48.6; 55.2) |
| Title 1 | Gender | Ectomorph | Mesomorph | Endomorph | In the General Sample |
|---|---|---|---|---|---|
| Average anatomical position Me (LQ; HQ) * | Male | 108.8 (104.5; 113.1) | 95.0 (91.1; 98.9) | 113.1 (108.8; 117.3) | 94.1 (88.6; 109.8) |
| Female | 94.5 (91.2; 97.9) | 92.8 (88.8; 96.8) | 83.5 (79.5; 87.5) | ||
| Flexion Me (LQ; HQ) | Male | 66.5 (62.2; 70.8) | 69.5 (65.6; 73.4) | 93.4 (89.1; 97.7) | 66.5 (61.9; 71.1) |
| Female | 70.4 (67.1; 73.8) | 64.8 (60.8; 68.8) | 58.6 (54.6; 62.6) | ||
| Extension Me (LQ; HQ) | Male | 120.6 (116.3; 124.9) | 107.9 (104.0; 111.8) | 108.9 (104.7; 113.2) | 105.6 (96.2; 113.6) |
| Female | 100.0 (96.6; 103.3) | 105.4 (101.3; 109.4) | 90.2 (86.2; 94.2) | ||
| Left rotation Me (LQ; HQ) | Male | 100.6 (96.3; 104.9) | 93.8 (89.9; 97.7) | 108.6 (104.3; 112.9) | 92.2 (85.6; 103.4) |
| Female | 88.8 (85.4; 92.1) | 93.7 (89.7; 97.7) | 75.6 (71.6; 79.6) | ||
| Right rotation Me (LQ; HQ) | Male | 99.1 (94.8; 103.4) | 94.1 (90.2; 98.0) | 106.3 (102.0; 110.6) | 91.1 (85.7; 102.1) |
| Female | 88.4 (85.1; 91.7) | 93.4 (89.4; 97.4) | 75.8 (71.8; 79.8) |
| Title 1 | Gender | Ectomorph | Mesomorph | Endomorph | In the General Sample |
|---|---|---|---|---|---|
| Average anatomical position Me (LQ; HQ) * | Male | 105.9 (102.3; 109.6) | 99.0 (95.7; 102.3) | 94.4 (90.8; 98.0) | 95.6 (86.7; 103.1) |
| Female | 92.2 (89.3; 95.0) | 98.9 (95.6; 102.3) | 81.0 (77.7; 84.4) | ||
| Flexion Me (LQ; HQ) | Male | 70.1 (66.5; 73.8) | 71.0 (67.7; 74.3) | 72.6 (69.0; 76.2) | 67.3 (62.0; 72.1) |
| Female | 70.8 (68.0; 73.6) | 61.6 (58.2; 65.0) | 59.6 (56.2; 62.9) | ||
| Extension Me (LQ; HQ) | Male | 119.3 (115.7; 123.0) | 113.8 (110.5; 117.1) | 99.4 (95.8; 103.1) | 100.1 (95.0; 111.7) |
| Female | 101.0 (98.1; 103.8) | 97.5 (94.2; 100.9) | 87.4 (84.0; 90.8) | ||
| Left rotation Me (LQ; HQ) | Male | 95.3 (91.7; 98.9) | 100.6 (97.3; 103.9) | 93.7 (90.1; 97.3) | 92.3 (86.9; 97.9) |
| Female | 89.7 (86.9; 92.6) | 93.7 (90.3; 97.1) | 80.1 (76.7; 83.4) | ||
| Right rotation Me (LQ; HQ) | Male | 96.2 (92.6; 99.8) | 100.7 (97.4; 103.9) | 93.3 (89.7; 97.0) | 92.6 (87.4; 98.4) |
| Female | 89.4 (86.5; 92.2) | 93.6 (90.2; 97.0) | 79.4 (76.0; 82.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tatarkin, V.V.; Shchegolev, A.I.; Bakunov, A.M.; Vasil’ev, Y.L.; Chernyshev, M.D.; Serebryakov, E.A.; Kaplieva, K.L.; Stetsik, E.O.; Pulotova, T.; Velichko, E.V.; et al. Intravital Position Study of the Clinical Anatomy of the Middle Lobe and Superior Poles of the Thyroid Gland. Medicina 2024, 60, 1520. https://doi.org/10.3390/medicina60091520
Tatarkin VV, Shchegolev AI, Bakunov AM, Vasil’ev YL, Chernyshev MD, Serebryakov EA, Kaplieva KL, Stetsik EO, Pulotova T, Velichko EV, et al. Intravital Position Study of the Clinical Anatomy of the Middle Lobe and Superior Poles of the Thyroid Gland. Medicina. 2024; 60(9):1520. https://doi.org/10.3390/medicina60091520
Chicago/Turabian StyleTatarkin, Vladislav V., Andrey I. Shchegolev, Aleksandr M. Bakunov, Yuriy L. Vasil’ev, Mikhail D. Chernyshev, Evgeniy A. Serebryakov, Ksenia L. Kaplieva, Egor O. Stetsik, Tahmina Pulotova, Ellina V. Velichko, and et al. 2024. "Intravital Position Study of the Clinical Anatomy of the Middle Lobe and Superior Poles of the Thyroid Gland" Medicina 60, no. 9: 1520. https://doi.org/10.3390/medicina60091520
APA StyleTatarkin, V. V., Shchegolev, A. I., Bakunov, A. M., Vasil’ev, Y. L., Chernyshev, M. D., Serebryakov, E. A., Kaplieva, K. L., Stetsik, E. O., Pulotova, T., Velichko, E. V., & Trunin, E. M. (2024). Intravital Position Study of the Clinical Anatomy of the Middle Lobe and Superior Poles of the Thyroid Gland. Medicina, 60(9), 1520. https://doi.org/10.3390/medicina60091520