
Use of Artificial Intelligence on Imaging and Preoperatory Planning of the Knee Joint: A Scoping Review

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
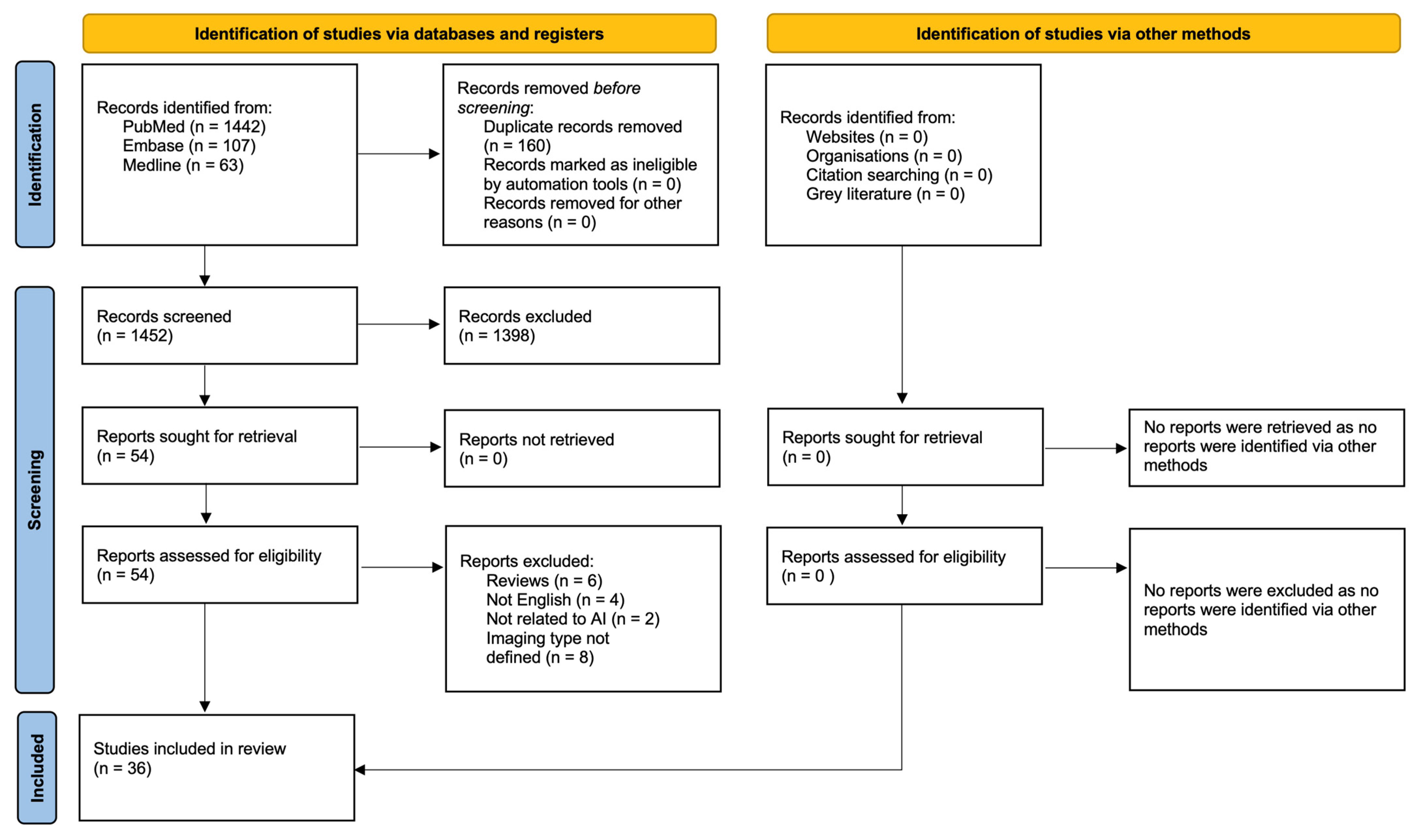
3.1. Screening and Selection
3.2. Overview of Papers
3.3. Imaging Methods
3.4. Range of AI Tool Applications
3.4.1. OA Diagnosis
3.4.2. Fracture Detection
3.4.3. Limb Alignment
3.4.4. Implant Size
3.5. AI Models and Technologies
4. Discussion
4.1. Strengths and Limitations
4.2. Next Steps
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Myers, T.G.; Ramkumar, P.N.; Ricciardi, B.F.; Urish, K.L.; Kipper, J.; Ketonis, C. Artificial Intelligence and Orthopaedics: An Introduction for Clinicians. J. Bone Jt. Surg. 2020, 102, 830–840. [Google Scholar] [CrossRef] [PubMed]
- Poduval, M.; Ghose, A.; Manchanda, S.; Bagaria, V.; Sinha, A. Artificial Intelligence and Machine Learning: A New Disruptive Force in Orthopaedics. Indian J. Orthop. 2020, 54, 109–122. [Google Scholar] [CrossRef] [PubMed]
- Castiglioni, I.; Rundo, L.; Codari, M.; Di Leo, G.; Salvatore, C.; Interlenghi, M.; Gallivanone, F.; Cozzi, A.; D’Amico, N.C.; Sardanelli, F. AI applications to medical images: From machine learning to deep learning. Phys. Medica 2021, 83, 9–24. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Chen, J.; Tang, Y.; Wang, C.; Landman, B.A. Transforming Medical Imaging with Transformers? A Comparative Review of Key Properties, Current Progresses, and Future Perspectives. Med. Image Anal. 2023, 85, 102762. [Google Scholar] [CrossRef]
- Federer, S.J.; Jones, G.G. Artificial intelligence in orthopaedics: A scoping review. PLoS ONE 2021, 16, e0260471. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Chaudhari, A.S.; Grissom, M.J.; Fang, Z.; Sveinsson, B.; Lee, J.H.; Gold, G.E.; Hargreaves, B.A.; Stevens, K.J. Diagnostic Accuracy of Quantitative Multicontrast 5-Minute Knee MRI Using Prospective Artificial Intelligence Image Quality Enhancement. Am. J. Roentgenol. 2021, 216, 1614–1625. [Google Scholar] [CrossRef]
- Lind, A.; Akbarian, E.; Olsson, S.; Nåsell, H.; Sköldenberg, O.; Razavian, A.S.; Gordon, M. Artificial intelligence for the classification of fractures around the knee in adults according to the 2018 AO/OTA classification system. PLoS ONE 2021, 16, e0248809. [Google Scholar] [CrossRef]
- Guermazi, A.; Tannaoury, C.; Kompel, A.; Murakami, A.M.; Ducarouge, A.; Gillibert, A.; Li, X.; Tournier, A.; Lahoud, Y.; Jarraya, M.; et al. Improving Radiographic Fracture Recognition Performance and Efficiency Using Artificial Intelligence. Radiology 2022, 302, 627–636. [Google Scholar] [CrossRef]
- Liu, P.R.; Zhang, J.-Y.; Xue, M.D.; Duan, Y.Y.; Hu, J.L.; Liu, S.X.; Xie, Y.; Wang, H.L.; Wang, J.W.; Huo, T.T.; et al. Artificial Intelligence to Diagnose Tibial Plateau Fractures: An Intelligent Assistant for Orthopedic Physicians. Curr. Med. Sci. 2021, 41, 1158–1164. [Google Scholar] [CrossRef]
- Schwarz, G.M.; Simon, S.; Mitterer, J.A.; Frank, B.J.H.; Aichmair, A.; Dominkus, M.; Hofstaetter, J.G. Artificial intelligence enables reliable and standardized measurements of implant alignment in long leg radiographs with total knee arthroplasties. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 2538–2547. [Google Scholar] [CrossRef] [PubMed]
- Smolle, M.A.; Goetz, C.; Maurer, D.; Vielgut, I.; Novak, M.; Zier, G.; Leithner, A.; Nehrer, S.; Paixao, T.; Ljuhar, R.; et al. Artificial intelligence-based computer-aided system for knee osteoarthritis assessment increases experienced orthopaedic surgeons’ agreement rate and accuracy. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 1053–1062. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.Z.; Abdelhameed, M.A.; AlMaeen, B.N.; Bernard de Villeneuve, F.; Fernandes, L.R.; Jacquet, C.; Ollivier, M. In slope-changing osteotomy one millimeter is not one degree: Results of an artificial intelligence-automated software analysis. Int. Orthop. 2023, 47, 915–920. [Google Scholar] [CrossRef]
- Bonnin, M.; Müller-Fouarge, F.; Estienne, T.; Bekadar, S.; Pouchy, C.; Ait Si Selmi, T. Artificial Intelligence Radiographic Analysis Tool for Total Knee Arthroplasty. J. Arthroplast. 2023, 38, S199–S207.e2. [Google Scholar] [CrossRef]
- Kim, M.S.; Cho, R.K.; Yang, S.C.; Hur, J.H.; In, Y. Machine Learning for Detecting Total Knee Arthroplasty Implant Loosening on Plain Radiographs. Bioengineering 2023, 10, 632. [Google Scholar] [CrossRef]
- Pagano, S.; Muller, K.; Gotz, J.; Reinhard, J.; Schindler, M.; Grifka, J.; Maderbacher, G. The Role and Efficiency of an AI-Powered Software in the Evaluation of Lower Limb Radiographs Before and After Total Knee Arthroplasty. Clin. Med. 2023, 12, 5498. [Google Scholar] [CrossRef]
- Liu, Z.; Zhou, A.; Fauveau, V.; Lee, J.; Marcadis, P.; Fayad, Z.A.; Chan, J.J.; Gladstone, J.; Mei, X.; Huang, M. Learning for Automated Measurement of Patellofemoral Anatomic Landmarks. Bioengineering 2023, 10, 815. [Google Scholar] [CrossRef]
- Wang, D.; Liu, S.G.; Ding, G.A.; Sun, A.L.; Jiang, D.; Jiang, J.; Zhao, J.Z.; Chen, D.S.; Ji, G.; Li, N.; et al. A Deep Learning Model Enhances Clinicians’Diagnostic Accuracy to More Than 96% for Anterior Cruciate Ligament Ruptures on Magnetic Resonance Imaging. Arthroscopy 2024, 40, 1197–1205. [Google Scholar] [CrossRef]
- Brejnebol, M.; Lenskjold, A.; Ziegeler, K.; Ruitenbeek, H.; Müller, F.C.; Nybing, J.U.; Visser, J.J.; Schiphouwer, L.M.; Jasper, J.; Bashian, B.; et al. Interobserver Agreement and Performance of Concurrent AI Assistance for Radiographic Evaluation of Knee Osteoarthritis. Radiology 2024, 312, e233341. [Google Scholar] [CrossRef]
- Alberti, L.; LoIacono, D.; Favaro, A.; Bondi, A.; Bertolino, L.; Bonanzinga, T. Artificial intelligence applied to q-angle measurement: Preliminary results on an algorithmbased on bounding box. Joints 2025, 3, e1397. [Google Scholar]
- Karnuta, J.M.; Luu, B.C.; Roth, A.L.; Haeberle, H.S.; Chen, A.F.; Iorio, R.; Schaffer, J.L.; Mont, M.A.; Patterson, B.M.; Krebs, V.E.; et al. Artificial Intelligence to Identify Arthroplasty Implants from Radiographs of the Knee. J. Arthroplast. 2021, 36, 935–940. [Google Scholar] [CrossRef]
- Schock, J.; Truhn, D.; Abrar, D.B.; Merhof, D.; Conrad, S.; Post, M.; Mittelstrass, F.; Kuhl, C.; Nebelung, S. Automated Analysis of Alignment in Long-Leg Radiographs by Using a Fully Automated Support System Based on Artificial Intelligence. Radiol. Artif. Intell. 2021, 3, e200198. [Google Scholar] [CrossRef] [PubMed]
- Tack, A.; Preim, B.; Zachov, S. Fully automated Assessment of Knee Alignment from Full-Leg X-Rays employing a “YOLOv4 and Resnet Landmark regression Algorithm” (YARLA): Data from the Osteoarthritis Initiative. Comput. Methods Programs Biomed 2021, 205, 106080. [Google Scholar] [CrossRef] [PubMed]
- Simon, S.; Schwartz, G.; Aichmair, A.; Frank, B.J.H.; Hummer, A.; DiFranco, M.D.; Dominkus, M.; Hofstaetter, J.G. Fully automated deep learning for knee alignment assessment in lower extremity radiographs: A cross-sectional diagnostic study. Skelet. Radiol. 2022, 51, 1249–1259. [Google Scholar] [CrossRef] [PubMed]
- Larson, N.; Nguyen, C.; Do, B.; Kaul, A.; Larson, A.; Wang, S.; Wang, E.; Bultman, E.; Stevens, K.; Pai, J.; et al. Artificial Intelligence System for Automatic Quantitative Analysis and Radiology Reporting of Leg Length Radiographs. J. Digit. Imaging 2022, 35, 1494–1505. [Google Scholar] [CrossRef]
- Lambrechts, A.; Wirix-Speetjens, R.; Maes, F.; Van Huffel, S. Artificial Intelligence Based Patient-Specific Preoperative Planning Algorithm for Total Knee Arthroplasty. Front. Robot. AI 2022, 9, 840282. [Google Scholar] [CrossRef]
- Houserman, D.J.; Berend, K.R.; Lombardi, A.V., Jr.; Fischetti, C.E.; Duhaime, E.P.; Jain, A.; Crawford, D.A. The Viability of an Artificial Intelligence/Machine Learning Prediction Model to Determine Candidates for Knee Arthroplasty. J. Arthroplast. 2022, 38, 2075–2080. [Google Scholar] [CrossRef]
- Erne, F.; Grover, P.; Dreischarf, M.; Reumann, M.K.; Saul, D.; Histing, T.; Nüssler, A.K.; Springer, F.; Scholl, C. Automated Artificial Intelligence-Based Assessment of Lower Limb Alignment Validated on Weight-Bearing Pre- and Postoperative Full-Leg Radiographs. Diagnostics 2022, 12, 2679. [Google Scholar] [CrossRef]
- Bernard de Villeneuve, F.; Jacquet, C.; El Kadim, B.; Donnez, M.; Coue, O.; Poujade, T.; Khakha, R.; Argenson, J.N.; Ollivier, M. An artificial intelligence based on a convolutional neural network allows a precise analysis of the alignment of the lower limb. Int. Orthop. 2023, 47, 511–518. [Google Scholar] [CrossRef]
- Fernandes, L.R.; Arce, C.; Martinho, G.; Campos, J.P.; Meneghini, R.M. Accuracy, Reliability, and Repeatability of a Novel Artificial Intelligence Algorithm Converting Two-Dimensional Radiographs to Three-Dimensional Bone Models for Total Knee Arthroplasty. J. Arthroplast. 2022, 38, 2032–2036. [Google Scholar] [CrossRef]
- Steele, J.R.; Jang, S.J.; Brilliant, Z.R.; Mayman, D.J.; Sculco, P.K.; Jerabek, S.A.; Vigdorchik, J.M. Deep Learning Phenotype Automation and Cohort Analyses of 1946 Knees Using the Coronal Plane Alignment of the Knee Classification. J. Arthroplast. 2023, 38, S215–S221.e1. [Google Scholar] [CrossRef] [PubMed]
- Huber, S.; Mitterer, J.A.; Vallant, S.M.; Simon, S.; Hanak-Hammerl, F.; Schwarz, G.M.; Klasan, A.; Hofstaetter, J.G. Gender-specific distribution of knee morphology according to CPAK and functional phenotype classification: Analysis of 8739 osteoarthritic knees prior to total knee arthroplasty using artificial intelligence. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 4220–4230. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Liu, X.; Chen, X.; Xu, H.; Zhang, Y.; Qian, W. Development and Validation of an Artificial Intelligence Preoperative Planning and Patient-Specific Instrumentation System for Total Knee Arthroplasty. Bioengineering 2023, 10, 1417. [Google Scholar] [CrossRef] [PubMed]
- Karnuta, J.M.; Shaikh, H.J.F.; Murphy, M.P.; Brown, N.M.; Pearle, A.D.; Nawabi, D.H.; Chen, A.F.; Ramkumar, P.N. Artificial Intelligence for Automated Implant Identification in Knee Arthroplasty: A Multicenter External Validation Study Exceeding 3.5 Million Plain Radiographs. J. Arthroplast. 2023, 38, 2004–2008. [Google Scholar] [CrossRef]
- Yang, J.; Ren, P.; Xin, P.; Wang, Y.; Ma, Y.; Liu, W.; Wang, Y.; Wang, Y.; Zhang, G. Automatic measurement of lower limb alignment in portable devices based on deep learning for knee osteoarthritis. J. Orthop. Surg. 2024, 19, 232. [Google Scholar] [CrossRef]
- Tanner, I.L.; Ye, K.; Moore, M.S.; Rechenmacher, A.J.; Ramirez, M.M.; George, S.Z.; Bolognesi, M.P.; Horn, M.E. Developing a Computer Vision Model to Automate Quantitative Measurement of Hip-Knee-Ankle Angle in Total Hip and Knee Arthroplasty Patients. J. Arthroplast. 2024, 39, 2225–2233. [Google Scholar] [CrossRef]
- Tandel, J.; Shetty, V.; Wagh, Y.; Shekhar, S.; Wagh, A.; Parvathy, J.M.; Karade, V.; Maurya, A. Evaluating axial alignment and knee phenotypes in a young Indian population, using X-rays converted to three-dimensional bone models, and their relevance in total knee arthroplasty. Knee 2024, 48, 197–206. [Google Scholar] [CrossRef]
- Lan, Q.; Li, S.; Zhang, J.; Guo, H.; Yan, L.; Tang, F. Reliable prediction of implant size and axial alignment in AI-based preoperative planning for total knee arthroplasty. Sci. Rep. 2024, 14, 16972. [Google Scholar] [CrossRef]
- Hoffmann, C.; Göksu, F.; Klöpfer-Krämer, I.; Watrinet, J.; Blum, P.; Hungerer, S.; Schröter, S.; Stuby, F.; Augat, P.; Fürmetz, J. High accuracy in lower limb alignment analysis usingconvolutional neural networks, with improvements needed for joint-level metrics. Knee Surg. Sports Traumatol. Arthrosc. 2024, 1–7. [Google Scholar] [CrossRef]
- Park, K.B.; Kim, M.S.; Yoon, D.K.; Jeon, Y.D. Clinical validation of a deep learning-based approach for preoperative decision-making in implant size for total knee arthroplasty. J. Orthop. Surg. Res. 2024, 19, 637. [Google Scholar] [CrossRef]
- Yu, Y.; Cho, Y.J.; Park, S.; Kim, Y.H.; Goh, T.S. Development of an artificial intelligence model for predicting implant size in total knee arthroplasty using simple X-ray images. J. Orthop. Surg. Res. 2024, 19, 516. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kim, S.E.; Kim, B.; Lee, S.; Lee, J.J.; Ro, D.H. A deep learning based automatic two-dimensional digital templating model for total knee arthroplasty. Knee Surg. Relat. Res. 2024, 36, 38. [Google Scholar] [CrossRef] [PubMed]
- Chaudhari, A.S.; Sandino, C.M.; Cole, E.K.; Larson, D.B.; Gold, G.E.; Vasanawala, S.S.; Lungren, M.P.; Hargreaves, B.A.; Langlotz, C.P. Prospective Deployment of Deep Learning in MRI: A Framework for Important Considerations, Challenges, and Recommendations for Best Practices. Magn. Reson. Imaging 2021, 54, 357–371. [Google Scholar] [CrossRef]
- Felländer-Tsai, L. AI ethics, accountability, and sustainability: Revisiting the Hippocratic oath. Acta Orthop. 2020, 91, 1–2. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| First Author, Year | Title | Imaging Type | AI Type | AIM/Application | Main Results |
|---|---|---|---|---|---|
| Chaudari et al., 2020 [7] | Diagnostic Accuracy of Quantitative Multicontrast 5-Minute Knee MRI Using Prospective Artificial Intelligence Image Quality Enhancement | MRI | Deep Learning | Use DL super-resolution augmentation algorithm to enhance a 5-min 3D qDESS MRI sequence that automatically generates multicontrast images and T2 relaxation time maps | Image quality scores were significantly better for conventional MRI vs. qDRESS for all tissues evaluated (p < 0.001), though both methods yielded 92% inter-reader agreement. The qDESS plus T2 method had a higher sensitivity for detecting cartilage lesions (73%) vs. conventional MRI (58%). Automatic T2 relaxation time maps evidenced early chondral degeneration vs. areas that appeared morphologically normal on conventional sequences |
| Lind et al., 2021 [8] | Artificial intelligence for the classification of fractures around the knee in adults according to the 2018 AO/OTA classification system | X-rays | Convolutional Neural Network | Produce detailed knee fracture classification as by the 2018 AO/Orthopedic Trauma Association (AO-OTA) fracture and dislocation compendium. | A weighted mean AUC of 0.87 for proximal tibia fractures, 0.89 for patella fractures and 0.89 for distal femur fractures. Almost ¾ of AUC estimates were above 0.8, out of which more than half reached an AUC of 0.9 or above. |
| Guermazi et al., 2021 [9] | Improving Radiographic Fracture Recognition Performance and Efficiency Using Artificial Intelligence | X-rays | Deep Learning | Interpretation of fracture detection full-size high spatial resolution and multiple radiographic views of the same patient for integration into picture archiving and communications systems. | The system has shown to improve fracture detection sensitivity by 10.4% and is appreciable for all body locations except for shoulder, clavicle and thoracolumbar spine. AI assistance improved the sensitivity and may even improve the specificity of fracture detection by radiologists and non-radiologists, without lengthening reading time. |
| Liu et al., 2021 [10] | Artificial Intelligence to Diagnose Tibial Plateau Fractures: An Intelligent Assistant for Orthopedic Physicians | X-rays | Convolutional Neural Network | Detection of tibial plateau fractures. | The algorithm searched a level of accuracy comparable to orthopedic: 0.91 vs. 0.92 ± 0.03 (p = 0.86). The average time spent for analysis of the AI was 16-fold faster than physician: 0.56 s vs. 8.44 ± 3.26 s. However, at the time of the study, the tool was still unable to replace evaluation of orthopedic physicians |
| Schwarz et al., 2022 [11] | Artificial intelligence enables reliable and standardized measurements of implant alignment in long leg radiographs with total knee arthroplasties | X-rays | Non-specified AI | Evaluation of long leg radiographs (LLR) after total knee arthroplasties (TKA). | AI software was reproducible on 96% and reliable on 92.1% of LLRs with an output and showed excellent reliability in all measured angles (ICC > 0.97) compared to manual measurements. Excellent results were found for primary unconstrained TKA. |
| Smolle et al., 2022 [12] | Artificial intelligence- based computer- aided system for knee osteoarthritis assessment increases experienced orthopaedic surgeons’ agreement rate and accuracy | X-rays | Convolutional Neural Network | Use of AI-enhanced X-rays by means of the Knee Osteoarthritis Labeling Assistant (KOALA). | Increase in senior reader agreement rates for KL grade (2.0-fold), sclerosis (1.42-fold), JSN (1.37-fold) and osteophyte OARSI grades (3.33-fold); reader specificity and accuracy for all features compared to the gold standard. On the other hand, sensitivity only increased for OA diagnosis. With aided analysis, senior readers reached similar agreement and accuracy rates as junior readers, with both surpassing AI performance. |
| Yang C. et al., 2023 [13] | In slope-changing osteotomy one millimeter is not one degree: results of an artificial intelligence-automated software analysis | X-rays | Non-specified AI | Investigation of the assumption that 1mm of wedge height gives 1° of slope correction (1:1) | In trans-tubercle anterior closing wedge, using a wedge height (mm) to slope correction (°) ratio of 1:1 can lead to slight over-correction. |
| Bonnin et al., 2023 [14] | Artificial Intelligence Radiographic Analysis Tool for Total Knee Arthroplasty | X-rays | Convolutional Neural Network | Assistance to surgeons in their postoperative interpretation. | AI tool increased accuracy by 5% and sensitivity by 12% in the detection of interface anomalies. A gain in repeatability for each single surgeon (Light’s kappa 0.17), as well as a gain in reproducibility between surgeons (Light’s kappa +0.1). |
| Kim MS et al., 2023 [15] | Machine Learning for Detecting Total Knee Arthroplasty Implant Loosening on Plain Radiographs. | X-rays | Convolutional Neural Network | Detection of TKA implant loosening. | The CNN algorithm, through transfer learning, shows high accuracy (sensitivity was 100% and the specificity was 97.5%) for detecting the loosening of TKA implants on plain radiographs |
| Pagano et al., 2023 [16] | The Role and Efficiency of an AI-Powered Software in the Evaluation of Lower Limb Radiographs before and after Total Knee Arthroplasty | X-rays | LAMA | Assess AI tool efficiency in measuring axial alignments (MAD, AMA), femoral and tibial angles (mLPFA, mLDFA, mMPTA, mLDTA), and other key measurements including JLCA, HKA. | The tool yielded good to excellent agreement with expert metrics (ICC = 0.78–1.00), it analyzed radiographs two-fold faster radiographs twice as fast (p < 0.001), yet struggled with accuracy for the JLCA (ICC = 0.79, 95% CI = 0.72–0.84), the Mikulicz line (ICC = 0.78, 95% CI = 0.32–0.90), and if patients had a body mass index higher than 30 kg/m2 |
| Liu Z et al., 2023 [17] | Deep Learning for Automated Measurement of Patellofemoral Anatomic Landmarks | CT | Deep Learning | Automatic measurement of patellofemoral anatomy. | Mean absolute error between prediction and ground truth landmark coordinates was 0.20/0.26 cm in the healthy/arthroplasty cohort. There was no statistically significant difference between the model’s predictions and the ground truth measurements for TEA length, TEA-PFA angle, and trochlear medial asymmetry ratio in both cohorts. |
| Wang DY et al., 2024 [18] | A Deep Learning Model Enhances Clinicians’ Diagnostic Accuracy to More Than 96% for Anterior Cruciate Ligament Ruptures on Magnetic Resonance Imaging | MRI | Deep Learning | Increase clinicians’ accuracy—especially among trainees—for anterior cruciate ligament (ACL) ruptures. | The model achieved an area ROC AUC of 0.987 and a sensitivity and specificity of 95.1%. |
| Brejnebøl et al., 2024 [19] | Interobserver Agreement and Performance of Concurrent AI Assistance for Radiographic Evaluation of Knee Osteoarthritis | X-rays | Non-specified AI | Improve X-ray knee OA assessment according to the established KL grading system using the AI tool RBknee (version 2.1; Radiobotics). | AI assistance increased junior readers’ radiographic KOA grading performance. Inter-observer agreement for KL grading across radiologists and orthopedics of various experience levels was higher with AI assistance versus without (κ = 0.77 ± 0.018 [SEM] vs. 0.85 ± 0.013; p < 0.001). Board-certified radiologists achieved almost perfect agreement for KL grading when assisted by AI (κ = 0.90 ± 0.01). |
| Alberti et al., 2025 [20] | Artificial intelligence applied to q-angle measurement: preliminary results on an algorithm based on bounding box | X-Rays | Machine Learning with YOLO | Develop an AI-driven algorithm for identification of key points on X-rays for automatic measurement of Q-angle. | Mean prediction errors by algorithm were smallest for the patella: 4.3 (SD ± 2.8) right and 4.0 (SD ± 2.0) left and was highest for the tibial tuberosity 10.3 (SD ± 7.6) right and 8.5 (SD ± 5.7) left. |
| First Author, Year | Title | Imaging Type | AI Type | AIM/Application | Main Results |
|---|---|---|---|---|---|
| Karnuta et al., 2020 [21] | Artificial Intelligence to Identify Arthroplasty Implants From Radiographs of the Knee | X-rays | Convolutional Neural Network | Implant evaluation | The DL algorithm differentiated between 9 unique knee arthroplasty implants from four manufacturers with near-perfect accuracy. |
| Schock et al., 2021 [22] | Automated Analysis of Alignment in Long-Leg Radiographs by Using a Fully Automated Support System Based on Artificial Intelligence | X-rays | Convolutional Neural Network | Automatize quantitative analysis of lower-extremity alignment. | ICC ranged from 0.918 to 0.995 (r range, p < 0.001), and agreement was almost perfect (intraclass correlation coefficient range, 0.87–0.99). Automatic analysis was faster than the two radiologists’ manual measurements (3 vs. 36 vs. 35 s, p < 0.001). |
| Tack et al., 2021 [23] | Fully automated Assessment of Knee Alignment from Full-Leg X-Rays employing a YOLOv4 And Resnet Landmark regression Algorithm (YARLA): Data from the Osteoarthritis Initiative. | X-rays | YOLO and YARLA | Automatize determination of four parameters in addition to hip–knee–ankle angle from FLRs (varus or valgus deformity | The average deviation of landmarks manually placed by experts and automatically detected by their system was less than 2.0 ± 1.5 mm for all structures. |
| Simon et al., 2021 [24] | Fully automated deep learning for knee alignment assessment in lower extremity radiographs: a cross-sectional diagnostic study | X-rays | Convolutional Neural Network | Automatize clinical angle measurements of commercially available software of mechanical axis HKA, bone length (femur, tibia, full length), laterality discrepancies, and position of orthopedic hardware. | The system showed good reliability in all lengths and angles (ICC ≥ 0.87) and was 130 s faster than clinicians. Overall accuracy was 89.2% when comparing the AI to the manually measured outputs. sMAD for AI vs. observer was between 0.39 and 2.19° for angles and 1.45–5.00 mm for lengths. It also generates radiologist-like reports. |
| Larson et al., 2022 [25] | Artificial Intelligence System for Automatic Quantitative Analysis and Radiology Reporting of Leg Length Radiographs | X-rays | Convolutional Neural Network | Quantification of leg lengths/angles and hardware detection from bilateral lower extremity radiographs using a keypoint-based artificial intelligence system. | AI hardware detection demonstrated an accuracy of 99.8%. Automatic quantitative and qualitative analysis of leg length radiographs using deep learning is feasible and holds potential in improving radiologist workflow. |
| Lambrechts et al., 2022 [26] | Artificial Intelligence Based Patient-Specific Preoperative Planning Algorithm for Total Knee Arthroplasty | N.A. | Machine Learning | Implant size prediction | The average number of corrections a surgeon has to make to the preoperative plan generated using AI was reduced by 39.7% compared to the manufacturer’s default plan. |
| Houserman et al., 2022 [27] | The Viability of an Artificial Intelligence/Machine Learning Prediction Model to Determine Candidates for Knee Arthroplasty | X-rays | Deep Learning | Assess the viability of a knee arthroplasty prediction model using 3-view X-rays (3 different X-ray views (anterior–posterior, lateral, and sunrise) that helps determine if patients with knee pain are candidates for TKA, UKA. | Achieved an accuracy of 87.8% on the holdout test set and a quadratic Cohen’s kappa score of 0.811. The multiclass receiver operating characteristic area under curve score for TKA was calculated to be 0.97; for UKA a score of 0.96 and for No Surgery a score of 0.98 was achieved. An accuracy of 93.8% was achieved for predicting Surgery versus No Surgery and 88% for TKA versus non TKA. |
| Erne et al., 2022 [28] | Automated Artificial Intelligence-Based Assessment of Lower Limb Alignment Validated on Weight-Bearing Pre- and Postoperative Full-Leg Radiographs | X-rays | Convolutional Neural Network | Determine the mMPTA, mLDFA, mLDTA, and FSAmTA | The ICC values of human vs. AI inter-rater reliability analysis ranged between 0.8 and 1.0 preoperatively and between 0.83 and 0.99 postoperatively (all p < 0.001). |
| Bernard de Villeneuve et al., 2022 [29] | An artificial intelligence based on a convolutional neural network allows a precise analysis of the alignment of the lower limb | X-rays | Convolutional Neural Network | Aid surgeons in assessing the preoperative of lower limb deformities and evaluating the appropriate angle for osteotomy | The algorithm showed high accuracy for automated angle measurement, allowing the estimation of limb frontal alignment to the nearest degree. |
| Fernandes et al., 2022 [30] | Accuracy, Reliability, and Repeatability of a Novel Artificial Intelligence Algorithm Converting Two-Dimensional Radiographs to Three-Dimensional Bone Models for Total Knee Arthroplasty | X-rays and CT scans | Non-specified AI | Convert 2D radiographs to 3D bone models. | A high degree of accuracy, reliability, and repeatability for converting 2D radiographs to 3D bone reconstructions similarly to a CT-scan. Mean absolute errors were <2 mm in 9/12 anatomical parameters vs. measurements performed on CTs and manual calipers. All inter-observer and intra-observer correlation coeficients were > 0.90. |
| Steele et al., 2023 [31] | Deep Learning Phenotype Automation and Cohort Analyses of 1946 Knees Using the Coronal Plane Alignment of the Knee Classification | X-rays | Deep Learning | Automated knee phenotyping and analyzed CPAK parameters (including the lateral distal femoral, medial proximal tibia, hip–knee–ankle, and joint line obliquity angles). | No significant difference in the CPAK angles (n = 140, p = 0.66–0.98, ICC = 0.89–0.91) or phenotype classifications made by the algorithm and surgeon (p = 0.96). Women had more valgus CPAK phenotypes than men (p < 0.05). Patients who had higher KL grades at baseline (2 to 4) were more varus using the CPAK classification compared to lower KL grades (0 to 1) (p < 0.05). |
| Huber et al., 2023 [32] | Gender-specific distribution of knee morphology according to CPAK and functional phenotype classification: analysis of 8739 osteoarthritic knees prior to total knee arthroplasty using artificial intelligence | X-rays | LAMA | Analyze the preoperative knee morphology with regard to CPAK and functional phenotype in LLR prior to TKA surgery | Distribution in knee morphology with gender-specific differences highlights the wide range in osteoarthritic knees, characterized by CPAK and phenotype classification and may influence future surgical planning |
| Li S et al., 2023 [33] | Development and Validation of an Artificial Intelligence Preoperative Planning and Patient-Specific Instrumentation System for Total Knee Arthroplasty | CT | NEURAL NETWORK | Develop the AI preoperative planning and PSI system (AIJOINT) for TKA and validate its time savings and accuracy in clinical applications | AIJOINT accurately predicted the component size planning the size of femoral and tibial components was 92.9%, while the accuracy of the conventional method in planning the size of the femoral and tibial components was 42.9% and 47.6%, respectively (p < 0.05). It significantly reduced the time needed for CT processing and PSI design without increasing the time for size planning. |
| Karnuta et al., 2023 [34] | Artificial Intelligence for Automated Implant Identification in Knee Arthroplasty: A Multicenter External Validation Study Exceeding 3.5 Million Plain Radiographs | X-rays | Deep Learning | External validation of knee arthroplasty classification systems | The model discriminated nine implant models with an AUC of 0.99, accuracy 99%, sensitivity of 95%, and specificity of 99% in the external-testing dataset. Excellent internal and external validation, suggesting immediate global scale use in assisting in preoperative planning prior to revision knee arthroplasty. |
| Yang J et al., 2024 [35] | “Automatic measurement of lower limb alignment in portable devices based on deep learning for knee osteoarthritis” | X-rays | Non-specified AI | Lower limb alignment analysis with portable devices (mobile phones) from X-rays. | In both the validation and test sets, the average mean radial errors were 2.778 and 2.447 (p < 0.05). The test results for native knee joints showed that 92.22%, 79.38%, 87.94%, 79.82%, and 80.16% of the joints reached angle deviation < 1° for HKA, JCLA, AMA, mLDFA, and mMPTA. Additionally, for joints with prostheses, 90.14%, 93.66%, 86.62%, 83.80%, and 85.92% of the joints reached that. |
| Tanner et al., 2024 [36] | Developing a Computer Vision Model to Automate Quantitative Measurement of Hip-Knee-Ankle Angle in Total Hip and Knee Arthroplasty Patients | X-rays | Deep Learning | Calculation of HKAA in THA and TKA patients and assessed the agreement between DL-derived HKAAs and manual measurement. | The algorithm could detect the bilateral femoral head, knee, and ankle joints with high precision, even where the femoral head is difficult to visualize. The inter-rater reliability between manual and DL-derived HKAA measurements on the operative leg and nonoperative leg indicated excellent reliability (ICC (2,k) = 0.987 [0.96, 0.99], intraclass correlation (2,k) = 0.987 [0.98, 0.99, respectively]). |
| Tandel J et al., 2024 [37] | Evaluating axial alignment and knee phenotypes in a young Indian population, using X-rays converted to 3D bone models, and their relevance in total knee arthroplasty | X-rays | Non-specified AI | Quantify the percentage of the young healthy Indian population have a HKA = 180° and the percentage of this population with deviation from the neutral HKA. | A significant portion of the normal population had limbs that deviated from neutral HKA. |
| Lan et al., 2024 [38] | Reliable prediction of implant size and axial alignment in AI-based 3D preoperative planning for total knee arthroplasty | X-rays | Neural Network | Assess 3D planning technology on prosthesis size and axial alignment planning in TKA vs. 2D X-ray template measurement. | The accuracy of prosthesis size, VCA and HKA prediction in AI group was significantly higher with AI-based preoperative 3D planning technique than that in 2D group (p < 0.05). |
| Hoffmann et al., 2024 [39] | High accuracy in lower limb alignment analysis using convolutional neural networks, with improvements needed for joint-level metrics | X-rays | Convolutional Neural Network | Implementation of a common planning software (mediCAD® 7.0; mediCAD Hectec GmbH) that allows analysis and preoperative planning. | mediCAD-based analysis demonstrated excellent accuracy for overall lower limb alignment and leg length, but showed significant deviations in joint-level measurements, particularly in cases involving TKA. CNN evaluation demonstrated high consistency in measuring leg length (ICC > 0.99) and lower limb alignment measures of mTFA (ICC > 0.97; RMSE < 1.1°). The mean absolute difference between angular measurements were low for lower limb alignment (mTFA 0.49–0.61°) and high for specific joint angles (aMPFA 3.86–4.50°). |
| Park KB et al., 2024 [40] | Clinical validation of a deep learning-based approach for preoperative decision-making in implant size for total knee arthroplasty | X-rays | Deep Learning | Predict implant sizes based on automatized measurement of the femoral and tibial regions without manual annotation. | Higher agreement levels achieved by the proposed DL model demonstrate its potential as a valuable tool in preoperative decision-making for TKA. Exact accuracies for predicting femoral and tibial implant sizes were 61.54% and 68.38% by surgeon and 89.32% and 90.60% by DL model. |
| Yu Y et al., 2024 [41] | Development of an artificial intelligence model for predicting implant size in total knee arthroplasty using simple X-ray images | X-rays | RESNET | Predict implant size using X-ray images alone without any other data (such as demographics), to achieve a model with strong predictive power. | The model showed micro F1-score 0.91 for femur and 0.87 for tibia. For predicting within ± 1 size, micro F1-score was 0.99 for femur and 0.98 for tibia. |
| Park J et al., 2024 [42] | A deep learning based automatic two-dimensional digital templating model for total knee arthroplasty | X-rays | Non-specified AI | Automatization of implant size prediction. | Exact predictions for 39.5% of fem- oral and 43.2% of tibial components. Allowing a one-size margin of error, 88.9% of predictions were deemed “accurate” for both components. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bertolino, L.; Ranzini, M.B.M.; Favaro, A.; Bardi, E.; Ronzoni, F.L.; Bonanzinga, T. Use of Artificial Intelligence on Imaging and Preoperatory Planning of the Knee Joint: A Scoping Review. Medicina 2025, 61, 737. https://doi.org/10.3390/medicina61040737
Bertolino L, Ranzini MBM, Favaro A, Bardi E, Ronzoni FL, Bonanzinga T. Use of Artificial Intelligence on Imaging and Preoperatory Planning of the Knee Joint: A Scoping Review. Medicina. 2025; 61(4):737. https://doi.org/10.3390/medicina61040737
Chicago/Turabian StyleBertolino, Luca, Marta Bianca Maria Ranzini, Alberto Favaro, Elena Bardi, Flavio Lorenzo Ronzoni, and Tommaso Bonanzinga. 2025. "Use of Artificial Intelligence on Imaging and Preoperatory Planning of the Knee Joint: A Scoping Review" Medicina 61, no. 4: 737. https://doi.org/10.3390/medicina61040737
APA StyleBertolino, L., Ranzini, M. B. M., Favaro, A., Bardi, E., Ronzoni, F. L., & Bonanzinga, T. (2025). Use of Artificial Intelligence on Imaging and Preoperatory Planning of the Knee Joint: A Scoping Review. Medicina, 61(4), 737. https://doi.org/10.3390/medicina61040737