1. Background
Malaria is an ancient disease and a major public health concern in Africa. Approximately 3.2 billion people remain at risk of contracting malaria, and 214 million new cases of malaria were reported in 2015, resulting in 428,000 deaths. Most cases (88%) occurred in the WHO African Region, followed by the South-East Region (10%) and WHO Eastern Mediterranean Region (2%). Approximately 80% of cases occurred in just 15 countries, mainly located in Africa. Combined, these high-burden countries recorded a slower than average reduction in malaria incidence and mortality [
1], and Mozambique was among them.
Mozambique was recently ranked fifth in Africa for the number of malaria cases [
2]. The disease is a major cause of morbidity and mortality, especially among children [
3], and the entire population is at risk of contracting the disease since it is endemic with seasonal peaks during and after the rainy season, which is between November and March [
4,
5].
Eradicating malaria is, therefore, one of Mozambique’s main priorities and is recognized as critical to achieve the 2030 Agenda for Sustainable Development [
6]. The environment and climate conditions highly influence malaria transmission, although their effects are often not linear. The malaria-climate relationship varies among areas covered by different agro-ecological zones [
6]; thus, resources for control have to be spread over time and space. An estimated 80 to 90% of malaria cases are related to environmental factors [
7,
8,
9]. The level of prevalence can be predicted based on the established relationship between malaria prevalence and environmental data.
Temperature affects the development of malaria as the parasite does not develop below 18 °C and over 40 °C [
10,
11]. The highest proportion of vectors surviving the incubation period is observed at temperatures between 28 °C and 32 °C [
12]. Precipitation is another key player in malaria occurrence; increased precipitation can provide more breeding sites for mosquitoes, but excess rain can also destroy breeding sites [
13,
14]. Altitude can indirectly influence the distribution and spread of malaria via its effect on temperature. For every 200 m increase in altitude, the temperature decreases by 1 °C [
15]. Highlands are colder and lowlands are warmer; at certain altitudes, malaria transmission does not occur due to extreme temperatures, which are not favourable to the mosquito or the life cycle of the parasite [
10]. For smaller regions, topography remains the single most important aspect that defines large scale differences in malaria risk because climate variables change little over the limited range of latitude [
16]. In Mozambique and Malawi, elevation is associated with malaria prevalence; at an elevation of <650 m, the prevalence was higher than that between 650 and 1100 mm [
17,
18].
Slope combined with precipitation levels at a certain location may influence the dispersion of malaria. Flat areas on the ground are more prone to accumulate water, creating dam rainwater and increasing the risk of malaria. In Ghana, swampy areas and banana production in the proximity of villages are strong predictors of a high malaria incidence [
19].
Land cover is another factor in malaria occurrence. In Kenya, the association between land cover type and presence of anopheline larvae was statistically significant; overall, the highest proportions of anopheline-positive habitats occurred in pastures (33%) and farmlands (32%), followed by swamp habitats (23%) [
20]. In Ghana, an increase in a forested area of 10% was associated with a 47% decrease in malaria incidence. Different cultivations in the vicinity of homesteads were related to childhood malaria in rural areas [
19,
20]. Marsh clearance, dam construction and crop cultivation increase the risk of malaria at the local scale. Open, treeless habitats have a lower malaria transmission risk compared with forest sites [
16].
The effectiveness of intervention measures against malaria can be determined by the Euclidian distance of a place from roads. In Zambia, for every 500 m increase in distance from the road, there was a corresponding 5% increase in malaria-positive households [
21]. In Kenya, roads were found to have the fewest number of anopheline habitats (15%), whereas habitats in forests had an 18% rate [
20].
The distribution of water bodies is a major factor that influences malaria occurrence and case distributions. Water bodies play a very important role as larval breeding sites for malaria mosquitoes [
22]. Therefore, identification of water body sites is a direct indicator for malaria risk occurrences. The Euclidian distance to a water body is a determinant of the malaria risk incidence [
23]. A study carried out in China indicated that populations living within 60 m of water bodies had a higher risk of contracting malaria [
24].
In terms of malaria breeding, the following statement was made in 1934: “it may safely be inferred that the influence of any production from breeding place within 0.81 km radius will be felt there in, at radii of 1.61 km the influence may be doubtful, and ordinarily at radii of more than 1.61 km the influence may be expected to be nil” [
25]. Recent studies have indicated that mosquitoes fly no more than 170 m after ingesting a blood meal [
26] and that a hungry mosquito will fly up to 1.5 km [
27].
In Chimoio, a weak positive correlation was found between malaria cases and population density [
28]. The mosquito breeding, feeding, and resting behaviours are often associated with vegetation [
18].
A number of vegetation indices have been used in remote sensing, but the most used index to enhance the vegetation areas is the Normalized Difference Vegetation Index (NDVI). The measurement of NDVI is from −1 to 1; if a value is close to 0, there is little vegetation in the area. When the value is close to 1, there is more vegetation in the region [
16]. In Brazil, most domiciles with more than five notified cases are located near areas with high NDVI values, and variations in the photosynthetic productivity of vegetation are strongly related to variations in malaria transmission [
29].
Chimoio is the capital of Manica Province in the Centre of Mozambique. Very little research on malaria has been carried out in Chimoio. Malaria is increasing in the suburbs, and urban areas present fewer malaria cases than rural areas. The annual overall average of malaria incidence is 20.1%, and the Attributable Fraction (AF) of malaria is 16%. Children under five are three times more prone to malaria than adults [
28], and 11.7% of the total annual deaths are due to malaria [
30].
The two most important climate factors that influence malaria in Chimoio were found to be the relative humidity and minimum temperature, and they showed positive high correlations with climate [
8]. In regard to the spatial epidemiology of malaria, recent studies have benefited from the great progress in the development of Geographic Information Systems (GIS). The health practitioner and/or researcher’s ability to locate the precise position of a disease in their area allows for the creation of maps of the spatial variability, and they can incorporate as many variables as can be measured [
31].
Precision public health strategies are based on a specific site by observing, measuring and responding to inter and intra-region variability in malaria trends. This makes statistical and computational treatments quite involved and can lead to decision support systems that can help to eradicate malaria, optimize resources and minimize the impact on the environment [
32]. The decisions can be in areas such as the right time and place for spraying, correct site to build a water body, correct time and place for drainage and other relevant activities for malaria control and eradication.
Targeting vector control in high-risk areas, focusing on asymptomatic and symptomatic infections and managing importation risk are needed to control and eradicate the disease. High spatial and temporal resolution maps of malaria risk can support all of these activities [
33].
Risk maps can be used for Precision Public Health, but the maps available for malaria were produced at national, regional or continental magnitudes, such as MARA [
34,
35], and have a limited operational use to support local programme activities.
Malaria risk maps of the country, especially of Chimoio, have not been produced, and they are urgently needed to identify areas at risk by the Public Precision Health approach. By using spatial modelling techniques with GIS, the research goal of this study was to map and model malaria risk areas using socio-demographic, climate, and clinical variables in Chimoio, Mozambique.
3. Results
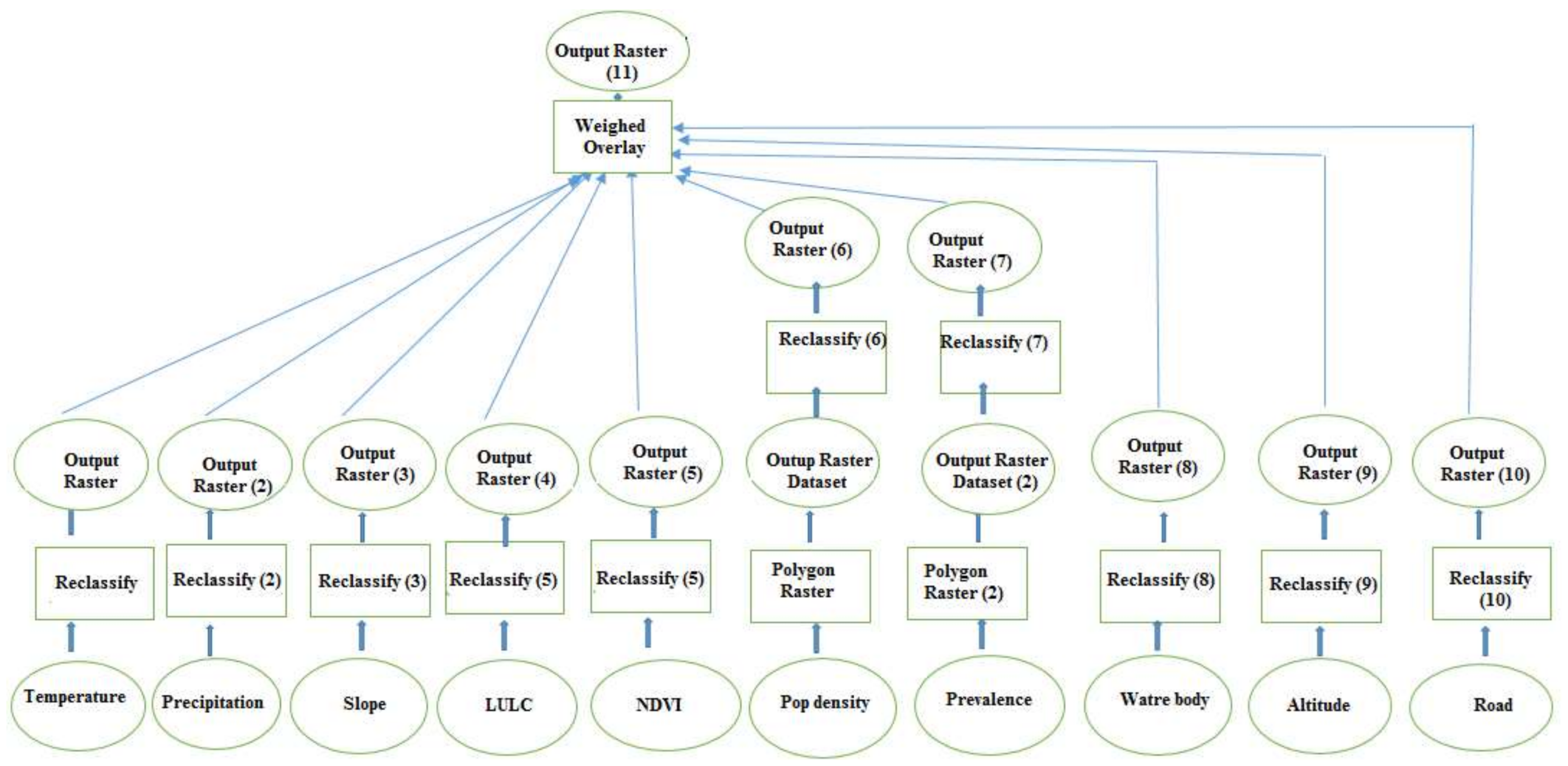
Table 3 shows the 10 × 10 comparison matrix of the malaria risk factors used in the study. A value of 1 means that the factors under comparison have the same weight and that they equally affect the malaria occurrence. A value of five means the factor in the column is five times more important in malaria risk occurrence than the comparison in the row.
The weights of each factor used for the spatial model to produce the malaria risk map are presented in
Table 4. The average temperature (22.4%) and precipitation (20.8%) presented the highest weights, followed by the distance to water body (12.3%) and altitude (10.4%), land use and land cover (8.2%), slope (7.3%), pop dens and malaria prevalence (5.1%), NDVI (4.7%) and distance to road (3.8%). The consistency index for the pair-wise matrix was 9%.
The special model to produce the malaria risk map formula was:
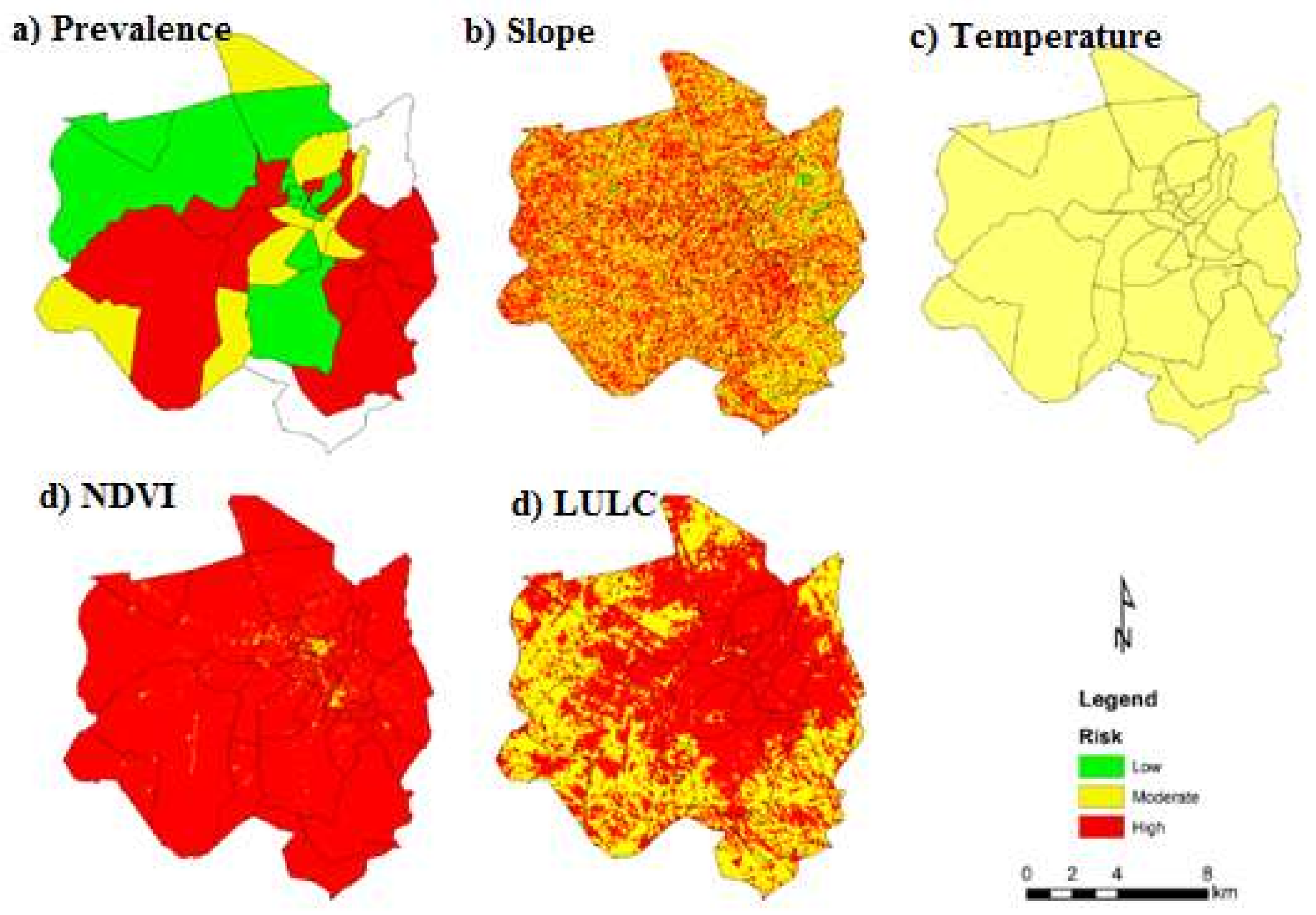
Figure 3 presents the maps of malaria prevalence, slope, temperature, NDVI and LULC. In terms of malaria prevalence, 42% of Chimoio’s areas presented a low risk, 17% a moderate risk and 41% a high risk. For the slope, 2% of the area presented a low risk, 52% a moderate risk and 46% a high risk. For the average temperature, 100% of Chimoio presented a moderate risk. For NDVI, 5% of Chimoio presented a low risk, 12% a moderate risk and 88% a high risk. For LULC, 39% of Chimoio presented a low risk, 4% a moderate risk and 43% a high risk.
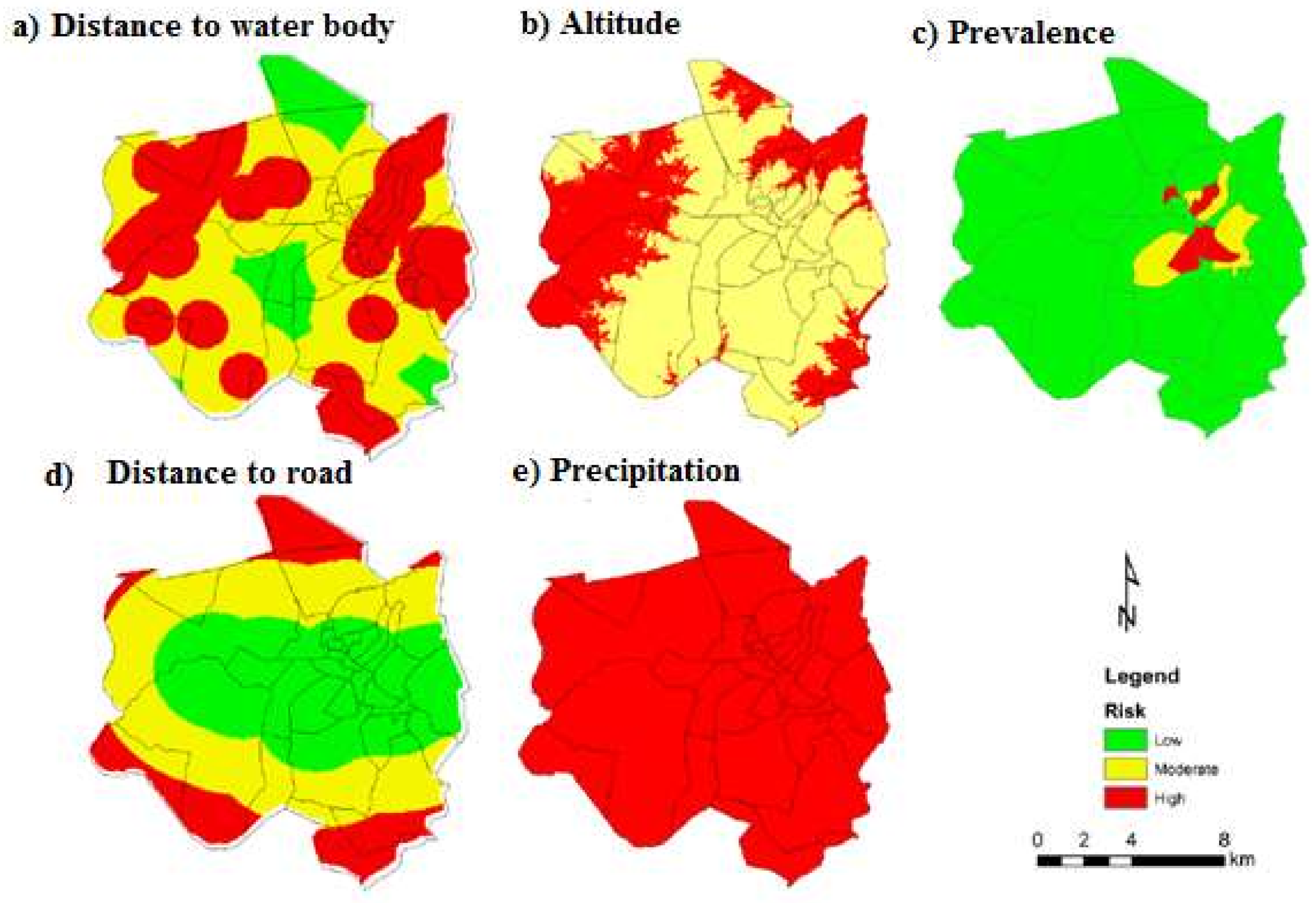
Figure 4 presents the maps of precipitation, altitude, distance to a water body (DTWB), distance to road (DTR), and population density (person/km
2). For precipitation, Chimoio presented 100% high-risk areas. For altitude, 34% of Chimoio presented a moderate risk and 66% a high risk. For DTWD, 44% of Chimoio presented a low risk, 40% a moderate risk and 16% a high risk. For DTR, 40% of the area presented a low risk, 43% a moderate risk and 17% a high risk. For population density, 92% of Chimoio presented a low risk, 5% a moderate risk and 3% a high-risk areas.
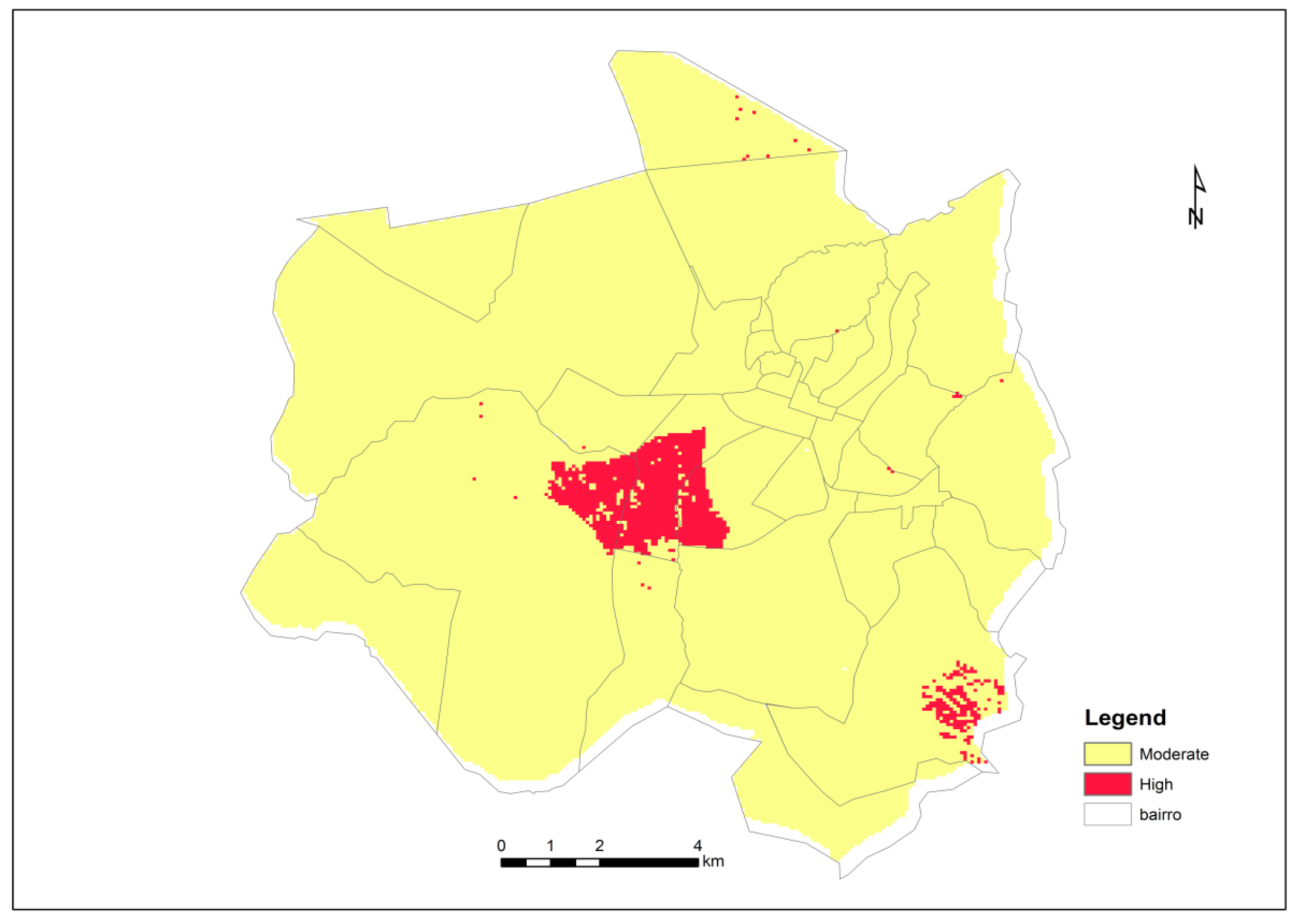
Figure 5 presents the Chimoio map risk for malaria after consolidation of the weighted malaria risk factors used in the present study. Chimoio presented 0% of the area with low risk, 96% with moderate risk and 4% with high risk. The map shows that the central and south-west residential areas, namely, Centro Hipico, Trangapsso, Bairro 5 and 1° de Maio, while the rest of the residential areas had a moderate risk of malaria.
4. Discussion
Few studies have included ten risk factor variables in geostatistical models for malaria risk mapping. In this study, 100% of Chimoio presented high-risk areas for precipitation, indicating that precipitation is a key player in malaria occurrence and that increased precipitation provides more breeding sites for mosquitoes [
9,
12,
13,
14]. For NDVI, 88% of the area presented high risk. Variation of the photosynthetic productivity of vegetation is strongly related to variation in malaria transmission. Similar NDVI results to those found in this study were reported in Brazil [
29]. Altitude indicated that 66% of the area was at high risk. At altitudes over 1000 m, malaria transmission decreases due to extreme temperatures, which are not favourable to the mosquito or parasite life cycle [
10]. The altitude of Chimoio varies from 513 and 786 m and seems to be favourable for malaria transmission. Similar results were reported in Mozambique [
18,
28], Swaziland and Malawi [
17,
22].
In this study, 100% of the Chimoio area presented a moderate risk for temperature and 52% for slope. The highest proportion of vectors surviving the incubation period is observed at temperatures between 28 °C and 32 °C [
12], and the annual average temperature in Chimoio is 21.5 °C [
38]. These observations can explain why the entire Chimoio area is at moderate risk. The slope together with the precipitation levels at a certain location may influence the dispersion of malaria. Flat areas on the ground are more prone to accumulate water, creating rainwater dams, increasing the risk of malaria [
18]. The results of this study are similar to studies in Mozambique [
51,
52] and Ghana [
19].
In this study, 92% of Chimoio presented a low risk for population density, 44% for distance to water bodies, and 42% for malaria prevalence and distance to the road. A previous study in Chimoio found a weaker relationship between malaria prevalence and population density [
27] compared to studies in China [
25].
In this study, climatic factors, mean temperature and precipitation presented the highest weights, followed by DTWB (12.3%) and altitude (10.4%), and the other climatic factors presented the least weights. The Mozambique risk map was similar to the findings of this study [
34,
53,
54]. Similar results were also reported in other studies in Zimbabwe, Tanzania, and Latin America [
16,
46,
47,
48].
The malaria risk map produced by this study differed in many ways from other available models. The area is small (174 km2), and the model used ten risk factor variables. The model also used high, sharp and fine spatial and temporal resolutions of risk factors and included climate variable data that impacted factors that affect mosquito proliferation. The model also included human-induced variables, such as the distance from roads, LULC changes, and clinical data. The model is reasonably scaled to present the variance in the malaria risk at the micro-scale level. Few studies have included ten risk factor variables in geostatistical models for malaria risk mapping. Similarly, this approach can also be applied to model and prediction of other environment-driven diseases.
One limitation of the current study is that it does not account for seasonal effects which can impact on disease transmission such as, temporal changes is malaria transmission risk, the environmental conditions that are suited to key stages of the mosquito life cycle, and mosquito numbers that varies throughout the year. Despite the limitations, one great strength of the study is that this is the first specific study in malaria mapping in Chimoio.
5. Conclusions
The weights used in this map are consistent with those from several studies, and the map is reliable. The entire population of Chimoio is at a risk of contracting malaria; 96% have a moderate risk and 4% have a high risk. Trees in the Chimoio streets and households are likely resting areas for mosquitoes.
Precise estimation of malaria risk has important precision public health implications and the planning of effective control measures, such as the right time and place to spray to combat vectors, right time to prune trees from homesteads, distribution of bed nets, correct site to build a water body, correct time and place for drainage and other relevant activities for malaria control and eradication.
This study demonstrated the importance of the use of GIS and remote sensing in predicting, mapping and modelling the malaria risk in the Chimoio municipality. More studies should be carried out, such as on bed net usage, the relationship between household presence of trees and malaria and others.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




