Trust in the Work Environment and Cardiovascular Disease Risk: Findings from the Gallup-Sharecare Well-Being Index




Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population
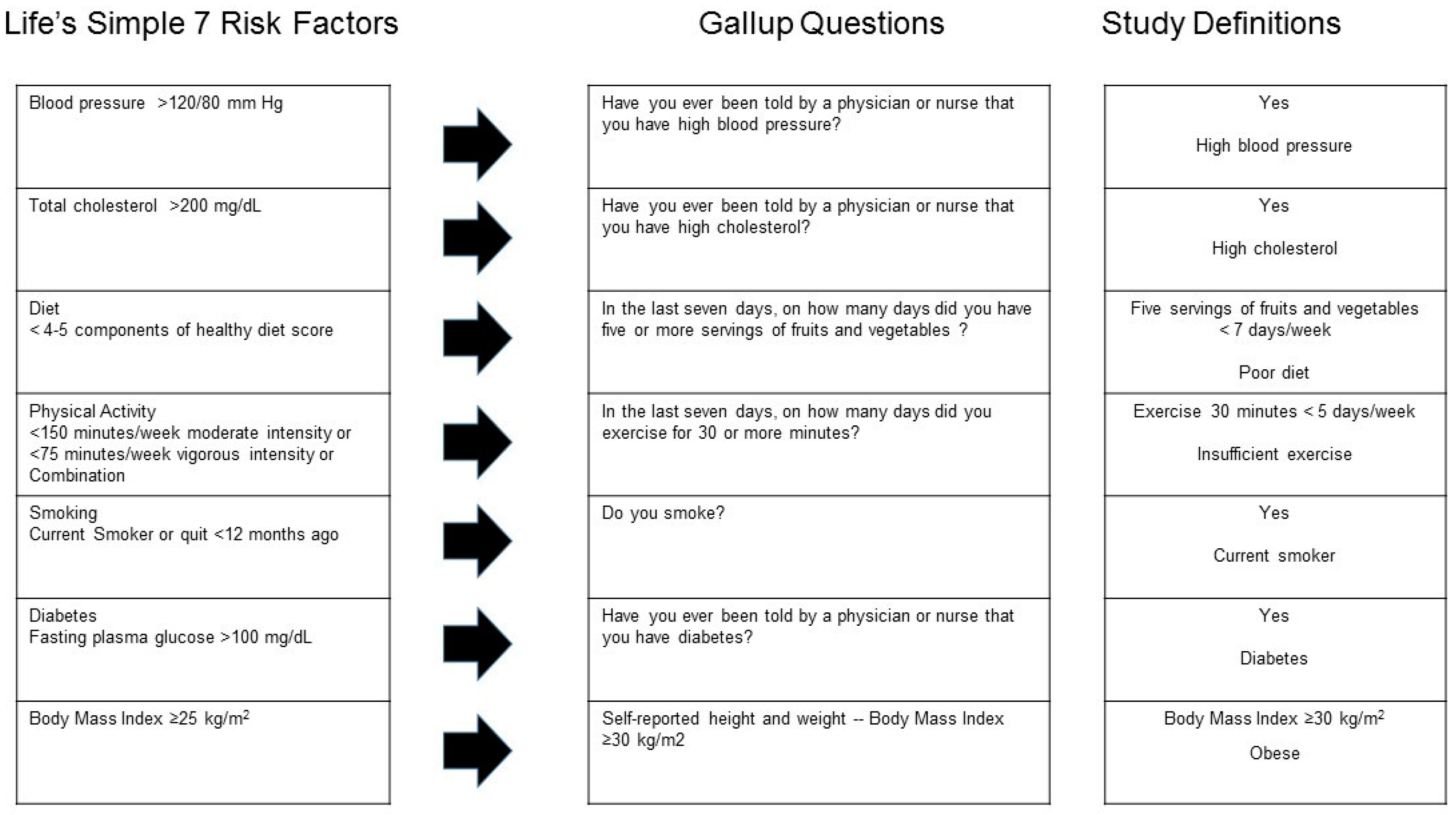
2.3. Measures
2.4. Data Analysis
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. CDC Heart Disease Facts. 2016. Available online: https://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_heart_disease.htm (accessed on 17 April 2018).
- Heidenreich, P.A.; Trogdon, J.G.; Khavjou, O.A.; Butler, J.; Dracup, K.; Ezekowitz, M.D.; Finkelstein, E.A.; Hong, Y.; Johnston, S.C.; Khera, A.; et al. Forecasting the future of cardiovascular disease in the United States: A policy statement from the American Heart Association. Circulation 2011, 123, 933–944. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J. American Heart Association Statistics, C.; Stroke Statistics, S. ‘Heart disease and stroke statistics—2015 update: A report from the American Heart Association. Circulation 2015, 131, e29–e322. [Google Scholar] [PubMed]
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; de Ferranti, S.; Després, J.P.; Fullerton, H.J.; Howard, V.J.; et al. American Heart Association Statistics C, Stroke Statistics S: Heart disease and stroke statistics—2017 update: A reportfFrom the American Heart Association. Circulation 2017, 135, e146–e603. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.M.; Hong, Y.; Labarthe, D.; Mozaffarian, D.; Appel, L.J.; Van Horn, L.; Greenlund, K.; Daniels, S.; Nichol, G.; Tomaselli, G.F.; et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: The American Heart Association’s strategic impact goal through 2020 and beyond. Circulation 2010, 121, 586–613. [Google Scholar] [CrossRef] [PubMed]
- Shay, C.M.; Gooding, H.S.; Murillo, R.; Foraker, R. Understanding and Improving Cardiovascular Health: An Update on the American Heart Association’s Concept of Cardiovascular Health. Prog. Cardiovasc. Dis. 2015, 58, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Backé, E.M.; Seidler, A.; Latza, U.; Rossnagel, K.; Schumann, B. The role of psychosocial stress at work for the development of cardiovascular diseases: A systematic review. Intl. Arch. Occup. Environ. Health 2012, 85, 67–79. [Google Scholar] [CrossRef]
- Belkic, K.L.; Landsbergis, P.A.; Schnall, P.L.; Baker, D. Is job strain a major source of cardiovascular disease risk? Scand. J. Work Environ. Health 2004, 30, 85–128. [Google Scholar] [CrossRef] [Green Version]
- Choi, B.K.; Schnall, P.; Landsbergis, P.; Dobson, M.; Ko, S.; Gomez-Ortiz, V.; Juárez-Garcia, A.; Baker, D. Recommendations for individual participant data meta-analyses on work stressors and health outcomes: Comments on IPD-Work Consortium papers. Scand. J. Work Environ. Health 2015, 41, 299–311. [Google Scholar] [CrossRef]
- Kasl, S.V. The influence of the work environment on cardiovascular health: A historical, conceptual, and methodological perspective. J. Occup. Health Psychol. 1996, 1, 42–56. [Google Scholar] [CrossRef]
- Kivimäki, M.; Kawachi, I. Work stress as a risk factor for cardiovascular disease. Curr. Cardiol. Rep. 2015, 17, 630. [Google Scholar] [CrossRef]
- Kivimäki, M.; Virtanen, M.; Elovainio, M.; Kouvonen, A.; Vaananen, A.; Vahtera, J. Work stress in the etiology of coronary heart disease—A meta-analysis. Scand. J. Work Environ. Health 2006, 32, 431–442. [Google Scholar] [CrossRef] [PubMed]
- Steptoe, A.; Kivimäki, M. Stress and cardiovascular disease: An update on current knowledge. Ann. Rev. Public Health 2013, 34, 337–354. [Google Scholar] [CrossRef]
- Szerensci, K.; van Amelsvoort, L.; Viechtbauer, W.; Mohren, D.; Prins, M.; Kant, I. The association between study characteristics and outcome in the relation between job stress and cardiovascular disease: A multilevel meta-regression analysis. Scand. J. Work Environ. Health 2012, 38, 489–502. [Google Scholar] [CrossRef] [PubMed]
- Theorell, T. Commentary triggered by the Individual Participant Data Meta-Analysis Consortium study of job strain and myocardial infarction risk. Scand. J. Work Environ. Health 2014, 40, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Toivanen, S. Social determinants of stroke as related to stress at work among working women: A literature review. Stroke Res. Treat. 2012, 2012, 873678. [Google Scholar] [CrossRef] [PubMed]
- Gilbert-Ouimet, M.; Trudel, X.; Brisson, C.; Milot, A.; Vezina, M. Adverse effects of psychosocial work factors on blood pressure: Systematic review of studies on demand-control-support and effort-reward imbalance models. Scand. J. Work Environ. Health 2014, 40, 109–132. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.V.; Hall, E.M. Job strain, work place social support, and cardiovascular disease: A cross-sectional study of a random sample of the Swedish working population. Am. J. Public Health 1988, 78, 1336–1342. [Google Scholar] [CrossRef] [PubMed]
- Karasek, R. Job demands, job decision latitude, and mental strain: Implications for job redesign. Adm. Sci. Q. 1979, 24, 285–308. [Google Scholar] [CrossRef]
- Karasek, R.; Theorell, T. Healthy Work: Stress, Productivity, and the Reconstruction of Working Life; Basic Books: New York, NY, USA, 1990; ISBN 978-0465028979. [Google Scholar]
- Nieuwenhuijsen, K.; Bruinvels, D.; Frings-Dresen, M. Psychosocial work environment and stress-related disorders, a systematic review. Occup. Med. 2010, 60, 277–286. [Google Scholar] [CrossRef] [Green Version]
- Schaufeli, W.; Bakker, A.; Salanova, M. The measurement of work engagement with a short questionnaire. A cross-national study. Educ. Psychol. Meas. 2006, 66, 701–716. [Google Scholar] [CrossRef]
- Siegrist, J. Adverse health effects of high-effort/low-reward conditions. J. Occup. Health Psychol. 1996, 1, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, M.; Heikkila, K.; Jokela, M.; Ferrie, J.E.; Batty, G.D.; Vahtera, J.; Kivimäki, M. Long working hours and coronary heart disease: A systematic review and meta-analysis. Am. J. Epidemiol. 2012, 176, 586–596. [Google Scholar] [CrossRef] [PubMed]
- Bakker, A.B.; Demerouti, E. The Job Demands-Resources model: State of the art. J. Manag. Psychol. 2007, 22, 309–328. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E.; Euwema, M.C. Job resources buffer the impact of job demands on burnout. J. Occup. Health Psycholol. 2005, 10, 170–180. [Google Scholar] [CrossRef]
- Demerouti, E.; Bakker, A.B.; Nachreiner, F.; Schaufeli, W.B. The job demands-resources model of burnout. J. Appl. Psychol. 2001, 86, 499–512. [Google Scholar] [CrossRef] [PubMed]
- Black, J.K.; Belanos, G.M.; Whitikaer, A.C. Resilience, work engagement and stress reactivity in a middle-aged manual worker population. Int. J. Psychophysiol. 2017, 116, 9–15. [Google Scholar] [CrossRef]
- Colquitt, J.A.; Conlon, D.E.; Wesson, M.J.; Porter, C.O.; Ng, K.Y. Justice at the millennium: A meta-analytic review of 25 years of organizational justice research. J. Appl. Psychol. 2001, 86, 425–445. [Google Scholar] [CrossRef]
- De Vogli, R.; Ferrie, J.E.; Chandola, T.; Kivimäki, M.; Marmot, M.G. Unfairness and health: Evidence from the Whitehall II Study. J. Epidemiol. Community Health 2007, 61, 513–518. [Google Scholar] [CrossRef]
- Elovainio, M.; Kivimäki, M.; Vahtera, J. Organizational justice: Evidence of a new psychosocial predictor of health. Am. J. Public Health 2002, 92, 105–108. [Google Scholar] [CrossRef]
- Inoue, A.; Kawakami, N.; Eguchi, H.; Miyaki, K.; Tsutsumi, A. Organizational justice and physiological coronary heart disease risk factors in japanese employees: A cross-sectional study. Int. J. Behav. Med. 2015, 22, 775–785. [Google Scholar] [CrossRef]
- Kivimäki, M.; Ferrie, J.E.; Brunner, E.; Head, J.; Shipley, M.J.; Vahtera, J.; Marmot, M.G. Justice at work and reduced risk of coronary heart disease among employees: The Whitehall II Study. Arch. Intern. Med. 2005, 165, 2245–2251. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.; Mesa-Frias, M.; Nuesch, E.; Hargreaves, J.; Prieto-Merino, D.; Bowling, A.; Smith, G.D.; Ebrahim, S.; Dale, C.E.; Casas, J.P. Social capital, mortality, cardiovascular events and cancer: A systematic review of prospective studies. Int. J. Epidemiol. 2014, 43, 1895–1920. [Google Scholar] [CrossRef] [PubMed]
- Coleman, J. Foundations of Social Theory; Harvard University Press: Cambridge, MA, USA, 1990. [Google Scholar]
- Hayami, Y. Social capital, human capital and the community mechanism: Toward a conceptual framework for economists. J. Dev. Stud. 2009, 45, 96–123. [Google Scholar] [CrossRef]
- Murayama, H.; Fujiwara, Y.; Kawachi, I. Social capital and health: A review of prospective multilevel studies. J. Epidemiol. 2012, 22, 179–187. [Google Scholar] [CrossRef]
- Putnam, R. Making Democracy Work: Civic Traditions in Modern Italy; Princeton University Press: Princeton, NJ, USA, 1993; ISBN 9780691037387. [Google Scholar]
- Berkman, L.F.; Kawachi, I. Social Epidemiology; Oxford University Press: New York, NY, USA, 2000. [Google Scholar]
- Zischka, L. Valuing Social capital by the Resources People Allocate to One Another. J. Int. Dev. 2013, 25, 609–625. [Google Scholar] [CrossRef]
- Giordano, G.N.; Ohlsson, H.; Lindström, M. Social capital and health-purely a question of context? Health Place 2011, 17, 946–953. [Google Scholar] [CrossRef]
- Pattussi, M.P.; Olinto, M.T.; Canuto, R.; da Silva Garcez, A.; Paniz, V.M.; Kawachi, I. Workplace social capital, mental health and health behaviors among Brazilian female workers. Soc. Psychiatry Psychiat. Epidemiol. 2016, 51, 1321–1330. [Google Scholar] [CrossRef] [PubMed]
- Samuel, L.J.; Commodore-Mensah, Y.; Himmelfarb, C.R. Developing behavioral theory with the systematic integration of community social capital concepts. Health Educ. Behav. 2014, 41, 359–375. [Google Scholar] [CrossRef] [PubMed]
- Kawachi, I.; Kennedy, B.P.; Glass, R. Social capital and self-rated health: A contextual analysis. Am. J. Public Health 1999, 89, 1187–1193. [Google Scholar] [CrossRef]
- Oksanen, T.; Kawachi, I.; Kouvonen, A.; Takao, S.; Suzuki, E.; Virtanen, M.; Pentti, J.; Kivimäki, M.; Vahtera, J. Workplace determinants of social capital: Cross-sectional and longitudinal evidence from a Finnish cohort study. PLoS ONE 2013, 8, e65846. [Google Scholar] [CrossRef]
- Oksanen, T.; Kouvonen, A.; Kivimäki, M.; Pentti, J.; Virtanen, M.; Linna, A.; Vahtera, J. Social capital at work as a predictor of employee health: Multilevel evidence from work units in Finland. Soc. Sci. Med. 2008, 66, 637–649. [Google Scholar] [CrossRef] [PubMed]
- Sundquist, J.; Johansson, S.E.; Yang, M.; Sundquist, K. Low linking social capital as a predictor of coronary heart disease in Sweden: A cohort study of 2.8 million people. Soc. Sci. Med. 2006, 62, 954–963. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, E.; Takao, S.; Subramanian, S.V.; Komatsu, H.; Doi, H.; Kawachi, I. Does low workplace social capital have detrimental effect on workers’ health? Soc. Sci. Med. 2010, 70, 1367–1372. [Google Scholar] [CrossRef]
- Lindström, M.; Giordano, G.N. Changes in social capital and cigarette smoking behavior over time: A population-based panel study of temporal relationships. Nicotine Tob. Res. 2016, 18, 2106–2114. [Google Scholar] [CrossRef] [PubMed]
- Tsuboya, T.; Tsutsumi, A.; Kawachi, I. Null association between workplace social capital and body mass index. Results from a four-wave panel survey among employees in Japan (J-HOPE study). Soc. Sci. Med. 2016, 150, 1–7. [Google Scholar] [CrossRef]
- Ehsan, A.M.; De Silva, M.J. Social capital and common mental disorder: A systematic review. J. Epidemiol. Community Health 2015, 69, 1021–1028. [Google Scholar] [CrossRef]
- Tsuboya, T.; Tsutsumi, A.; Kawachi, I. Change in psychological distress following change in workplace social capital: Results from the panel surveys of the J-HOPE study. Occup. Environ. Med. 2015, 72, 188–194. [Google Scholar] [CrossRef]
- Johnson, C.M.; Sharkey, J.R.; Dean, W.R. Eating behaviors and social capital are associated with fruit and vegetable intake among rural adults. J. Hunger. Environ. Nutr. 2010, 5, 302–315. [Google Scholar] [CrossRef]
- Lindström, M. Social capital, the miniaturization of community and high alcohol consumption: A population-based study. Alcohol Alcohol. 2005, 40, 556–562. [Google Scholar] [CrossRef]
- Lindström, M. Social capital, political trust and purchase of illegal liquor: A population-based study in southern Sweden. Health Policy 2008, 86, 266–275. [Google Scholar] [CrossRef]
- Weitzman, E.R.; Chen, Y.Y. Risk modifying effect of social capital on measures of heavy alcohol consumption, alcohol abuse, harms, and secondhand effects: National survey findings. J. Epidemiol. Community Health 2005, 59, 303–309. [Google Scholar] [CrossRef]
- Ball, K.; Cleland, V.J.; Timperio, A.F.; Salmon, J.; Giles-Corti, B.; Crawford, D.A. Love thy neighbour? Associations of social capital and crime with physical activity amongst women. Soc. Sci. Med. 2010, 71, 807–814. [Google Scholar] [CrossRef] [PubMed]
- Lindström, M. Social capital, desire to increase physical activity and leisure-time physical activity: A population-based study. Public Health 2011, 125, 442–447. [Google Scholar] [CrossRef] [Green Version]
- Lindström, M.; Moghaddassi, M.; Merlo, J. Social capital and leisure time physical activity: A population based multilevel analysis in Malmo, Sweden. J. Epidemiol. Community Health 2003, 57, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Oksanen, T.; Kivimäki, M.; Kawachi, I.; Subramanian, S.V.; Takao, S.; Suzuki, E.; Kouvonen, A.; Pentti, J.; Salo, P.; Virtanen, M.; et al. Workplace social capital and all-cause mortality: A prospective cohort study of 28,043 public-sector employees in Finland. Am. J. Public Health 2011, 101, 1742–1748. [Google Scholar] [CrossRef] [PubMed]
- Giordano, G.N.; Lindström, M. The impact of social capital on changes in smoking behaviour: A longitudinal cohort study. Eur. J. Public Health 2011, 21, 347–354. [Google Scholar] [CrossRef]
- Kouvonen, A.; Oksanen, T.; Vahtera, J.; Vaananen, A.; De Vogli, R.; Elovainio, M.; Pentti, J.; Leka, S.; Cox, T.; Kivimäki, M. Work-place social capital and smoking cessation: The Finnish Public Sector Study. Addiction 2008, 103, 1857–1865. [Google Scholar] [CrossRef] [PubMed]
- Lindström, M. Social capital, political trust and daily smoking and smoking cessation: A population-based study in southern Sweden. Public Health 2009, 123, 496–501. [Google Scholar] [CrossRef]
- Nieminen, T.; Prattala, R.; Martelin, T.; Harkanen, T.; Hyyppa, M.T.; Alanen, E.; Koskinen, S. Social capital, health behaviours and health: A population-based associational study. BMC Public Health 2013, 13, 613. [Google Scholar] [CrossRef]
- Väänänen, A.; Kouvonen, A.; Kivimäki, M.; Oksanen, T.; Elovainio, M.; Virtanen, M.; Pentti, J.; Vahtera, J. Workplace social capital and co-occurrence of lifestyle risk factors: The Finnish Public Sector Study. Occup. Environ. Med. 2009, 66, 432–437. [Google Scholar] [CrossRef]
- Tamers, S.L.; Goetzel, R.; Kelly, K.M.; Luckhaupt, S.E.; Nigam, J.A.; Pronk, N.P.; Rohlman, D.S.; Baron, S.; Brosseau, L.; Bushnell, P.T.; et al. Research methodologies for Total Worker Health®: Proceedings from a workshop. J. Occup. Environ. Med. 2018, 6, 968–978. [Google Scholar] [CrossRef] [PubMed]
- Werbel, J.; Henriques, P. Different views of trust and relational leadership: Supervisor and subordinate perspectives. J. Manag. Psychol. 2009, 24, 780–796. [Google Scholar] [CrossRef]
- Nienaber, A.; Romeike, P.; Searle, R.; Schewe, G. A qualitative meta-analysis of trust in supervisor-subordinate relationships. J. Manag. Psychol. 2015, 30, 507–534. [Google Scholar] [CrossRef]
- Schill, A.L. Advancing well-being through Total Worker Health®. Workplace Health Saf. 2017, 65, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Quality of Worklife Questionnaire. 2013. Available online: http://www.cdc.gov/niosh/topics/stress/qwlquest.html (accessed on 17 April 2018).
- University of Michigan. ‘Health and Retirement Study’. Available online: http://hrsonline.isr.umich.edu (accessed on 17 April 2018).
- National Center for Health Statistics. 2010 National Health Interview Survey (NHIS) Public Use Data Release. NHIS Survey Description; 2011. Available online: ftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/NHIS/2010/srvydesc.pdf (accessed on 13 February 2018).
- National Center for Health Statistics. National Health Interview Survey (NHIS) Public Use Data Release. NHIS Survey Description; 2015. Available online: ftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/NHIS/2015/srvydesc.pdf (accessed on 16 April 2018).
- Gallup. Gallup Daily Methodology 2015. Available online: http://www.gallup.com/poll/195539/gallup-healthways-index-methodology-report-indexes.aspx (accessed on 17 April 2018).
- Kahneman, D.; Deaton, A. High income improves evaluation of life but not emotional well-being. Proc. Natl. Acad. Sci. USA 2010, 107, 16489–16493. [Google Scholar] [CrossRef] [Green Version]
- Deaton, A.; Stone, A.A. Evaluative and hedonic well-being among those with and without children at home. Proc. Natl. Acad. Sci. USA 2014, 111, 1328–1333. [Google Scholar] [CrossRef]
- Fujishiro, K.; Heaney, C.A. Doing what I do best: The association betweem skill utilization and employee health with healthy behavior as a mediator. Soc. Sci. Med. 2017, 175, 235–243. [Google Scholar] [CrossRef]
- Rentfrow, P.; Mellander, C.; Florida, R. Happy states of America: A state-level analysis of psychological, economic, and social well-being. J. Pers. Res. 2009, 43, 1073–1082. [Google Scholar] [CrossRef]
- Sommers, B.D.; Gunja, M.Z.; Finegold, K.; Musco, T. Changes in self-reported insurance coverage, access to care, and health under the Affordable Care Act. JAMA 2015, 314, 366–374. [Google Scholar] [CrossRef]
- Maric-Bilkan, C.; Arnold, A.P.; Taylor, D.A.; Dwinell, M.; Howlett, S.E.; Wenger, N.; Reckelhoff, J.F.; Sandberg, K.; Churchill, G.; Levin, E.; et al. Report of the National Heart, Lung, and Blood Institute Working Group on Sex Differences Research in Cardiovascular Disease: Scientific Questions and Challenges. Hypertension 2016, 67, 802–807. [Google Scholar] [CrossRef]
- Wasserstein, R.; Lazar, N. The ASA’s statement on p-values: Context, process, and purpose. Am. Stat. 2016, 70, 129–133. [Google Scholar] [CrossRef]
- Gilbert, K.L.; Quinn, S.C.; Goodman, R.M.; Butler, J.; Wallace, J. A meta-analysis of social capital and health: A case for needed research. J. Health Psychol. 2013, 18, 1385–1399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giordano, G.N.; Lindström, M. The impact of changes in different aspects of social capital and material conditions on self-rated health over time: A longitudinal cohort study. Soc. Sci. Med. 2010, 70, 700–710. [Google Scholar] [CrossRef]
- Barnay, T. Health, work and working conditions: A review of the European economic literature. Eur. J. Health Econ. 2016, 17, 693–709. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, S.T.; Fransson, E.I.; Heikkila, K.; Alfredsson, L.; Casini, A.; Clays, E.; De Bacquer, D.; Dragano, N.; Erbel, R.; Ferrie, J.E.; et al. Job strain and cardiovascular disease risk factors: Meta-analysis of individual-participant data from 47,000 men and women. PLoS ONE 2013, 8, e67323. [Google Scholar] [CrossRef]
- Chandola, T.; Britton, A.; Brunner, E.; Hemingway, H.; Malik, M.; Kumari, M.; Badrick, E.; Kivimaki, M.; Marmot, M. Work stress and coronary heart disease: What are the mechanisms? Eur. Heart J. 2008, 29, 640–648. [Google Scholar] [CrossRef] [PubMed]
- Janczura, M.; Bochenek, G.; Nowobilski, R.; Dropinski, J.; Kotula-Horowitz, K.; Laskowicz, B.; Stanisz, A.; Lelakowski, J.; Domagala, T. The relationship of metabolic syndrome with stress, coronary heart disease and pulmonary function—An occupational cohort-based study. PLoS ONE 2015, 10, e0133750. [Google Scholar] [CrossRef]
- Hammer, L.B.; Sauter, S. Total worker health and work-life stress. J. Occup. Environ. Med. 2013, 55, S25–S29. [Google Scholar] [CrossRef] [PubMed]
- Väänänen, A.; Kouvonen, A.; Kivimäki, M.; Pentti, J.; Vahtera, J. Social support, network heterogeneity, and smoking behavior in women: The 10-town study. Am. J. Health Promot. 2008, 22, 246–255. [Google Scholar] [CrossRef]
- Jaaskelainen, A.; Kaila-Kangas, L.; Leino-Arjas, P.; Lindbohm, M.L.; Nevanpera, N.; Remes, J.; Järvelin, M.R.; Laitinen, J. Psychosocial factors at work and obesity among young finnish adults: A cohort study. J. Occup. Environ. Med. 2015, 57, 485–492. [Google Scholar] [CrossRef]
- Cundiff, D.K. Diet and tobacco use: Analysis of data from the diabetic control and complications trial, a randomized study. Medscape J. Gen. Med. 2002, 4, 2. [Google Scholar]
- Nomura, K.; Nakao, M.; Tsurugano, S.; Takeuchi, T.; Inoue, M.; Shinozaki, Y.; Yano, E. Job stress and healthy behavior among male Japanese office workers. Am. J. Ind. Med. 2010, 53, 1128–1134. [Google Scholar] [CrossRef] [PubMed]
- Westermann, O.; Ashby, J.; Petty, J. Gender and social capital: The importance of gender differences for the maturity and effectivenss of natural resource management groups. World Dev. 2005, 33, 1783–1799. [Google Scholar] [CrossRef]
- Fonarow, G.C.; Calitz, C.; Arena, R.; Baase, C.; Isaac, F.W.; Lloyd-Jones, D.; Peterson, E.D.; Pronk, N.; Sanchez, E.; Terry, P.E.; et al. Workplace wellness recognition for optimizing workplace health: A presidential advisory from the American Heart Association. Circulation 2015, 131, e480–e497. [Google Scholar] [CrossRef] [PubMed]
- Skopec, L.; Musco, T.; Sommers, B.D. A potential new data source for assessing the impacts of health reform: Evaluating the Gallup-Healthways Well-Being Index. Healthcare 2014, 2, 113–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crowne, D.P.; Marlowe, D. A new scale of social desirability independent of psychopathology. J. Consult. Psychol. 1960, 24, 349–354. [Google Scholar] [CrossRef]
- Olynk Widmar, N.J.; Byrd, E.S.; Dominick, S.R.; Wolf, C.A.; Acharya, L. Social desirability bias in reporting of holiday season healthfulness. Prev. Med. Rep. 2016, 4, 270–276. [Google Scholar] [CrossRef] [Green Version]
- Prather, A.A.; Gottlieb, L.M.; Giuse, N.B.; Koonce, T.Y.; Kusnoor, S.V.; Stead, W.W.; Adler, N.E. National Academy of Medicine social and behavioral measures: Associations with self-reported health. Am. J. Prev. Med. 2017, 53, 449–456. [Google Scholar] [CrossRef]
- Hauser, C.; Perkmann, U.; Puntscher, S.; Walde, J.; Tappeiner, G. Trust works! Sources and effects of social capital in the workplace. Soc. Indic. Res. 2016, 128, 589–608. [Google Scholar] [CrossRef]
- Hämmig, O. Health and well-being at work: The key role of supervisor support. SSM Popul. Health 2017, 3, 393–402. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | Total Women | Mistrustful Environment | Total Men | Mistrustful Environment | ||
|---|---|---|---|---|---|---|
| % | % | SE | % | % | SE | |
| Total | 22.1 | 0.1 | 20.3 | 0.1 | ||
| Age | ||||||
| 18–29 * | 19.8 | 17.4 | 0.3 | 21.8 | 15.7 | 0.2 |
| 30–44 * | 32.4 | 22.3 | 0.2 | 35.1 | 20.5 | 0.2 |
| 45–64 * | 45.0 | 24.4 | 0.2 | 40.3 | 23.0 | 0.2 |
| 65+ | 2.8 | 17.2 | 0.5 | 2.9 | 15.9 | 0.5 |
| Race/ethnicity | ||||||
| White * | 72.0 | 22.4 | 0.1 | 72.2 | 21.1 | 0.1 |
| Black * | 12.9 | 23.2 | 0.4 | 8.8 | 20.6 | 0.4 |
| Asian | 2.4 | 17.7 | 0.8 | 2.7 | 17.1 | 0.6 |
| Hispanic * | 9.9 | 18.7 | 0.4 | 12.8 | 16.3 | 0.3 |
| Other | 2.8 | 21.9 | 0.8 | 3.4 | 19.5 | 0.6 |
| Education | ||||||
| <High school * | 4.4 | 19.3 | 0.7 | 7.1 | 17.3 | 0.5 |
| High school graduate | 21.9 | 20.0 | 0.3 | 26.0 | 19.8 | 0.2 |
| Technical/some college or associate degree * | 53.5 | 22.0 | 0.2 | 53.4 | 20.9 | 0.1 |
| 4-year college/post graduate * | 20.3 | 25.2 | 0.3 | 16.6 | 20.4 | 0.2 |
| Marital status | ||||||
| Single/ Never married * | 22.7 | 20.8 | 0.3 | 23.1 | 18.0 | 0.2 |
| Married * | 54.2 | 21.4 | 0.2 | 61.8 | 20.7 | 0.1 |
| Separated | 2.6 | 23.3 | 0.8 | 1.9 | 21.9 | 0.9 |
| Divorced | 12.1 | 26.8 | 0.4 | 7.0 | 24.7 | 0.4 |
| Widowed * | 2.9 | 22.8 | 0.7 | 0.8 | 20.8 | 1.1 |
| Domestic partner * | 5.5 | 23.2 | 0.6 | 5.5 | 20.1 | 0.5 |
| Family Income per month | ||||||
| <$1000 * | 3.3 | 21.0 | 0.8 | 2.8 | 18.6 | 0.8 |
| $1000–$,2999 * | 27.0 | 22.5 | 0.3 | 22.9 | 20.1 | 0.3 |
| $3000–$4999 * | 26.6 | 23.0 | 0.3 | 23.8 | 21.2 | 0.2 |
| $5000–$7499 * | 21.4 | 22.5 | 0.3 | 21.5 | 21.7 | 0.2 |
| ≥$7500 * | 21.9 | 21.9 | 0.3 | 29.1 | 19.6 | 0.2 |
| Mistrustful Environment | High Blood Pressure * | High Cholesterol * | Diabetes | Current Smoker * | ||||||||||||
| Women | Men | Women | Men | Women | Men | Women | Men | |||||||||
| % | SE | % | SE | % | SE | % | SE | % | SE | % | SE | % | SE | % | SE | |
| Yes | 21.9 | 0.3 | 25.7 | 0.3 | 19.7 | 0.2 | 24.6 | 0.2 | 6.9 | 0.2 | 7.0 | 0.1 | 18.7 | 0.3 | 23.5 | 0.3 |
| No | 18.7 | 0.1 | 21.2 | 0.1 | 16.6 | 0.1 | 20.2 | 0.1 | 5.9 | 0.1 | 5.8 | 0.1 | 17.2 | 0.1 | 21.6 | 0.1 |
| Mistrustful Environment | Poor Diet * | Insufficient Exercise * | BMI ≥ 30 * | |||||||||||||
| Women | Men | Women | Men | Women | Men | |||||||||||
| % | SE | % | SE | % | SE | % | SE | % | SE | % | SE | |||||
| Yes | 69.3 | 0.3 | 76.6 | 0.2 | 77.7 | 0.3 | 73.2 | 0.3 | 26.2 | 0.3 | 31.0 | 0.3 | ||||
| No | 67.6 | 0.2 | 75.1 | 0.1 | 76.1 | 0.1 | 71.4 | 0.1 | 22.8 | 0.2 | 26.9 | 0.1 | ||||
| CVD Risk Factors (Dependent variables) | Models | |
|---|---|---|
| Mistrustful Environment | ||
| OR (95% CI) | ||
| Women | Men | |
| High blood pressure | 1.15 (1.11, 1.20) | 1.20 (1.16, 1.24) |
| High cholesterol | 1.18 (1.13, 1.22) | 1.22 (1.18,1.26) |
| Diabetes | 1.15 (1.09, 1.23) | 1.18 (1.12, 1.25) |
| Current smoker | 1.15 (1.10, 1.20) | 1.15 (1.11, 1.19) |
| Poor diet | 1.10 (1.07, 1.14) | 1.11 (1.07, 1.15) |
| Insufficient physical activity | 1.10 (1.06, 1.14) | 1.08 (1.05, 1.11) |
| Obese | 1.18 (1.14, 1.23) | 1.18 (1.15, 1.22) |
| Four or more risk factors | 1.22 (1.16, 1.27) | 1.29 (1.25, 1.34) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alterman, T.; Tsai, R.; Ju, J.; Kelly, K.M. Trust in the Work Environment and Cardiovascular Disease Risk: Findings from the Gallup-Sharecare Well-Being Index. Int. J. Environ. Res. Public Health 2019, 16, 230. https://doi.org/10.3390/ijerph16020230
Alterman T, Tsai R, Ju J, Kelly KM. Trust in the Work Environment and Cardiovascular Disease Risk: Findings from the Gallup-Sharecare Well-Being Index. International Journal of Environmental Research and Public Health. 2019; 16(2):230. https://doi.org/10.3390/ijerph16020230
Chicago/Turabian StyleAlterman, Toni, Rebecca Tsai, Jun Ju, and Kevin M. Kelly. 2019. "Trust in the Work Environment and Cardiovascular Disease Risk: Findings from the Gallup-Sharecare Well-Being Index" International Journal of Environmental Research and Public Health 16, no. 2: 230. https://doi.org/10.3390/ijerph16020230