Profile and Motivation of Patients Consulting in Emergency Departments While not Requiring Such a Level of Care

 ,
,
Abstract
:1. Introduction
Definition of a Consultation not Requiring a Medical Emergency Department Level of Care
2. Methods
2.1. Study Design
2.2. Objectives
- Establish whether CIMU 5 patients could be reoriented by the TN towards their PCP without an ED physician consultation;
- Assess post-ED consultation satisfaction.
2.3. Population
- Age > 18 years;
- Beneficiary of social security;
- French or English speaking and writing;
- French resident;
- Spontaneously coming to consult at the emergency department; in other words, not having been sent to the ED by the 112 emergency hotline, another physician, or brought to the ED by any first responder (police, fire department, military);
- Categorized as CIMU 5.
- Having been asked back by the ED (systematic follow-up, clinical deterioration);
- Unable to write (for example, due to trauma);
- Vulnerable or marginalized members of the population (homeless, refugees, migrants, undocumented migrants, etc.);
- Presenting with a nonmedical issue;
- Having refused to participate in the study;
- Having answered the survey but having left without having been seen by the ED physician;
- Not categorized as CIMU 5 (in case of survey given to the wrong patient);
- Other cases (inaccurate history).
2.4. Questionnaire
2.5. Data Collection
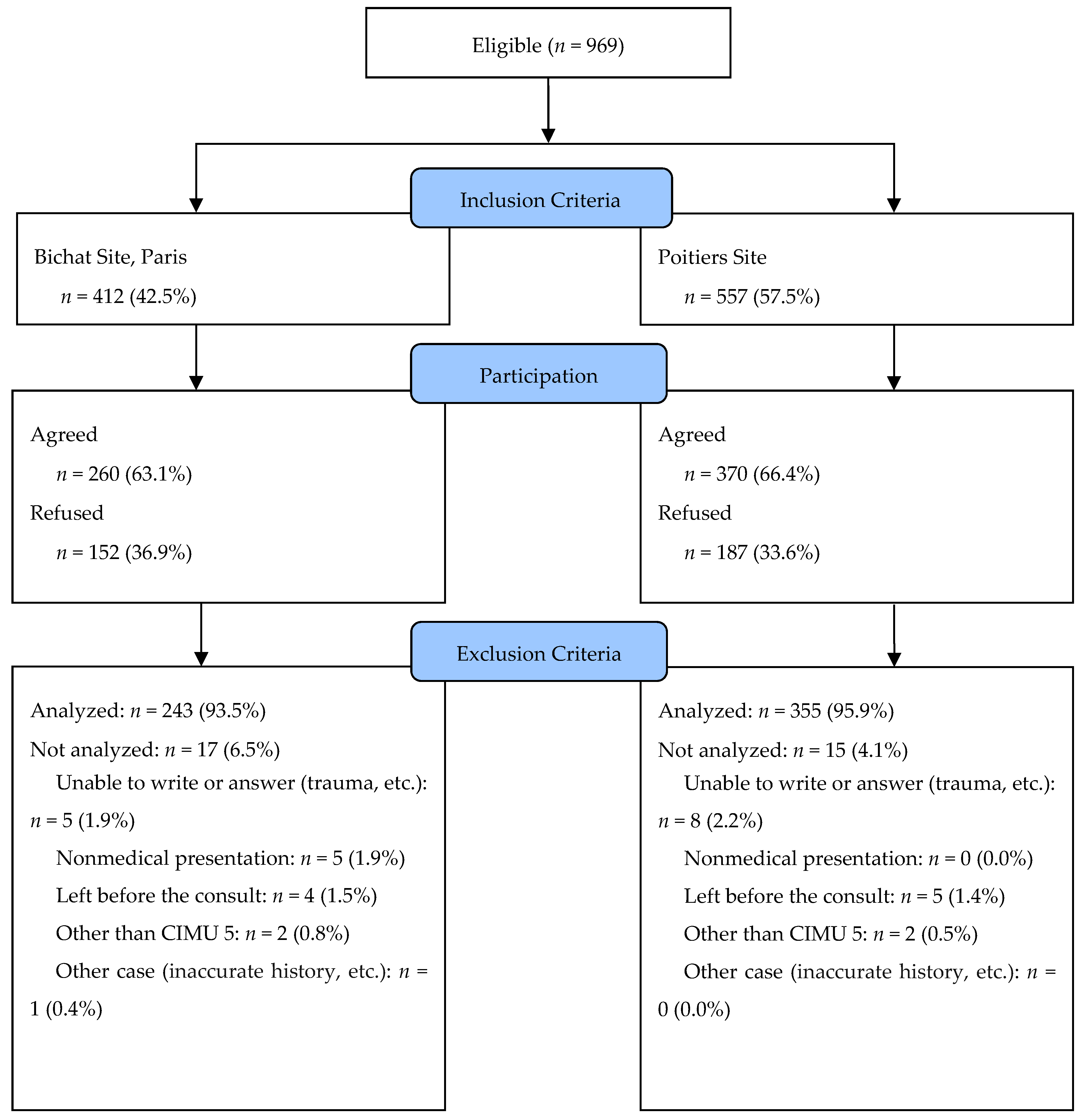
2.6. Flow Chart
2.7. Outcomes and Study Variables
2.8. Statistics
2.9. Ethics
3. Results
3.1. CIMU 5 Patient Characteristics
3.2. Patient Flow Paths
3.3. Complaints Justifying the Consultations
3.4. Care provided at the ED
4. Discussion
4.1. Profile and Flow Path of Patients Manageable by General Practice Consultations
4.2. What Solutions Could Be Feasible to Optimally Offer Care for These Patients?
4.3. Limits
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Consent to Publish
Availability of Data and Material
Abbreviations
| CCMU | French clinical emergency department classification (Classification Clinique des Malades aux Urgences) |
| CIMU | French Emergency Nurses Classification in Hospital scale, CIMU (Classification Infirmière des Malades aux Urgences) |
| ED | emergency department |
| ENT | ear, nose, and throat |
| PCP | primary care provider |
| SFMU | French Emergency Medicine Society |
| TN | triage nurse |
Appendix A. The French Emergency Nurses Classification in Hospital scale, Classification Infirmière des Malades aux Urgences (CIMU)

{kind=link}
| Triage | Description | Action |
| 1 | Immediately life-threatening. | Actions focused on support of one or more vital functions. Immediate medical and paramedical intervention. |
| 2 | Marked impairment of a vital organ or imminently life-threatening or functionally disabling traumatic lesion. | Actions focused on treatment of the vital function or traumatic lesion. Immediate paramedical and medical intervention within 20 min. |
| 3 | Functional impairment or organic lesions likely to deteriorate within 24 h or complex medical situation justifying the use of several hospital resources. | Multiple actions focused on diagnostic evaluation and prognostic evaluation in addition to treatment. Medical intervention within 60 min ± followed by paramedical intervention. |
| 4 | Stable, noncomplex functional impairment or organic lesions, but justifying the urgent use of at least one hospital resource. | Consult with limited diagnostic or therapeutic procedures. Medical intervention within 120 min ± followed by paramedical intervention. |
| 5 | No functional impairment or organic lesion justifying the use of hospital resources. | Consult with no diagnostic or therapeutic procedure. Medical intervention within 240 min. |
| * | Intense symptom or abnormal vital parameter justifying rapid corrective action. | Specific action within 20 min. The star can complete a triage 3 or 4. |
Appendix B. Survey Distributed to the Included CIMU 5 Patients
| Family name: _____________________________________ |  | |
| First name: _____________________________________ | ||
| Sex: ▯ Female ▯ Male | ||
| Birthday: | ___ / ___ / ______ | |
| Phone: | __ __ __ __ __ | |
| City/Town of residence: | ____________________________ | |
- ▯
- Social security insurance
- ▯
- Complementary health coverage
- ▯
- Special social security (CMU, AME)
- ▯
- None
- ▯
- Yes, in which city is your GP? ________________________
- ▯
- No
- ▯
- Farmer, agricultural worker
- ▯
- Craftsman, merchant, manager
- ▯
- Executive, intellectual profession
- ▯
- Intermediate professions
- ▯
- Employee
- ▯
- Unskilled laborer
- ▯
- Retired
- ▯
- No professional activity
- ▯
- Student
- ▯
- Yes
- ▯
- No, where did you consult? _______ ________________________________
- ▯
- Proximity to home or work
- ▯
- Schedule compatibility with my activity
- ▯
- Attending GP unavailable
- ▯
- The appointment proposed by my doctor was not convenient for me
- ▯
- I have moved and I have not yet found a doctor
- ▯
- I don’t have a GP
- ▯
- I am on business travel, so I do not have access to my GP
- ▯
- After advice from my GP or another health professional (another doctor, physiotherapist, nurse, etc.)
- ▯
- I wanted another medical opinion, in addition to that of my GP
- ▯
- I would like to have direct advice from a specialist
- ▯
- I thought I would need additional tests (blood test, imagery, etc.)
- ▯
- I thought I would have to be hospitalized
- ▯
- I’m being followed in the hospital
- ▯
- I chose to consult at the emergency department because it is well known that it is the quickest
- ▯
- I cannot pay any upfront fees
- ▯
- Other:
Appendix C. French Clinical Emergency Department Classification, Classification Clinique des Malades aux Urgences (CCMU)
| Classification | Description |
| CCMU 1 | Stable situation, abstention from complementary diagnostic or therapeutic act |
| CCMU 2 | Stable situation, perform a complementary diagnostic or therapeutic act |
| CCMU 3 | Situation likely to deteriorate without being life-threatening |
| CCMU 4 | Prognosis committed, no immediate resuscitation maneuver |
| CCMU 5 | Prognosis committed, perform immediate resuscitation maneuver |
| CCMU P | Patient with psychological or psychiatric problems dominant in the absence of any unstable somatic pathology |
| CCMU D | Patient dies at the entrance to the emergency |
Appendix D. Informed Consent
- -
- Sociodemographic categories
- -
- Medical administrative information
- -
- Motivation to consult in the emergency department
- -
- Patient satisfaction
- -
- Dr Aiham Daniel GHAZALI, main investigator, Emergency Department of Bichat Hospital
- -
- Dr Arnaud CHAUDET, Emergency Department of Poitiers Hospital
References
- Durand, A.C.; Gentile, S.; Devictor, B.; Palazzolo, S.; Vignally, P.; Gerbeaux, P.; Sambuc, R. ED patients: How non-urgent are they? Systematic review of the emergency medicine literature. Am. J. Emerg. Med. 2011, 29, 333–345. [Google Scholar] [CrossRef] [PubMed]
- Résultats de l’enquête nationale auprès des structures des urgences hospitalières. 2013. Available online: http://drees.solidarites-sante.gouv.fr/etudes-et-statistiques/publications/les-dossiers-de-la-drees/dossiers-solidarite-et-sante/article/resultats-de-l-enquete-nationale-aupres-des-structures-des-urgences (accessed on 12 September 2019).
- Sarría-Santamera, A.; Hijas-Gómez, A.I.; Carmona, R.; Gimeno-Feliú, L.A. A systematic review of the use of health services by immigrants and native populations. Public Health Rev. 2016, 37, 28. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.; Klingberg, K.; Srivastava, D.; Exadaktylos, A.K. Consultations by Asylum Seekers: Recent Trends in the Emergency Department of a Swiss University Hospital. PLoS ONE 2016, 11, e0155423. [Google Scholar] [CrossRef] [PubMed]
- Ruud, S.E.; Aga, R.; Natvig, B.; Hjortdahl, P. Use of emergency care services by immigrants—A survey of walk-in patients who attended the Oslo Accident and Emergency Outpatient Clinic. BMC Emerg. Med. 2015, 15, 25. [Google Scholar] [CrossRef] [PubMed]
- Mladovsky, P. Migration and Health in the EU, Research Note for the European Commission, DG Employment and Social Affairs; Employment, Social Affairs and Equal Opportunities: London, UK, 2007. [Google Scholar]
- Berchet, C. Health care utilisation in France: An analysis of the main drivers of health care use inequalities related to migration. Rev. Epidemiol. Sante Publique 2013, 61, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Winters, M.; Rechel, B.; de Jong, L.; Pavlova, M. A systematic review on the use of healthcare services by undocumented migrants in Europe. BMC Health Serv. Res. 2018, 18, 30. [Google Scholar] [CrossRef] [PubMed]
- Crawford, J.; Cooper, S.; Cant, R.; DeSouza, R. The impact of walk-in centres and GP co-operatives on emergency department presentations: A systematic review of the literature. Int. Emerg. Nurs. 2017, 34, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Van den Heede, K.; Quentin, W.; Dubois, C.; Devriese, S.; Van de Voorde, C. The 2016 proposal for the reorganisation of urgent care provision in Belgium: A political struggle to co-locate primary care providers and emergency departments. Health Policy 2017, 121, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Bardelli, P.; Kaplan, V. Non-urgent encounters in a Swiss medical emergency unit. Swiss Med. Wkly. 2013, 143, w13760. [Google Scholar] [CrossRef] [PubMed]
- Baubeau, D.; Carrasco, V. Ministère de la Solidarité de la Santé et de la Protection Sociale. Direction de la Recherche des Etudes de l’Evaluation et des Statistiques. (D.R.E.E.S.). Paris. FRA. Motifs et trajectoires de recours aux urgences hospitalières. Etudes Result 2003, 215, 1–12. Available online: https://drees.solidarites-sante.gouv.fr/etudes-et-statistiques/publications/etudes-et-resultats/article/motifs-et-trajectoires-de-recours-aux-urgences-hospitalieres (accessed on 12 September 2019).
- Aissaoui, L. Consultations spontanées aux urgences du centre hospitalier de Givors étude monocentrique, observationnelle, du 1er au 28 mars 2011 des patients non hospitalisés durant les heures ouvrables des cabinets médicaux analyse des caractéristiques sociologiques des consultants, de leurs motifs de recours et évaluation de leur satisfaction de service. Lyon. 2014. Available online: https://books.google.fr/books/about/Consultations_spontan%C3%A9es_aux_urgences_d.html?id=gkvMoAEACAAJ&redir_esc=y (accessed on 12 September 2019).
- Miyazawa, A.; Maeno, T.; Shaku, F.; Tsutsumi, M.; Kurihara, H.; Takayashiki, A. Inappropriate use of the emergency department for non-urgent conditions: Patient characteristics and associated factors at a Japanese hospital. J. Gen. Fam. Med. 2019, 20, 146–153. [Google Scholar] [PubMed]
- Redstone, P.P. Non-urgent use of the emergency department. J. Ambul. Care Manag. 2008, 31, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Sempere-Selva, T.; Peiro, S.; Sendra-Pina, P.; Martinez-Espin, C.; Lopez-Aguilera, I. Inappropriate use of an accident and emergency department: Magnitude, associated factors, and reasons—An approach with explicit criteria. Ann. Emerg. Med. 2001, 37, 568–579. [Google Scholar] [CrossRef] [PubMed]
- Mesnier, T. Assurer le premier accès aux soins—Organiser les soins non programmés dans les territoires. 2018. Available online: https://solidaritessante.gouv.fr/IMG/pdf/rapport_snp_vf.pdf (accessed on 12 September 2019).
- Cohen, L.; Genisson, C.; Savary, R.P. Sénat. Paris. FRA. Rapport d’information sur les urgences hospitalières. 2017. Available online: https://www.senat.fr/rap/r16-685/r16-6851.pdf (accessed on 12 September 2019).
- Gentile, S.; Amadeï, E.; Bouvenot, J.; Durand, A.C.; Bongiovanni, I.; Haro, J.; Giraud, C.; Sambuc, R. Attitudes et comportement des usagers face à une urgence réelle ou ressentie. St. Publique 2004, 16, 63. [Google Scholar] [CrossRef] [PubMed]
- Toulemonde, C. Évaluation de l’offre de soins primaires des médecins et des urgences médicales de Paris et évolution prévue à 2 et 5 ans dans le cadre de l’étude Demomed75. Thèse d’exercice de médecine générale. Paris 6 Pierre et Marie Curie. 2015. Available online: https://pdfs.semanticscholar.org/1be4/2be0e6e651c3ff7fabfc6317db9ec8dc0acb.pdf. (accessed on 12 September 2019).
- Atenstaedt, R.; Gregory, J.; Price-Jones, C.; Newman, J.; Roberts, L.; Turner, J. Why do patients with non-urgent conditions present to the Emergency Department despite the availability of alternative services? Eur. J. Emerg. Med. 2015, 22, 370–373. [Google Scholar] [CrossRef] [PubMed]
- Sagnes-Raffy, C. Observatoire Régional des Urgences Midi-Pyrénées (O.R.U.M.I.P.). Étude des déterminants conduisant les patients qui ne relèvent pas de l’urgence médico-vitale à se présenter dans un service d’urgence public ou privé plutôt que de faire appel à la médecine de ville. RECTO VERSO. Toulouse. 2004. Available online: https://www.orumip.fr/wp-content/uploads/2011/11/RV6.pdf (accessed on 12 September 2019).
- Pigozzo, C. Étude prospective et analyse du profil et motivations des patients consultant aux urgences pour des motifs relevant de la médecine générale. Thèse d’exercice de médecine générale. Montpellier. 2014. Available online: https://bdsp-ehesp.inist.fr/vibad/index.php?action=getRecordDetail&idt=483061 (accessed on 12 September 2019).
- Le Roux, S. Les patients CCMU1 consultent-ils au service des urgences du CHU de Nîmes suite à des difficultés d’accès aux soins primaires? Thèse d’exercice de médecine générale. Montpellier. 2013. Available online: https://books.google.fr/books/about/Les_patients_CCMU1_consultent_ils_au_ser.html?id=5IrLuQEACAAJ&redir_esc=y (accessed on 12 September 2019).
- Beauné, n. Quels sont les déterminants de consultations spontanées au service des urgences des patients adultes ayant dejà consulté un médecin généraliste pour le même motif? étude quantitative menée au service des urgences du centre hospitalier Alpes Léman. Thèse d’exercice de médecine générale. Lyon. 2016. Available online: https://www.worldcat.org/title/quels-sont-les-determinants-de-consultations-spontanees-au-service-des-urgences-des-patients-adultes-ayant-deja-consulte-un-medecin-generaliste-pour-le-meme-motif-etude-quantitative-menee-au-service-des-urgences-du-centre-hospitalier-alpes-leman/oclc/951383097 (accessed on 12 September 2019).
- Gentile, S.; Vignally, P.; Durand, A.C.; Gainotti, S.; Sambuc, R.; Gerbeaux, P. Non-urgent patients in the emergency department? A French formula to prevent misuse. BMC Health Serv. Res. 2010, 10, 66. [Google Scholar] [CrossRef] [PubMed]
- Saryoul, S. Influence de la précarité sur le choix des urgences ou du médecin généraliste pour une consultation de soins primaires. Thèse d’exercice de médecine générale. Dijon. 2016. Available online: file:///D:/Users/g-bjn-5054263/Downloads/SARYOUL_THESEMED.pdf (accessed on 12 September 2019).
- Shaw, E.K.; Howard, J.; Clark, E.C.; Etz, R.S.; Arya, R.; Tallia, A.F. Decision-making processes of patients who use the emergency department for primary care needs. J. Health Care Poor Underserved 2013, 24, 1288–1305. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Nejtek, V.A.; Zieger, D.; Robinson, R.D.; Schrader, C.D.; Phariss, C. The role of charity care and primary care physician assignment on ED use in homeless patients. Am. J. Emerg. Med. 2015, 33, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Taboulet, P.; Moreira, V.; Haas, L.; Porcher, R.; Braganca, A.; Fontaine, J.P.; Poncet, M.C. Triage with the French Emergency Nurses Classification in Hospital scale: Reliability and validity. Eur. J. Emerg. Med. 2009, 16, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Fays Duet, M. Enquête DémoMed 75: Évaluation de l’offre de soins primaires à Paris et évolution prévisible dans 2 et 5 ans. Résultats sur le 18ème arrondissement. Thèse d’exercice de médecine générale. Paris 7 Denis Diderot. 2014. Available online: http://www.bichat-larib.com/publications.documents/4698_FAYS-THESE.pdf?bcsi_scan_08276ca4327756e4=1 (accessed on 12 September 2019).
- Données statistiques sur la démographie des professionnels de santé (PS) libéraux. L’Assurance Maladie. 2017. Available online: https://www.ameli.fr/l-assurance-maladie/statistiques-et-publications/donnees-statistiques/professionnels-de-sante-liberaux/demographie/effectifs-et-densite.php (accessed on 12 September 2019).
- Sanz, M.; Noguerol, B.; Sanz-Sanchez, I.; Hammerle, C.H.; Schliephake, H.; Renouard, F.; Steering Committee. European Association for Osseointegration Delphi study on the trends in Implant Dentistry in Europe for the year 2030. Clin. Oral Implant. Res. 2019, 30, 476–486. [Google Scholar] [CrossRef] [PubMed]
- Afilal, M.; Yalaoui, F.; Dugardin, F.; Amodeo, L.; Laplanche, D.; Blua, P. Emergency department flow: A new practical patients classification and forecasting daily attendance. IFAC PapersOnLine 2016, 49, 721–726. [Google Scholar] [CrossRef]
- Nosjean, C. Quels sont les déterminants de l’accès aux soins primaires en pré-hospitalier des consultations de médecine générale aux urgences de Fontenay Le Comte? étude descriptive, prospective, monocentrique, réalisée entre février 2016 et septembre 2016. Thèse d’exercice de médecine générale. Nantes. 2017. Available online: file:///D:/Users/g-bjn-5054263/Downloads/nosjeanMED17.pdf (accessed on 12 September 2019).
- Cour des Comptes. Paris. FRA. Les urgences hospitalières: Une fréquentation croissante, une articulation avec la médecine de ville à repenser. In Rapport sur l’application des lois de financement de la sécurité sociale; Cour des Comptes: Paris, France, 2014; pp. 359–387. Available online: https://www.ccomptes.fr/sites/default/files/EzPublish/rapport_securite_sociale_2014_urgences_hospitalieres.pdf (accessed on 12 September 2019).
- Xin, H. Patient Dissatisfaction with Primary Care and Non-urgent Emergency Department Use. J. Ambul. Care Manag. 2019, 42, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Greenfield, G.; Ignatowicz, A.; Gnani, S.; Bucktowonsing, M.; Ladbrooke, T.; Millington, H. Staff perceptions on patient motives for attending GP-led urgent care centres in London: A qualitative study. BMJ Open 2016, 6, e007683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chmiel, C.; Wang, M.; Sidler, P.; Eichler, K.; Rosemann, T.; Senn, O. Implementation of a hospital-integrated general practice—A successful way to reduce the burden of inappropriate emergency-department use. Swiss Med. Wkly. 2016, 146, w14284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleary, A.; Zeller, R.; Maguire, C.; Goh, S.; Shortt, N. Do all adult orthopaedic injuries seen in emergency departments need to attend fracture clinic? A Queensland multicentred review. Emerg. Med. Australas. EMA 2017, 29, 658–663. [Google Scholar] [CrossRef] [PubMed]
- Norredam, M.; Nielsen, S.S.; Krasnik, A. Migrants’ utilization of somatic healthcare services in Europe—A systematic review. Eur. J. Public Health 2010, 20, 555–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norredam, M.; Mygind, A.; Nielsen, A.S.; Bagger, J.; Krasnik, A. Motivation and relevance of emergency room visits among immigrants and patients of Danish origin. Eur. J. Public Health 2007, 17, 497–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hargreaves, S.; Friedland, J.S.; Gothard, P.; Saxena, S.; Millington, H.; Eliahoo, J. Impact on and use of health services by international migrants: Questionnaire survey of inner city London A&E attenders. BMC Health Serv. Res. 2006, 6, 153. [Google Scholar]

| Characteristics of Patients | Total n = 598 | Bichat n = 243 | Poitiers n = 355 | p |
|---|---|---|---|---|
| Male patients, no. (%) | 475 (79.4) | 179 (73.7) | 296 (83.4) | 0.003 |
| Age (year), median (IQR *) | 38 (27–50) | 37 (27–50) | 38 (26–49) | 0.74 |
| Nearby place of residence **, no. (%) | 314 (52.5) | 140 (57.6) | 174 (49.0) | 0.04 |
| Basic Social Security coverage, no. (%) | 511 (85.5) | 200 (82.3) | 311 (87.6) | 0.07 |
| Complementary health coverage, no. (%) | 395 (66.1) | 142 (58.4) | 253 (81.4) | 0.04 |
| Designated primary care provider, no. (%) | 521 (87.1) | 189 (77.8) | 332 (93.5) | <0.0001 |
| Nearby primary care provider, no. (%) | 423 (70.7) | 215 (88.5) | 208 (58.6) | <0.0001 |
| Professional category/occupation, no. (%) | 0.27 | |||
| Farmers | 5 (0.8) | 1 (0.4) | 4 (1.1) | |
| Managers | 50 (8.4) | 29 (11.9) | 21 (5.9) | |
| Craftsman/woman | 33 (5.5) | 10 (4.1) | 23 (6.5) | |
| Laborers | 48 (8.0) | 21 (8.6) | 27 (7.6) | |
| Middle management | 41 (6.9) | 7 (2.9) | 34 (9.6) | |
| Employees | 66 (11.0) | 22 (9.1) | 44 (12.4) | |
| Inactive | 89 (14.9) | 39 (16.1) | 50 (14.1) | |
| Students | 203 (33.9) | 86 (35.4) | 117 (32.9) | |
| Retired | 63 (10.6) | 28 (11.5) | 35 (9.9) |
| Total of CIMU 5 * Patients | University Hospital of Bichat | University Hospital of Poitiers | |||||||
|---|---|---|---|---|---|---|---|---|---|
| PCP ** | No PCP | p | PCP | No PCP | p | PCP | No PCP | p | |
| 08:00–20:00 | 433 | 66 | 0.57 | 161 | 48 | 0.48 | 272 | 18 | 0.66 |
| 20:00–08:00 | 88 | 11 | 28 | 6 | 60 | 5 | |||
| Weekdays | 363 | 56 | 0.58 | 145 | 40 | 0.69 | 218 | 16 | 0.15 |
| Weekends/Holidays | 158 | 21 | 44 | 14 | 114 | 7 | |||
| Consultation Reasons | Total n = 598 | Bichat n = 243 | Poitiers n = 355 | p |
|---|---|---|---|---|
| Cardio-vascular, no. (%) | 26 (4.3) | 13 (5.3) | 13 (3.7) | 0.32 |
| Dermatological, no. (%) | 74 (12.4) | 23 (9.5) | 51 (14.4) | 0.07 |
| Gastroenterological, no. (%) | 43 (7.2) | 30 (12.4) | 13 (3.7) | <0.0001 |
| General and other, no. (%) | 58 (9.7) | 30 (12.4) | 28 (7.9) | 0.07 |
| Urogenital, no. (%) | 24 (4.0) | 13 (5.3) | 11 (3.1) | 0.17 |
| Neurological, no. (%) | 28 (4.7) | 10 (4.1) | 18 (5.1) | 0.59 |
| Ophthalmological, no. (%) | 57 (9.5) | 4 (1.6) | 53 (14.9) | <0.0001 |
| ENT, no. (%) | 67 (11.2) | 18 (7.4) | 49 (13.8) | 0.02 |
| Psychiatry, no. (%) | 7 (1.2) | 4 (1.6) | 3 (0.8) | 0.45 |
| Respiratory, no. (%) | 9 (1.5) | 5 (2.1) | 4 (1.1) | 1 |
| Rheumatology, no. (%) | 109 (18.2) | 49 (20.2) | 60 (16.9) | 0.31 |
| Traumatology, no. (%) | 96 (16.1) | 44 (18.1) | 52 (14.6) | 0.26 |
| Motivation | Total n = 598 | Bichat n = 243 | Poitiers n = 355 | p |
|---|---|---|---|---|
| Workplace accident, no. (%) | 17 (2.8) | 6 (2.5) | 11 (3.1) | 0.65 |
| Suggested by peers, no. (%) | 3 (0.5) | 1 (0.4) | 2 (0.6) | 1.0 |
| Suggested by a professional *, no. (%) | 58 (9.7) | 17 (7.0) | 41 (11.6) | 0.06 |
| Second opinion, no. (%) | 21 (3.6) | 7 (2.9) | 14 (3.9) | 0.49 |
| Intense pain, no. (%) | 27 (4.5) | 9 (3.7) | 18 (5.1) | 0.43 |
| Additional testing, no. (%) | 157 (26.3) | 59 (24.3) | 98 (27.6) | 0.36 |
| Appointmenthours, no. (%) | 8 (1.3) | 4 (1.6) | 4 (1.1) | 0.59 |
| After business hours **, no. (%) | 31 (5.2) | 8 (3.3) | 23 (6.5) | 0.11 |
| Hospitalization, no. (%) | 14 (2.3) | 6 (2.5) | 8 (2.3) | 0.86 |
| Unavailable PCP ***, no. (%) | 115 (19.2) | 42 (17.3) | 73 (20.6) | 0.32 |
| Lack of upfront payment, no. (%) | 22 (3.7) | 13 (5.3) | 9 (2.5) | 0.07 |
| Geographic proximity ****, no. (%) | 106 (17.7) | 63 (26.0) | 43 (12.1) | <0.0001 |
| Already taken care of in this hospital, no. (%) | 19 (3.2) | 8 (3.2) | 11 (3.0) | 0.89 |
| Clinical Severity | Total n = 593 | Bichat n = 242 | Poitiers n = 351 | p |
|---|---|---|---|---|
| CCMU 1, no. (%) | 399 (67.3) | 167 (69.1) | 232 (66.1) | 0.81 |
| CCMU 2, no. (%) | 178 (30.0) | 68 (28.1) | 110 (31.3) | |
| CCMU 3, no. (%) | 10 (1.7) | 4 (1.7) | 6 (1.7) | |
| CCMU 4, no. (%) | 3 (0.5) | 1 (0.4) | 2 (0.6) | |
| CCMU 5, no. (%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| CCMU P, no. (%) | 3 (0.5) | 2 (0.8) | 1 (0.3) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghazali, D.A.; Richard, A.; Chaudet, A.; Choquet, C.; Guericolas, M.; Casalino, E. Profile and Motivation of Patients Consulting in Emergency Departments While not Requiring Such a Level of Care. Int. J. Environ. Res. Public Health 2019, 16, 4431. https://doi.org/10.3390/ijerph16224431
Ghazali DA, Richard A, Chaudet A, Choquet C, Guericolas M, Casalino E. Profile and Motivation of Patients Consulting in Emergency Departments While not Requiring Such a Level of Care. International Journal of Environmental Research and Public Health. 2019; 16(22):4431. https://doi.org/10.3390/ijerph16224431
Chicago/Turabian StyleGhazali, Daniel Aiham, Arnaud Richard, Arnaud Chaudet, Christophe Choquet, Maximilien Guericolas, and Enrique Casalino. 2019. "Profile and Motivation of Patients Consulting in Emergency Departments While not Requiring Such a Level of Care" International Journal of Environmental Research and Public Health 16, no. 22: 4431. https://doi.org/10.3390/ijerph16224431