Abstract
Background. The world population is aging. This phenomenon is accompanied by an increase in the number of elderly with dementia, whose oral hygiene care is a challenge. Objective. This paper presents a literature review of oral health status and the need for oral care in people with dementia, as compared to people without dementia and also of the relationship between periodontal disease and cognitive impairment. Methods. A systematic review was conducted in PubMed, CINAHL, and the Cochrane Library. Fifty-six articles met the inclusion criteria and were consequently included for quality assessment and data extraction. Results. No significant differences were found between both groups with regard to the number of present teeth, DMFT Index, edentulousness/use of denture, and orofacial pain. Coronal/root caries and retained roots were more common in people with dementia than in those without dementia. Most of the participants with dementia presented gingival bleeding or inflammation and they suffered from the periodontal disease more than people without dementia. Conclusions. Poor oral health is a common condition among the elderly with dementia. The education process of caregivers might improve the oral health status of people with dementia. Finally, periodontal disease might contribute to the onset or progression of dementia.
1. Introduction
The transition from high to low mortality and fertility that accompanied the socioeconomic development of this century has meant a shift in the leading causes of disease and death and an increase of general health problems [1].
As a consequence, a decline of the oral health conditions of the elderly, such as dental caries and periodontal disease, is to be expected [2]. Poor oral health is more common in the elderly suffering from dementia, a disorder that will become prevalent with advancing age of the world population. Several studies analyzed the relationship between poor oral health and cognitive impairment, which suggests that cognitive decline might negatively impact oral health and also that poor oral health might lead to cognitive decline via specific biological mechanisms [3]. Conversely, in a recent systematic review by Wu et al. it has been argued that, according to some studies, it is unclear how or whether oral health conditions and cognitive status are related [4].
In cognitively impaired elderly, the increased incidence of oral disease might be favored by their general conditions: cognitive decline, loss of memory, learning disabilities, attention deficits, and motor skills deterioration, which result in reduced ability to perform routine oral care [5]. A frequent difficulty among these subjects is also the refusal of oral hygiene care, not opening their mouth, using abusive language, or being aggressive.
Even in the early stages of the disease progression, the elderly with dementia have a reduced salivary flow, which can lead not only to a higher prevalence of dental caries [6], but also to difficulties with eating and swallowing, which compromises communication skills [7]. The study by Silva et al. demonstrated that people with dementia living in Australians nursing homes have higher levels of untreated coronal and root caries, due to their cognitive condition and to poor access to professional services [8].
Periodontal disease is higher in the elderly with dementia than in normal cognitive individuals and the periodontal status worsens with the cognitive impairment progression [9]. Evidence of the association between periodontal disease and dementia has been demonstrated: periodontal disease is an inflammatory illness that affects the mouth and it could systemically affect individuals who are vulnerable to dementia and contribute to its pathogenesis [10].
Oral mucosal lesions are frequent in the elderly: the most common denture-related lesions are stomatitis, angular cheilitis, ulcers, hyperplasia, or candidosis. Reduced cognitive independence and decline in self-care, due to dementia, delirium, and social isolation, and it could make oral mucosal condition even worse [11].
Oral health problems in non-verbal individuals could negatively impact life quality, since they cannot communicate their pain and discomfort. On this topic, the study by Merlijn W. de Vries et al. proved the reliability of “the Orofacial Pain Scale for Non-Verbal Individuals” (OPS-NVI) and its psychometric evaluation (Delwel et al. 2018), to establish the presence of pain-related nonverbal communication, such as facial expressions, body movements, and vocal expressions [12].
1.1. Rationale of the Systematic Review
The most important risk factor that is associated with the onset of dementia is age and in an aging society, the impact of the phenomenon will be of alarming dimensions. Dementia reduces the quality of life of patients also with regard to oral health. It has been demonstrated that oral health of the elderly with dementia is poorer than oral health in people with normal cognitive function [13,14]. However, it is currently unclear how or whether oral health and cognitive status are related [15,16]. This study is aimed at reviewing literature, in order to evaluate oral health status in elderly with dementia, while comparing the data with those of elderly without dementia and to establish and assess the need of specific oral care strategies, which could improve their quality of life. This research was also conducted to review the available data regarding the influence of periodontal disease on the progression of cognitive impairment.
1.2. Objectives
The purpose of this systematic review was to examine studies about oral health in elderly with and without dementia, focusing the research on coronal and roots caries, number of remained teeth and retained roots, Decayed Missing Filled Index, periodontal disease, utilization of dentures, salivary flow, oral hygiene, oral mucosal lesions, orofacial pain, and on the analysis of periodontal disease as a potential risk factor for dementia.
This study reviewed cohort, case-control, cross-sectional studies, and randomized controlled clinical trials in order to examine oral health comparing the elderly with and without dementia. Inclusion criteria of participants were a diagnosis of dementia and the availability of data related to their oral health.
1.3. Clinical Question (PICO):
- P: A population of participants with diagnosis of dementia aged 60 years or older
- I: Analysis of the oral health status and of the association between periodontal disease and dementia
- C: Comparison between oral health of elderly with and without dementia
- O: Prevalence of oral disease (affecting hard and soft tissues) in elderly with dementia compared to those without dementia, to define their need of oral care. Role of tooth loss due to periodontal disease in the onset/progression of dementia.
2. Material and Methods
2.1. Protocol and Registration
Methods and inclusion criteria were selected following the PRISMA statement [17], which offers a protocol with respect to the reference items that were included in this systematic review.
2.2. Eligibility Criteria
Inclusion and Exclusion Criteria
In this systematic review, all of the articles concerning oral health in the elderly with dementia meeting the following requirements were included:
- Participants must have been diagnosed with dementia
- Quantitative data about oral health problems
- Participants had to be available
- Participants had to be 60 years or older
- Cohort, case-control, cross-sectional studies, and clinical trial were considered
The exclusion criteria were as follows:
- Case report and reviews
- No quantitative data available
- Age of participants below 60 years
2.2.1. Search
An electronic research was conducted to identify relevant studies that have been published within 2019, but no restrictions were imposed with regard to language of the primary studies or methodology. The following electronic databases were used: PubMed, CINAHL, and Cochrane Library. The keywords used were the same for all three databases and they were combined with the Boolean term “AND”: “oral health”, “aging population”, “oral disease”, “association with periodontal disease” and “OR”: “oral care need”, and “oral care strategies”. The research was completed on May 2019.
2.2.2. Study Selection
Two researchers (G.M., D.L.) independently analyzed the title, abstract, and full text of each English article to identify those that were eligible for the systematic review, according to the inclusion and exclusion criteria established above. Disagreements between reviewers were resolved by consensus. Articles that were published in other languages were assessed by a native speaker specialized in medical language. Articles in which the diagnosis of dementia was not defined or quantitative data were not available were excluded.
2.2.3. Data Collection Process
Two reviewers (G.M., D.L.) extracted the data, who also checked their methodological and clinical heterogeneity (D.L.). The information extracted from each article were as follows: study design (cohort, case-control, cross-sectional studies, or randomized clinical trial), participants characteristics, such as age and diagnosis of dementia, and quantitative data on participants (outcome measures), including the number of teeth present, number of retained roots, DMFT Index (Decayed Missing Filled Teeth Index), edentulousness and dentures, coronal and root caries, periodontal health, and its association with the onset or progression of dementia, oral mucosal disease, salivary flow, orofacial pain, oral hygiene, and need for dental treatment. Means and percentages were used for the principal outcome measures.
2.2.4. Quality assessment
Newcastle-Ottawa scale (NOS) [18] was used to assess the quality of the studies (Table 1, Table 2, Table 3 and Table 4). The highest score was 9 and the lowest one was 1 (average score was 5.5 or cohort studies, 6.1 for case-control studies, 4.6 for cross-sectional studies, and 5.5 for RCT). Most articles used the standardized method to examine oral health and the examination was considered to be adequate if a dentist performed it. With regard to “Comparability”, 30 of all the studies controlled for age or gender or both and in the case-control, cross-sectional studies, and RCT only 5 (1.98% of the non-cohort studies) described the non-response rate [14,19,20]. In almost all studies, the duration of follow-up period was longer than three months. The evaluated quality parameters are shown in Additional file 1–4.

Table 1.
Quality assessment for cohort studies (Additional file 1).
Table 2.
Quality assessment for case-control studies (Additional file 2).
Table 3.
Quality assessment for cross-sectional studies (Additional file 3).
Table 4.
Quality assessment for RCT (Additional file 4).
3. Results
3.1. Study Selection and Characteristics
A total of 922 studies that were published between 1990 and 2019 were identified from database searches. Among these articles, after examining titles and abstracts and the full texts of the remaining, only 56 met the inclusion criteria and were consequently included for quality assessment and data extraction. One study was added after scanning the reference list of the included articles [39]. All of the studies were analyzed with regard to quality while using the Newcastle-Ottawa Scale (NOS). Figure 1 shows the flow chart of publication assessment.
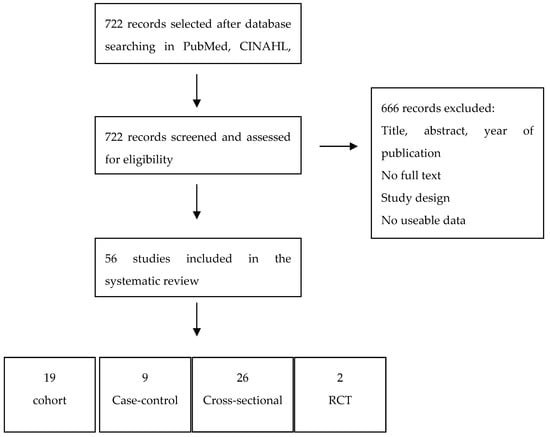
Figure 1.
PRISMA flow diagram.
The detailed characteristics about the 56 included studies are presented in Table 5, and Table 6, with reference to author and year of publication, study design, case and controls, mean age of participants, dementia measure, and measure of oral health. This review included 19 cohort studies, 9 case-control-studies, 26 cross-sectional studies, and two randomized clinical trials. Almost all of the articles were in English, except for Sumi et al. article, which was written in Japanese [33]. A native Japanese speaker, who extracted the data included in the review, examined this article.
Table 5.
List of studies about coronal/root caries, number of remained teeth/retained roots, DMFT, periodontal disease, utilization of dentures, salivary flow, oral hygiene, and oral mucosal lesions in elderly with and without dementia.
Table 6.
List of studies about the relationship between dementia and periodontal disease.
The studies that were selected for the review included in total 8466 participants with dementia and 6797 participants without dementia. In particular, selected studies regarding the association between periodontal disease and dementia included 4698 participants with periodontal disease or history of teeth extraction, 3132 elderly without periodontal disease, 60 subjects with dementia, and 2885 without dementia. In the included studies, the diagnosis of dementia was performed while using DSM-III and IV [70], ICD-9 and 10 (International Classification of Disease [71]), NINCDS-ADRDA (National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s disease and Related Disorders Association [72]), Minimental State examination [73] (MMSE), and other additional measures (e.g., computed tomography, magnetic resonance imaging, CDR [74]).
3.2. Results of Individual Studies
The number of present teeth was one of the most used measures for assessing oral health. In particular, from the included studies it came to light that the range within the two groups varied between 2.0 to 20. 2 for people without dementia and between 1.7 to 20.5 for people with dementia. According to Delwel et al. [53], the number of present teeth was lower in the participants with dementia (median = 2.0, IQR = 0.0–18.0) than in people with MCI (median = 18.0, IQR = 5.5–24.0). However, this study underlined that, if only dentate participants were considered, no significant differences were recorded between the two groups (median = 18.0, IQR = 9.0-24-0) (Table 7). The review showed that coronal and root caries were more common in people with dementia that in people without dementia: coronal caries varied between 0.1–2.9 [43,54,55] and 0.0-1-0, respectively [21,54], and root caries varied between 0.6–4.9 [43,54,55] in participants with dementia and 0.3–1.7 [13,54,55] in normal cognitive participants. For retained roots, the range was between 0.0–1.2 [54] in people without dementia and between 0.2–10 [21,54] in people with dementia. Moreover, Delwel et al. [53] demonstrated that dentate participants with dementia had more coronal caries (median = 1.0, IQR = 0.0–2.0), root caries, and retained roots (median = 0.0, IQR = 0.0–1.0) than dentate people with MCI (Table 8. With regards to the DMFT Index (Table 9), the lowest one was 14.9 in the study by Srilapanan et al. In general, the DMFT index did not show a significant difference within the two groups (19.7–26.1 in healthy people and 14.9–28.0 in people with dementia), except for one study, which demonstrated that the DMFT Index was 25.5 in people without dementia and 28.0 in people with dementia.
Table 7.
Results about the number of present teeth.
Table 8.
Results about coronal/root caries and retained roots.
Table 9.
Results about the DMFT Index.
Most of the participants with dementia presented gingival bleeding or inflammation [23,48] (Table 10). According to De Souza [24], the Gingival Bleeding Index was 46.0% in the elderly with dementia and periodontal infections were most common in the latter (58.6%) than in normal cognitive participants (26.7%). 73.8% of the Delwel et al. [53] study included patients had periodontal pockets of ≥4 mm, 18.8% of them had one or more teeth with mobility grade 2, and 5.8% had one or more teeth with mobility grade 3.
Table 10.
Results about gingival and periodontal disease.
Zenthöfer [36,37,44] demonstrated that the Gingival Bleeding Index of people with dementia was 43.8 to 53.8% and confirmed De Souza’s results, proving that people with dementia suffer from periodontitis more than people without dementia (community periodontal index of treatment needs was 3.1–3.4 in dementia people and 2.7–2.8 in non dementia people [36,37]).
Nine of the included studies found no significant differences between both groups with regards to oral hygiene [21,22,27,45,61,62,64,65,66,67] and five studies demonstrated a higher level of plaque in dementia people [14,36,43,56,65]. The Plaque Index by Silness and Loe was 0.7 in the study by Chalmers et al. [13], 2.5 in the study by Gil-Montoya [14] in the elderly with dementia, and 2.0 in the study by Delwel et al. [53]. Sumi et al. [33] showed a Plaque Index by Quigley and Hein of 1.6. O’Leary Plaque Index was significantly higher in dementia people (90.1%) than in non dementia people [36] (73.3%). Finally, Ribeiro [65] et al. established that the Oral Hygiene Index by Green and Vermillion is higher in participants with dementia (4.5) than in participants without dementia (2.2). A significantly higher Debris Index in people with moderate to severe dementia was found [43].
Furthermore, edentuloussnes was a condition that affected a large percentage of the elderly, in particular 11.6 to 72.7% of the elderly with dementia [66,67] and 14.0 to 70% of the elderly without dementia [38,45]. Within partially or totally edentulous participants, denture utilization varied between these percentages: 17.0–81.8% in normal cognitive people and 5.0 to 100% in people with cognitive impairment [27,31] (Table 11).
Table 11.
Results about dentures and edentulousness.
Data about orofacial pain were extracted from seven of the included studies [13,24,39,40,45,52]. The percentage of the elderly with dementia suffering from orofacial pain was higher than that of participants without dementia: 7.4 to 21.7%, 6.7 to 18.5%, respectively. The cross-sectional study by Delwel et al. [53] carefully examined the presence of orofacial pain in the elderly with dementia or MCI, while using the OPS-NVI [12] and self reported pain. The OPS-NVI was 4% in rest, 10% during drinking, 19% during chewing, and 22% during oral hygiene care. Pain reported by participants with dementia or MCI was 25.7% overall (Table 12).
Table 12.
Results about Orofacial pain.
The feeling of a dry mouth or xerostomia reached the percentages of 22.0% in people with dementia and 8.4% in people without dementia [33] and it was present in 9.1–45% of the cases and 8.4–20.0% of the controls [40,41,42,43]. Gil-Montoya [58] showed a more drug-induced xerostomia in cases (68.5–72.2%) than in the controls (36.5%).
Oral pathology, such as stomatitis and candidiasis, was most common in the cases than in controls. Chu et al. [38] and other authors [24,39,41] reported a percentage of candidiasis of 3.6–30% for cases and 0.0–5.0% for controls. Furthermore, 18.1–59.1% of cases and 0.0–7.4% of controls showed stomatitis [13,27,40].
In conclusion, with regards to the oral care need, the included studies [13,47,49,50,61,64,67] reported a need of 21% for cleaning teeth and dentures in the elderly with dementia. Chalmers et al. [47] demonstrated that, with an increasing severity of cognitive impairment, there is also an increase of oral care need: the assistance need for cleaning teeth and dentures in severe dementia was 100.0%, as compared to the assistance need in moderate dementia, which was 57.2% (teeth) and 97.3% (dentures). Regarding periodontal disease (Table 13), Dintica et al. [25] and Ide et al. [31] found that the mean change (decrease) in MMSE score due to tooth loss was, respectively, −0.94 to 0.37 (nine months follow-up, adjusted for age, sex, and education) and −3.6 to −0.03 (six months follow-up), establishing a significant association between tooth loss and the progression of cognitive impairment. The crude hazard ratio of dementia according to the number of remaining/lost teeth was 1.6 [10,34]. Tiisanoja et al. [68] demonstrated that subjects with pocket depth ≥4 mm had an increased, but not statistically significant, risk of developing Alzheimer’s Disease (Relative risk: 1.54). Furthermore, Yoo et al. [35] demonstrated that periodontal treatment lead to a significant decrease in the incidence of dementia. The prospective community-based study by Kato et al. [30] showed that the number of natural teeth was significantly associated with an individual’s MMSE score: the percentage of cognitively normal subjects (MMSE scores: 27–30) significantly decreased with a decrease in the number of natural teeth (number of teeth = 5–9, percentage of participants without cognitive impairment = 26.7%; number of teeth = 15–19; and, percentage of normal cognitive participants = 44.8%). Kato et al. also demonstrated that the use of artificial teeth was associated with cognitive function preservation.
Table 13.
Association between periodontal disease and dementia.
4. Discussion
The purpose of this systematic review was to examine studies regarding oral health in the elderly with and without dementia and to investigate the relationship between periodontal status and dementia. As reported in a recent review by Delwel et al. [75], the analysis of this study showed no significant differences between the case and controls with regards to the number of present teeth [13,21,29,43,53,56,61,67,69] and to the DMFT Index [27,38,61,65]. However, the DMFT categories separately, “decay”, “missing”, and “filled”, give a better indication of disease and treatment need compared to the index, which reports dental caries history as a whole. Coronal and root caries and retained roots are most common in people with dementia [21,56,65], and this condition might be explained by cognitive and behavioral deterioration, which reduced the ability to perform routine oral care [76]. In the elderly with dementia saliva flow rates decreases [32], eating habits change (more cariogenic food) [51,56,61,77], and motor skills and coordination worsen [65], which leads to a lower chewing and swallowing efficiency [56,77].
Another important point to be considered is the oppositional and aggressive behavior towards oral care and decreased communication skills, which represent barriers to oral hygiene and assistance. These obstacles could be overcome by performing oral care education to caregivers and by increasing dental checks of the elderly with dementia [62,78,79].
Moreover, the recent observational study by Delwel et al. [53] recorded a significant correlation between the cognitive impairment level and the number of present/missing/restored teeth and retained roots, which suggests that dementia could have a negative impact on oral health.
Concerning oral soft tissues, this study confirmed Delwel’s et al. review results [80]: gingival bleeding, periodontal disease, mucosal lesions, and xerostomia were found at higher rates in participants with cognitive impairment. Dry mouth was more common in the elderly, who used medication or had radiotherapy history (head and neck) or autoimmune disease [32].
Approximately the same percentage of the elderly either with or without dementia wore dentures [13,42]. However, people with an advanced dementia degree showed a lower use of dentures, as compared to people with moderate dementia, because of the musculature, salivary flow decrease, and lower tolerance of dentures.
The deterioration of verbal communication skills and the higher prevalence of oral disease might cause a higher suffering to people with dementia, due to orofacial pain [45,50,52,53]. In this systematic review, the new information included concern the potential role of periodontal disease as a risk factor for developing cognitive impairment. In fact, all of the studies included in Table 10 demonstrated an association between teeth loss due to periodontal disease and the onset of dementia [10,25,30,31,34,35,60]. This association is based on biological mechanisms: subjects with periodontal disease or antibodies to periodontal bacterial flora show an increased systemic proinflammatory state, which lead to an increase of the cognitive decline rate [31]. According to Yoo et al., the more teeth are lost, the higher incidence of dementia is. The author also stated that monitoring cognitive status in patients with extensive teeth loss could lead to an early diagnosis of dementia. The significant association between the number of natural teeth and the MMSE score was also confirmed in the study by Kato et al., which suggest that the use of artificial teeth could help to preserve the cognitive function.
Strengths and Limitations
The most important limitation of this study is the result of the quality assessment of the articles, since more than half of the included studies have a score equal or below 5. The number of high quality studies was low and no homogeneity can be found. For this reason, it was impossible to perform a meta-analysis. In the included studies, several different measures were used to evaluate oral health status and some studies did not distinguish between the elderly with and without dementia.
The main strength of this review is the systematic approach and involvement of a multidisciplinary team (dentists, neuropsychologist, pain specialist). In addition, in almost all of the studies reviewed, oral examinations are structured and standardized, and were carried out by dentists.
5. Conclusions
The elderly with dementia show a higher level of plaque, coronal and root caries, retained roots, gingival, and periodontal disease. Further attention is needed regarding orofacial pain, which is very common in dementia people. Poor oral health within this group could be increased by the reduction of submandibular salivary flow, deterioration of cognitive functions, motor and communication skills, and aggressive behavior. Caregivers should be educated and dentist’s checks in nursing homes should be enhanced in order to improve the oral health status of the elderly with dementia. Our contribution highlights the relationship between periodontal disease and dementia. Teeth loss due to periodontal disease increases the risk of cognitive function deterioration. However, the specific mechanisms of this association need further investigation.
Author Contributions
Conceptualization, D.L. and G.M.; methodology, F.D.V.; validation A.L. and F.C.; formal analysis, D.D.S.; investigation, G.M.; data curation, D.L.; writing—original draft preparation, G.M.; writing—review and editing, D.L.; visualization, F.C.; supervision, M.P.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- National Institute on Aging; National Institutes of Health, U.S.; Department of Health and Human Services. Global Health and Aging; World Health Organisation: Geneva, Switzerland, 2011. [Google Scholar]
- Lopez, R.; Smith, P.C.; Göstemeyer, G.; Schwendicke, F. Ageing, dental caries and periodontal diseases. J. Clin. Periodontol. 2017, 44 (Suppl. 18), S145–S152. [Google Scholar] [CrossRef] [PubMed]
- Nangle, M.R.; Riches, J.; Grainger, S.A.; Manchery, N.; Sachdev, P.S.; Henry, J.D. Oral Health and Cognitive Function in Older Adults: A systematic Review. Gerodontology 2019, 65, 659–672. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.; Fillenbaum, G.G.; Plassman, B.L.; Guo, L. Association Between Oral Health and Cognitive Status: A Systematic Review. J. Am. Geriatr. Soc. 2016, 64, 739–751. [Google Scholar] [CrossRef] [PubMed]
- Moritz, D.J.; Kasl, S.V.; Berkman, L.F. Cognitive Functioning and the Incidence of Limitations in Activities of Daily Living in an Elderly Community Sample. Am. J. Epidemiol. 1995, 141, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Ship, J.A.; De Carli, C.; Friedland, R.P.; Baum, B.J. Diminished submandibular salivary flow in dementia of the Alzheimer type. J. Gerontol. 1990, 45, M61–M66. [Google Scholar] [CrossRef] [PubMed]
- Ship, J.A.; Pillemer, S.R.; Baum, B.J. Xerostomia and the geriatric patient. J. Am. Geriatr. Soc. 2002, 50, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.; Hopcraft, M.; Morgan, M. Dental caries in Victorian nursing homes. Aust. Dent. J. 2014, 59, 321–328. [Google Scholar] [CrossRef]
- Martande, S.S.; Pradeep, A.R.; Singh, S.P.; Kumari, M.; Suke, D.K.; Raju, A.P.; Naik, S.B.; Singh, P.; Guruprasad, C.N.; Chatterji, A. Periodontal Health Condition in Patients With Alzheimer’s Disease. Am. J. Alzheimers Dis. Other Demen. 2014, 29, 498–502. [Google Scholar] [CrossRef]
- Lee, Y.T.; Lee, H.C.; Hu, C.J.; Huang, L.K.; Chao, S.P.; Lin, C.P.; Su, E.C.; Lee, Y.C.; Chen, C.C. Periodontitis as a Modifiable Risk Factor for Dementia: A Nationwide Population-Based Cohort Study. Am. Geriatr. Soc. 2017, 65, 301–305. [Google Scholar] [CrossRef]
- Ewan, V.; Staines, K. Diagnosis and management of oral mucosal lesions in older people: A review. Rev. Clin. Gerontol. 2008, 18, 115–128. [Google Scholar] [CrossRef]
- De Vries, M.W.; Visscher, C.; Delwel, S.; van der Steen, J.T.; Pieper, M.J.C.; Scherder, E.J.A.; Achterberg, W.P.; Lobbezoo, F. Orofacial Pain during Mastication in People with Dementia: Reliability Testing of the Orofacial Pain Scale for Non-Verbal Individuals. Behav. Neurol. 2016, 2016, 3123402. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J.M.; Carter, K.D.; Spencer, A.J. Oral diseases and conditions in community-living older adults with and without dementia. Spec. Care Dent. 2003, 23, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Gil-Montoya, J.A.; Sanchez-Lara, I.; Carnero-Pardo, C.; Fornieles-Rubio, F.; Montes, J.; Barrios, R.; Gonzalez-Moles, M.A.; Bravo, M. Oral Hygiene in the Elderly with Different Degrees of Cognitive Impairment and Dementia. J. Am. Geriatr. Soc. 2017, 65, 642–647. [Google Scholar] [CrossRef]
- Cerutti-Kopplin, D.; Feine, J.; Padilha, D.M.; de Souza, R.F.; Ahmadi, M.; Rompré, P.; Booij, L.; Emami, E. Tooth Loss Increases the Risk of Diminished Cognitive Function: A Systematic Review and Meta-analysis. JDR Clin. Trans. Res. 2016, 1, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Noble, J.M.; Scarmeas, N.; Papapanou, P.N. Poor Oral Health as a Chronic, Potentially, Modifiable Dementia Risk Factor: Review of Literature. Curr. Neurol. Neurosci. Rep. 2013, 13, 384. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Petersen, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses; Department of Epidemiology and Community Medicine, University of Ottawa, Canada: Ottawa, ON, Canada, 2012. [Google Scholar]
- Hoeksema, A.R.; Peters, L.L.; Raghoebar, G.M.; Meijer, H.J.A.; Vissink, A.; Visser, A. Oral health status and need for oral care of care-dependent indwelling elderly: From admission to death. Clin. Oral Investig. 2017, 21, 2189–2196. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Wu, B.; Zhao, Q.; Guo, Q.; Meng, H.; Yu, L.; Zheng, L.; Hong, Z.; Ding, D. Association between tooth loss and cognitive function among 3063 Chinese older adults: A community-based study. PLoS ONE 2015, 10, e0120986. [Google Scholar] [CrossRef]
- Chalmers, J.M.; Carter, K.D.; Spencer, A.J. Caries incidence and increments in community-living older adults with and without dementia. Gerodontology 2002, 19, 80–94. [Google Scholar] [CrossRef]
- Chalmers, J.M.; Carter, K.; Spencer, A. Oral health of Adelaide nursing home residents: Longitudinal study. Aust. J. Ageing 2004. [Google Scholar] [CrossRef]
- Chen, X.; Shuman, S.K.; Hodges, J.S.; Gatewood, L.C.; Xu, J. Patterns of tooth loss in older adults with and without dementia: A retrospective study based on a Minnesota cohort. J. Am. Geriatr. Soc. 2010, 58, 2300–2307. [Google Scholar] [CrossRef] [PubMed]
- De Souza Rolim, T.; Fabri, G.M.; Nitrini, R.; Anghinah, R.; Teixeira, M.J.; de Siqueira, J.T.; Cestari, J.A.; de Siqueira, S.R. Oral infections and orofacial pain in Alzheimer’s disease: A case-control study. J. Alzheimers Dis. 2014, 38, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Dintica, C.S.; Rizzuto, D.; Marseglia, A.; Kalpouzos, G.; Welmer, A.K.; Wårdh, I.; Bäckman, L.; Xu, W. Tooth loss is associated with accelerated cognitive decline and volumetric brain differences: A population-based study. Neurobiol. Aging 2018, 67, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Ellefsen, B.; Holm-Pedersen, P.; Morse, D.E.; Schroll, M.; Andersen, B.B.; Waldemar, G. Assessing caries increments in elderly patients with and without dementia: A one-year follow-up study. J. Am. Dent. Assoc. 2009, 140, 1392–1400. [Google Scholar] [CrossRef]
- Hatipoglu, M.G.; Kabay, S.C.; Güven, G. The clinical evaluation of the oral status in Alzheimer-type dementia patients. Gerodontology 2011, 28, 302–306. [Google Scholar] [CrossRef]
- Hoben, M.; Poss, J.W.; Norton, P.G.; Estabrooks, C.A. Oral/dental items in the resident assessment instrument–minimum data set 2.0 lack validity: Results of a retrospective, longitudinal validation study. Popul. Health Metr. 2016, 14, 36. [Google Scholar] [CrossRef]
- Jones, J.A.; Lavallee, N.; Alman, J.; Sinclair, C.; Garcia, R.I. Caries incidence in patients with dementia. Gerodontology 1993, 10, 76–82. [Google Scholar] [CrossRef]
- Kato, H.; Takahashi, Y.; Iseki, C.; Igari, R.; Sato, H.; Sato, H.; Koyama, S.; Tobita, M.; Kawanami, T.; Iino, M.; et al. Tooth Loss-associated Cognitive Impairment in the Elderly: A Community-based Study in Japan. Intern. Med. 2019, 58, 1411–1416. [Google Scholar] [CrossRef]
- Ide, M.; Harris, M.; Stevens, A.; Sussams, R.; Hopkins, V.; Culliford, D.; Fuller, J.; Ibbett, P.; Raybould, R.; Thomas, R.; et al. Periodontitis and cognitive decline in Alzheimer’s disease. PLoS ONE 2016, 11, e0151081. [Google Scholar] [CrossRef]
- Ship, J.A.; Puckett, S.A. Longitudinal study on oral health in subjects with Alzheimer’s disease. J. Am. Geriatr. Soc. 1994, 42, 57–63. [Google Scholar] [CrossRef]
- Sumi, Y.; Ozawa, N.; Michiwaki, Y.; Washimi, Y.; Toba, K. Oral conditions and oral management approaches in mild dementia patients. Nihon Ronen Igakkai Zasshi 2012, 49, 90–98. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Takeuchi, K.; Ohara, T.; Furuta, M.; Takeshita, T.; Shibata, Y.; Hata, J.; Yoshida, D.; Yamashita, Y.; Ninomiya, T. Tooth Loss and Risk of Dementia in the Community: The Hisayama Study. J. Am. Geriatr. Soc. 2017, 65, e95–e100. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.J.; Yoon, J.H.; Kang, M.J.; Kim, M.; Oh, N. The effect of missing teeth on dementia in older people: A nationwide population-based cohort study in South Korea. BMC Oral Health 2019, 19, 61. [Google Scholar] [CrossRef] [PubMed]
- Zenthöfer, A.; Schröder, J.; Cabrera, T.; Rammelsberg, P.; Hassel, A.J. Comparison of oral health among older people with and without dementia. Community Dent. Health 2014, 31, 27–31. [Google Scholar]
- Zenthöfer, A.; Cabrera, T.; Rammelsberg, P.; Hassel, A.J. Improving oral health of institutionalized older people with diagnosed dementia. Aging Ment. Health 2016, 20, 303–308. [Google Scholar] [CrossRef]
- Chu, C.H.; Ng, A.; Chau, A.M.; Lo, E.C. Oral health status of elderly Chinese with dementia in Hong Kong. Oral Health Prev. Dent. 2015, 13, 51–57. [Google Scholar] [CrossRef]
- Rolim Tde, S.; Fabri, G.M.; Nitrini, R.; Anghinah, R.; Teixeira, M.J.; Siqueira, J.T.; Cesari, J.A.; Siqueira, S.R. Evaluation of patients with Alzheimer’s disease before and after dental treatment. Arq. Neuropsiquiatr. 2014, 72, 919–924. [Google Scholar] [CrossRef]
- Kossioni, A.E.; Kossionis, G.E.; Polychronopoulou, A. Oral health status of elderly hospitalised psychiatric patient. Gerodontology 2012, 29, 272–283. [Google Scholar] [CrossRef]
- Leal, S.C.; Bittar, J.; Portugal, A.; Falcão, D.P.; Faber, J.; Zanotta, P. Medication in elderly people: Its influence on salivary pattern, signs and symptoms of dry mouth. Gerodontology 2010, 27, 129–133. [Google Scholar] [CrossRef]
- Nordenram, G.; Ryd-Kjellen, E.; Johansson, G.; Nordstrom, G.; Winblad, B. Alzheimer’s disease, oral function and nutritional status. Gerodontology 1996, 13, 9–16. [Google Scholar] [CrossRef]
- Warren, J.J.; Chalmers, J.M.; Levy, S.M.; Blanco, V.L.; Ettinger, R.L. Oral health of persons with and without dementia attending a geriatric clinic. Spec. Care Dent. 1997, 17, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Zenthöfer, A.; Baumgart, D.; Cabrera, T.; Rammelsberg, P.; Schröder, J.; Corcodel, N.; Hassel, A.J. Poor dental hygiene and periodontal health in nursing home residents with dementia: An observational study. Odontology 2017, 105, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Adam, H.; Preston, A.J. The oral health of individuals with dementia in nursing homes. Gerodontology 2006, 23, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Bomfim, F.M.S.; Chiari, B.M.; Roque, F.P. Fatores associados a sinais sugestivos de disfagia orofaríngea em idosas institucionalizadas. CoDAS 2013, 25, 154–163. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chalmers, J.M.; Hodge, C.; Fuss, J.M.; Spencer, A.J.; Carter, K.D. The prevalence and experience of oral diseases in Adelaide nursing home residents. Aust. Dent. J. 2002, 47, 123–130. [Google Scholar] [CrossRef]
- Chapman, P.J.; Shaw, R.M. Normative dental treatment needs of Alzheimer patients. Aust. Dent. J. 1991, 36, 141–144. [Google Scholar] [CrossRef]
- Chen, X.; Clark, J.J.; Naorungroj, S. Oral health in older adults with dementia living in different environments: A propensity analysis. Spec. Care Dent. 2013, 33, 239–247. [Google Scholar] [CrossRef]
- Chen, X.; Clark, J.J.; Naorungroj, S. Oral health in nursing home residents with different cognitive statuses. Gerodontology 2013, 30, 49–60. [Google Scholar] [CrossRef]
- Chen, X.; Clark, J.J.; Chen, H.; Naorungroj, S. Cognitive impairment, oral self-care function and dental caries severity in community-dwelling older adults. Gerodontology 2015, 32, 53–61. [Google Scholar] [CrossRef]
- Cohen-Mansfield, J.; Lipson, S. The underdetection of pain of dental etiology in persons with dementia. Am. J. Alzheimers Dis. Other Demen. 2002, 17, 249–253. [Google Scholar] [CrossRef]
- Delwel, S.; Scherder, E.J.A.; de Baat, C.; Binnekade, T.T.; van der Wouden, J.C.; Hertogh, C.M.P.M.; Maier, A.B.; Perez, R.S.G.M.; Lobbezoo, F. Orofacial pain and its potential oral causes in older people with mild cognitive impairment or dementia. J. Oral Rhabilit. 2019, 46, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Ellefsen, B.; Holm-Pedersen, P.; Morse, D.E.; Schroll, M.; Andersen, B.B.; Waldemar, G. Caries prevalence in older persons with and without dementia. J. Am. Geriatr. Soc. 2008, 56, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Ellefsen, B.S.; Morse, D.E.; Waldemar, G.; Holm-Pedersen, P. Indicators for root caries in Danish persons with recently diagnosed Alzheimer’s disease. Gerodontology 2012, 29, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Elsig, F.; Schimmel, M.; Duvernay, E.; Giannelli, S.V.; Graf, C.E.; Carlier, S.; Herrmann, F.R.; Michel, J.P.; Gold, G.; Zekry, D.; et al. Tooth loss, chewing efficiency and cognitive impairment in geriatric patients. Gerodontology 2015, 32, 149–156. [Google Scholar] [CrossRef]
- Eshkoor, S.A.; Hamid, T.A.; Nudin, S.S.; Mun, C.Y. Association between dentures and the rate of falls in dementia. Med. Devices 2014, 7, 225–230. [Google Scholar] [CrossRef]
- Gil-Montoya, J.A.; Barrios, R.; Sánchez-Lara, I.; Carnero-Pardo, C.; Fornieles-Rubio, F.; Montes, J.; Gonzalez-Moles, M.A.; Bravo, M. Prevalence of drug-induced xerostomia in older adults with cognitive impairment or dementia: An observational study. Drugs Aging 2016, 33, 611–618. [Google Scholar] [CrossRef]
- Kossioni, A.E.; Kossionis, G.E.; Polychronopoulou, A. Self-reported oral complaints in older mentally ill patient. Geriatr. Gerontol. Int. 2013, 13, 358–364. [Google Scholar] [CrossRef]
- Furuta, M.; Komiya-Nonaka, M.; Akifusa, S.; Shimazaki, Y.; Adachi, M.; Kinoshita, T.; Kikutani, T.; Yamashita, Y. Interrelationship of oral health status, swallowing function, nutritional status, and cognitive ability with activities of daily living in Japanese elderly people receiving home care services due to physical disabilities. Community Dent. Oral Epidemiol. 2013, 41, 173–181. [Google Scholar] [CrossRef]
- Hopcraft, M.S.; Morgan, M.V.; Satur, J.G.; Wright, F.A.C. Edentulism and dental caries in Victorian nursing homes. Gerodontology 2012, 29, e512–e519. [Google Scholar] [CrossRef]
- Lee, K.H.; Wu, B.; Plassman, B.L. Cognitive function and oral health-related quality of life in older adults. J. Am. Geriatr. Soc. 2013, 61, 1602–1607. [Google Scholar] [CrossRef]
- Minakuchi, S.; Takaoka, S.; Shimoyama, K.; Uematsu, H. Factors affecting denture use in some institutionalized elderly people. Spec. Care Dent. 2006, 26, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Philip, P.; Rogers, C.; Kruger, E.; Tennant, M. Oral hygiene care status of elderly with dementia and in residential aged care facilities. Gerodontology 2012, 29, e306–e311. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, G.R.; Costa, J.L.; Ambrosano, G.M.; Garcia, R.C. Oral health of the elderly with Alzheimer’s diseas. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 114, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Srisilapanan, P.; Jai-Ua, C. Oral health status of dementia patients in Chiang Mai Neurological Hospital. J. Med. Assoc. Thai 2013, 96, 351–357. [Google Scholar]
- Syrjälä, A.-M.H.; Ylöstalo, P.; Ruoppi, P.; Komulainen, K.; Hartikainen, S.; Sulkava, R.; Knuuttila, M. Dementia and oral health among subjects aged 75 years or older. Gerodontology 2012, 29, 36–42. [Google Scholar] [CrossRef]
- Tiisanoja, A.; Syrjala, A.M.; Tertsonen, M.; Komulainen, K.; Pesonen, P.; Knuuttila, M.; Hartikainen, S.; Ylostalo, P. Oral disease and inflammatory burden and Alzheimer’s disease among subjects aged 75 years or older. Spec. Care Dent. 2019, 39, 158–165. [Google Scholar] [CrossRef]
- Fjeld, K.G.; Mowe, M.; Eide, H.; Willumsen, T. Effect of electric toothbrush on residents’ oral hygiene: A randomized clinical trial in nursing homes. Eur. J. Oral Sci. 2014, 122, 142–148. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; Text. Revision DSM-IV-TR; American Psychiatric Association: Arlington, VA, USA, 2000. [Google Scholar]
- World Health Organization. ICD-10 International Statistical Classification of Diseases and Related Health Problems; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-mental state. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Morris, J.C. The clinical dementia rating (CDR): Current version and scoring rules. Neurology 1993, 43, 2412–2414. [Google Scholar] [CrossRef]
- Delwel, S.; Binnekade, T.T.; Perez, R.S.; Hertogh, C.M.; Scherder, E.J.; Lobbezzoo, F. Oral health and Orofacial pain in older people with dementia: A systematic review with focus on dental hard tissues. Clin. Oral Investig. 2017, 21, 17–32. [Google Scholar] [CrossRef] [PubMed]
- Weijenberg, R.A.F.; Delwel, S.; Ho, B.V.; van der Maarel-Wierink, C.D.; Lobbezoo, F. Mind your teeth-The relationship between mastication and cognition. Gerodontology 2019, 36, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Delwel, S.; Scherder, E.J.A.; Perez, R.S.G.M.; Hertogh, C.M.P.M.; Maier, A.B.; Lobbezoo, F. Oral function of older people with mild cognitive impairment or dementia. J. Oral Rehabilit. 2018, 45, 990–997. [Google Scholar] [CrossRef] [PubMed]
- Jablonski, R.A.; Therrien, B.; Mahoney, E.K.; Kolanowski, A.; Gabello, M.; Brock, A. An intervention to reduce care-resistant behavior in persons with dementia during oral hygiene: A pilot study. Spec. Care Dent. 2011, 31, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Willumsen, T.; Karlsen, L.; Naess, R.; Bjørntvedt, S. Are the barriers to good oral hygiene in nursing homes within the nurses or the patients? Gerodontology 2012, 29, e748–e755. [Google Scholar] [CrossRef] [PubMed]
- Delwel, S.; Binnekade, T.T.; Perez Roberto, S.G.; Hertogh, C.M.P.M.; Scherder, E.J.A.; Lobbezzoo, F. Oral hygiene and oral health in older people with dementia: A comprehensive review with focus on oral soft tissues. Clin. Oral Investig. 2018, 22, 93–108. [Google Scholar] [CrossRef] [PubMed]

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).