Interventional Effects of Weight-Loss Policy in a Healthy City among Participants with Metabolic Syndrome


 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
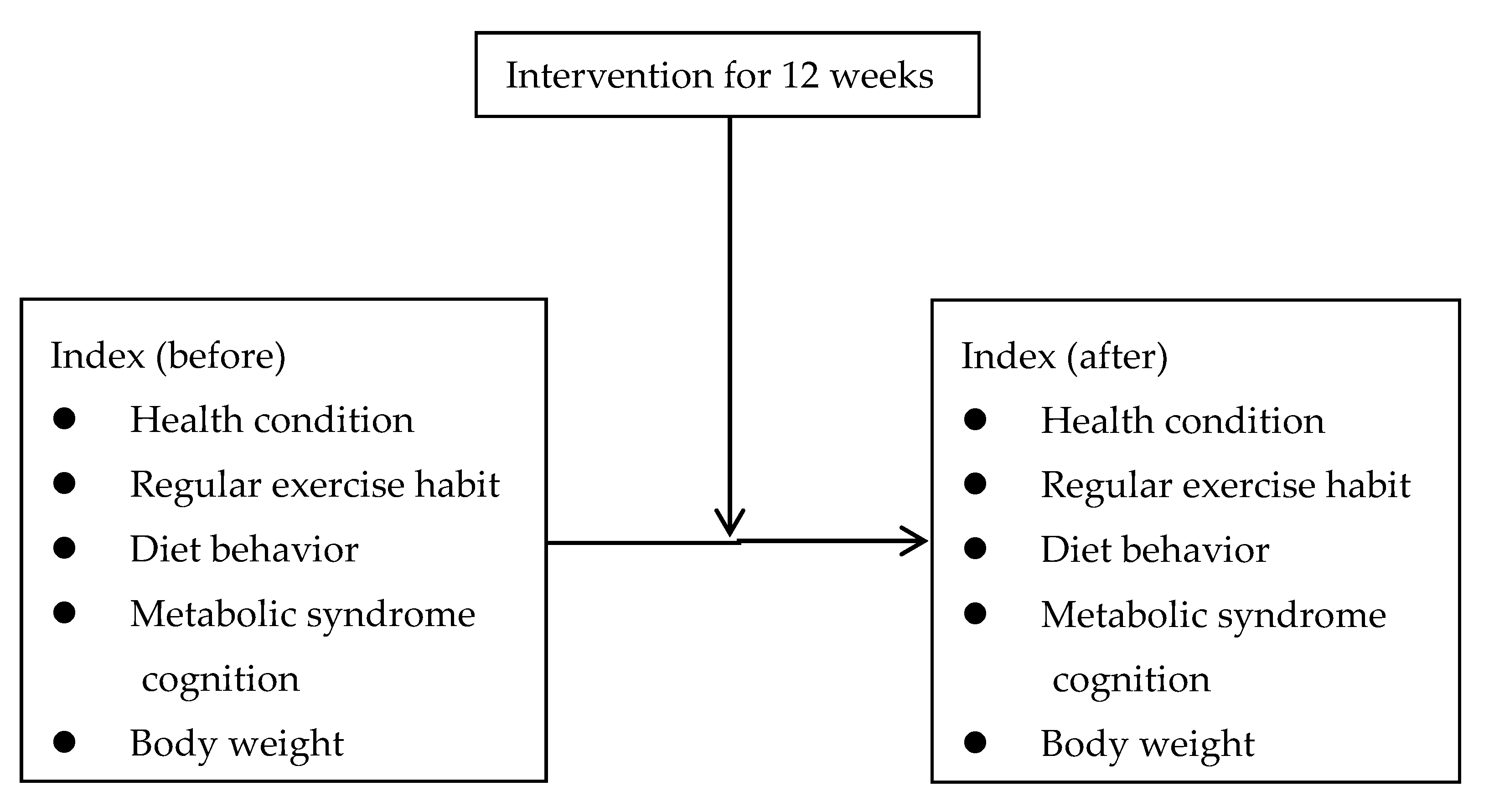
2.2. Intervention Program
- (1)
- Health condition standard score = (Sum of the total score of the 3 specific questions)/15 × 100
- (2)
- Exercise index score = Exercise intensity score × Exercise time score × Exercise frequency score
- (3)
- Diet behavior standard score is divided into 2 parts:Outside food behavior score = (Sum of the total score of the 6 specific questions)/24 × 100Cooking at home behavior score = (Sum of the total score of the 8 specific questions)/32 × 100
- (4)
- The standard score based on the recognition of MetS = (Number of correct answers for each question/Total number of selections for questions) × 100
2.3. Physical Status
2.4. Statistical Analysis
3. Results
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Neeland, I.J.; Singh, S.; McGuire, D.K.; Vega, G.L.; Roddy, T.; Reilly, D.F.; Castro-Perez, J.; Kozlitina, J.; Scherer, P.E. Relation of plasma ceramides to visceral adiposity, insulin resistance and the development of type 2 diabetes mellitus: The Dallas Heart Study. Diabetologia 2018, 61, 2570–2579. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Chiodini, P.; Colao, A.; Lenzi, A.; Giugliano, D. Metabolic syndrome and risk of cancer: A systematic review and meta-analysis. Diabetes Care 2012, 35, 2402–2411. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2018. Diabetes Care 2018, 41 (Suppl. 1), S13–S27. [Google Scholar] [CrossRef] [PubMed]
- Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [CrossRef]
- Grundy, S.M.; Brewer, H.B.; Cleeman, J.I.; Smith, S.C.; Lenfant, C. Definition of metabolic syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation 2004, 109, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Cho, L.W. Metabolic syndrome. Singap. Med. J. 2011, 52, 779–785. [Google Scholar]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar]
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.L.; Eisenberg, M.J. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef]
- Wilson, P.W.; D’Agostino, R.B.; Parise, H.; Sullivan, L.; Meigs, J.B. Metabolic syndrome as a precursor of cardiovascular disease and type 2 diabetes mellitus. Circulation 2005, 112, 3066–3072. [Google Scholar] [CrossRef]
- Ford, E.S. Risks for all-cause mortality, cardiovascular disease, and diabetes associated with the metabolic syndrome: A summary of the evidence. Diabetes Care 2005, 28, 1769–1778. [Google Scholar] [CrossRef]
- Resnick, H.E.; Jones, K.; Ruotolo, G.; Jain, A.K.; Henderson, J.; Lu, W.; Howard, B.V. Insulin resistance, the metabolic syndrome, and risk of incident cardiovascular disease in nondiabetic american indians: The Strong Heart Study. Diabetes Care 2003, 26, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Huh, J.H.; Yadav, D.; Kim, J.S.; Son, J.W.; Choi, E.; Kim, S.H.; Shin, C.; Sung, K.C.; Kim, J.Y. An association of metabolic syndrome and chronic kidney disease from a 10-year prospective cohort study. Metabolism 2017, 67, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Kitiyakara, C.; Yamwong, S.; Cheepudomwit, S.; Domrongkitchaiporn, S.; Unkurapinun, N.; Pakpeankitvatana, V.; Sritara, P. The metabolic syndrome and chronic kidney disease in a Southeast Asian cohort. Kidney Int. 2007, 71, 693–700. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Muntner, P.; Hamm, L.L.; Jones, D.W.; Batuman, V.; Fonseca, V.; Whelton, P.K.; He, J. The metabolic syndrome and chronic kidney disease in U.S. adults. Ann. Intern. Med. 2004, 140, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Yahia, N.; Brown, C.; Rapley, M.; Chung, M. Assessment of college students’ awareness and knowledge about conditions relevant to metabolic syndrome. Diabetol. Metab. Syndr. 2014, 6, 111. [Google Scholar] [CrossRef] [PubMed]
- Rogers, R.W. A protection motivation theory of fear appeals and attitude change. J. Psychol. 1975, 91, 93–114. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.C.; Kuo, H.W.; Lin, C.C. Current status and policy planning for promoting age-friendly cities in Taitung County: Dialogue between older adults and service providers. Int. J. Environ. Res. Public Health 2018, 15, 2314. [Google Scholar] [CrossRef]
- Stefani, L.; Galanti, G. Physical Exercise Prescription in Metabolic Chronic Disease. Adv. Exp. Med. Biol. 2017, 1005, 123–141. [Google Scholar]
- Moghetti, P.; Bacchi, E.; Brangani, C.; Donà, S.; Negri, C. Metabolic Effects of Exercise. Front. Horm. Res. 2016, 47, 44–57. [Google Scholar]
- Do Rosário Pinto, M.; Parreira, P.M.D.S.; Basto, M.L.; Dos Santos Mendes Mónico, L. Impact of a structured multicomponent educational intervention program on metabolic control of patients with type 2 diabetes. BMC Endocr. Disord. 2017, 17, 77. [Google Scholar] [CrossRef]
- Gamiochipi, M.; Cruz, M.; Kumate, J.; Wacher, N.H.; DIMSS Study Group. Effect of an intensive metabolic control lifestyle intervention in type-2 diabetes patients. Patient Educ. Couns. 2016, 99, 1184–1189. [Google Scholar] [CrossRef] [PubMed]
- Sumamo, E.; Ha, C.; Korownyk, C.; Vandermeer, B.; Dryden, D.M. Lifestyle Interventions for Four Conditions: Type 2 Diabetes, Metabolic Syndrome, Breast Cancer, and Prostate Cancer; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2011. [Google Scholar]


{kind=link}
| Township | Pre-Test | Post-Test | ||||
|---|---|---|---|---|---|---|
| n | % | Response Rate | n | % | Response Rate | |
| Miaoli | 296 | 14.3 | 100.0 | 236 | 12.5 | 79.7 |
| Yuanli | 160 | 7.7 | 100.0 | 126 | 6.7 | 78.8 |
| Tongxiao | 159 | 7.7 | 100.0 | 158 | 8.4 | 99.4 |
| Zhunan | 148 | 7.2 | 100.0 | 146 | 7.7 | 98.6 |
| Toufen | 243 | 11.8 | 100.0 | 177 | 9.4 | 72.8 |
| Houlong | 107 | 5.2 | 100.0 | 107 | 5.7 | 100.0 |
| Zhuolan | 48 | 2.3 | 100.0 | 48 | 2.5 | 100.0 |
| Dahu | 78 | 3.8 | 100.0 | 77 | 4.1 | 98.7 |
| Gongguan | 84 | 4.1 | 100.0 | 82 | 4.3 | 97.6 |
| Tongluo | 97 | 4.7 | 100.0 | 96 | 5.1 | 99.0 |
| Nanzhuang | 46 | 2.2 | 100.0 | 46 | 2.4 | 100.0 |
| Touwu | 114 | 5.5 | 100.0 | 114 | 6.1 | 100.0 |
| Sanyi | 104 | 5.0 | 100.0 | 89 | 4.7 | 85.6 |
| Xihu | 104 | 5.0 | 100.0 | 104 | 5.5 | 100.0 |
| Zaoqiao | 85 | 4.1 | 100.0 | 85 | 4.5 | 100.0 |
| Sanwan | 48 | 2.3 | 100.0 | 48 | 2.5 | 100.0 |
| Shitan | 80 | 3.9 | 100.0 | 79 | 4.2 | 98.8 |
| Tai’an | 67 | 3.2 | 100.0 | 67 | 3.6 | 100.0 |
| Total | 2068 | 100 | 100.0 | 1886 | 100 | 91.2 |
| Sessions | Objectives | A Summary of Topics and Activities |
|---|---|---|
| Healthy eating | To increase awareness of the benefits of healthy eating | -Set one day per month as “vegetable and fruit healthy day”: media broadcasting promotion movie on the same day -Promote a healthy restaurant: eat local food and create new menu -Hold healthy eating contest: assist restaurant to prepare local food and develop healthy eating -Develop campus vegetable and fruit project: assist and design healthy eating project in college and university -Recruit vending carts selling fresh vegetable dishes to remote areas -Develop a convenient shopping environment for vegetables and fruit in offices -Provide free healthy menu: set out low calorie high fiber menu in high density population area -Develop organic vegetable and fruit planting: combine food scraps activity and assign planting section to provide free organic vegetables and fruit to citizens |
| Regular exercise | To increase exercise capacity gradually | -Provide healthy recreational sports map: set the flash board for the length and calorie expenditure of regular walking -Combination of exercise and breaking through the barricade: apply the exercise map resource (8 exercise spots set by 18 towns) and encourage students to participate the physical activity -Apply exercise map to civil departments; Miaoli County Government holds outdoor recreation and physical activity on a holiday |
| Healthy weight loss | To prevent the risk of metabolic syndrome | -Evaluation by questionnaire (cause of overweight environmental assessment, exercise and eat healthy investigation) and weight scale -Screening: (i) analyze and compare the improvements of participants’ recognition, attitude, and behavior after 12 weeks of public health education; (ii) screen participants’ body weight and follow-up each week; (iii) observe the effect of weight loss and the ratio of regain weight again. -Evaluate the status of improvements: (i) compare participants who exercise regularly before and after; (ii) compare participants who maintain a healthy diet before and after; (iii) analyze body weight before and after. |
| Characteristics | Category | n | Mean | SD | t/F | Post Hoc |
|---|---|---|---|---|---|---|
| Sex | Male (1) | 561 | 72.49 | 15.81 | −0.02 | |
| Female (2) | 1415 | 72.50 | 16.20 | |||
| Age | 20–29 (1) | 112 | 71.72 | 12.82 | 2.81* | (7) > (3), (4), (5) |
| 30–39 (2) | 319 | 73.64 | 11.40 | |||
| 40–49 (3) | 391 | 71.81 | 15.59 | |||
| 50–59 (4) | 398 | 71.90 | 16.20 | |||
| 60–69 (5) | 354 | 71.79 | 18.32 | |||
| 70–79 (6) | 275 | 72.55 | 19.54 | |||
| 80–89 (7) | 77 | 79.07 | 11.79 | |||
| Birthplace | Weinan (1) | 691 | 71.73 | 16.46 | 2.67 * | (3) > (1), (2), (4) |
| Hakka (2) | 1137 | 72.89 | 15.96 | |||
| Aboriginal (3) | 62 | 77.03 | 11.92 | |||
| Other provinces (4) | 70 | 70.70 | 17.85 | |||
| Education level | Elementary school or under level (1) | 564 | 73.01 | 17.44 | 2.51 * | (5) > (3) |
| Junior high school (2) | 274 | 73.52 | 15.29 | |||
| High school (3) | 337 | 70.74 | 17.05 | |||
| College (4) | 622 | 72.01 | 14.68 | |||
| Graduate institute (5) | 157 | 74.96 | 14.37 | |||
| Marital status | Celibate (1) | 224 | 72.38 | 13.55 | 0.26 | |
| Married (2) | 1560 | 72.36 | 16.40 | |||
| Separated/Divorced (3) | 41 | 71.21 | 14.62 | |||
| Widowed (4) | 144 | 73.40 | 16.48 | |||
| Religion | None (1) | 563 | 73.75 | 14.09 | 2.38 | |
| Taoism (2) | 730 | 72.42 | 16.07 | |||
| Buddhism (3) | 506 | 71.05 | 18.43 | |||
| I-Kuan Tao (4) | 36 | 73.55 | 12.93 | |||
| Christian/Catholic (5) | 102 | 74.60 | 11.92 | |||
| Working situation | None (housekeeper) (1) | 710 | 73.72 | 16.00 | 1.69 | |
| Unemployed (2) | 43 | 69.96 | 16.79 | |||
| Retired (3) | 219 | 71.37 | 20.03 | |||
| Part time (4) | 68 | 72.53 | 16.21 | |||
| Full time (5) | 891 | 72.14 | 14.54 | |||
| Occupational class | Public service (1) | 190 | 70.17 | 16.72 | 4.52 *** | (2) > (4) |
| Teach (2) | 457 | 73.90 | 14.06 | |||
| Agriculture (3) | 77 | 74.28 | 13.86 | |||
| Craft (4) | 121 | 68.60 | 15.91 | |||
| Business (5) | 47 | 69.26 | 15.31 | |||
| Freelance (6) | 99 | 69.24 | 16.50 |
| Index | n | Before | After | Paired T |
|---|---|---|---|---|
| Metabolic syndrome cognition | 1612 | 56.80 ± 26.77 | 73.37 ± 23.95 | 23.12 *** |
| Exercise index score | 1747 | 36.89 ± 26.44 | 41.01 ± 24.78 | 4.80 *** |
| Diet behavior standard score | 1741 | 72.31 ± 16.24 | 75.64 ± 14.85 | 6.35 *** |
| Health condition standard score | 1827 | 63.43 ± 12.75 | 64.17 ± 12.98 | 1.76 |
| Intervention | Pre-Test | Post-Test | Chi-Square | ||||||
|---|---|---|---|---|---|---|---|---|---|
| No | Yes | No | Yes | ||||||
| n | % | n | % | n | % | n | % | ||
| Regular exercise measures | 710 | 50.6 | 694 | 49.4 | 645 | 45.9 | 759 | 54.1 | 6.09 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tai, H.-C.; Tzeng, I.-S.; Liang, Y.-C.; Liao, H.-H.; Su, C.-H.; Kung, W.-M. Interventional Effects of Weight-Loss Policy in a Healthy City among Participants with Metabolic Syndrome. Int. J. Environ. Res. Public Health 2019, 16, 323. https://doi.org/10.3390/ijerph16030323
Tai H-C, Tzeng I-S, Liang Y-C, Liao H-H, Su C-H, Kung W-M. Interventional Effects of Weight-Loss Policy in a Healthy City among Participants with Metabolic Syndrome. International Journal of Environmental Research and Public Health. 2019; 16(3):323. https://doi.org/10.3390/ijerph16030323
Chicago/Turabian StyleTai, Hsu-Chih, I-Shiang Tzeng, Yen-Ching Liang, Hsiu-Hui Liao, Chun-Hsien Su, and Woon-Man Kung. 2019. "Interventional Effects of Weight-Loss Policy in a Healthy City among Participants with Metabolic Syndrome" International Journal of Environmental Research and Public Health 16, no. 3: 323. https://doi.org/10.3390/ijerph16030323
APA StyleTai, H.-C., Tzeng, I.-S., Liang, Y.-C., Liao, H.-H., Su, C.-H., & Kung, W.-M. (2019). Interventional Effects of Weight-Loss Policy in a Healthy City among Participants with Metabolic Syndrome. International Journal of Environmental Research and Public Health, 16(3), 323. https://doi.org/10.3390/ijerph16030323