Is There a Difference in the Utilisation of Inpatient Services Between Two Typical Payment Methods of Health Insurance? Evidence from the New Rural Cooperative Medical Scheme in China

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
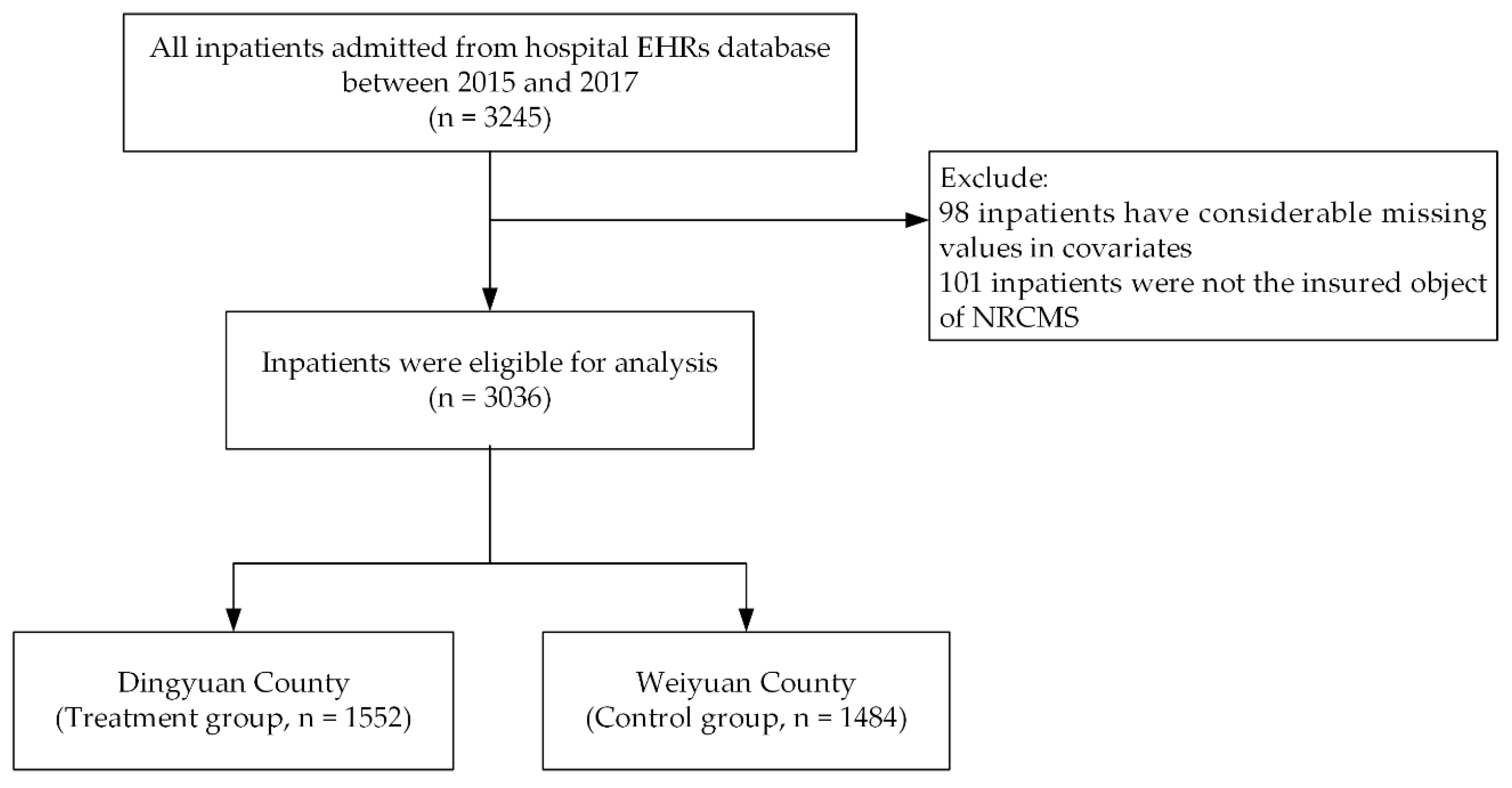
2.1. Data Source and Sampling
2.2. Outcome Variables
2.2.1. Behaviour of Inpatient Service Utilisation
2.2.2. Appropriateness of Inpatient Service Utilisation
2.3. Statistical Analysis
2.3.1. Interrupted Time Series Analysis
2.3.2. Propensity Score Matching
3. Results
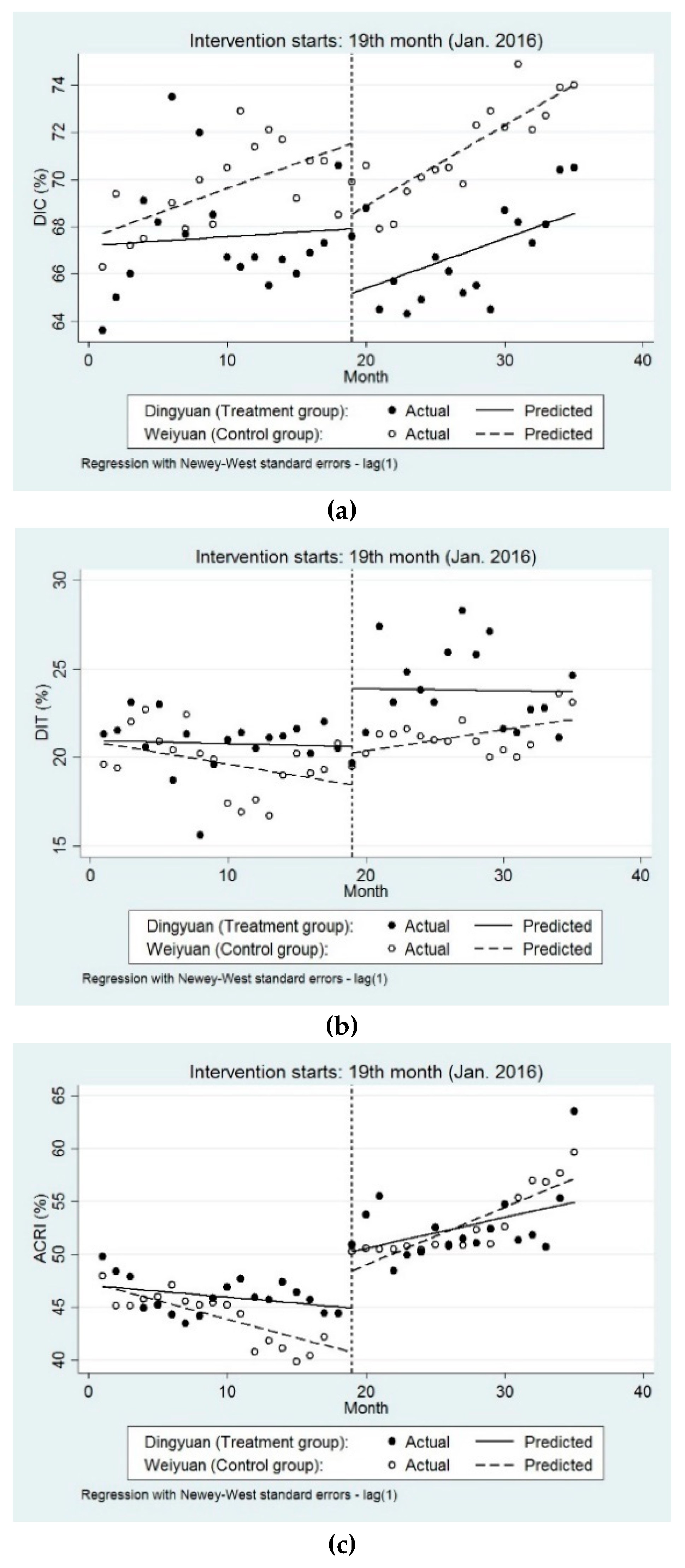
3.1. ITSA on the Behaviour of Inpatient Service Utilisation Before and After Reform
3.2. ITSA on the Differences in Behaviour of Inpatient Service Utilisation Between Groups
3.3. Characteristics of Our Study Sample for PSM Method
3.4. Balance Test and Matching Results from Three Matching Methods
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| NRCMS | new rural cooperative medical scheme |
| EHRs | electronic health records |
| ITSA | interrupted time-series analysis |
| PSM | Propensity score matching |
| DIC | distribution of inpatients in county hospitals |
| DIT | distribution of inpatients in township hospitals |
| ARCI | actual compensation ratio of inpatients |
| AA | appropriateness of admission |
| AD | appropriateness of disease |
| OOP | out-of-pocket |
| DRGs | diagnosis related groups |
| AEP | appropriateness evaluation protocol |
| GLS | generalised least-squares |
| DW | Durbin–Watson |
| AR | autorelated |
| RCTs | randomized controlled trials |
| ATT | average treatment effect on the treated |
| TX | Texas |
| USA | United States of America |
| CI | confidence interval |
| UK | United Kingdom |
References
- Bauhoff, S.; Hotchkiss, D.R.; Smith, O. The impact of medical insurance for the poor in Georgia: A regression discontinuity approach. Health Econ. 2011, 20, 1362–1378. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.T.; Hamid, F.; Pati, S.; Atun, R.; Millett, C. Impact of Noncommunicable Disease Multimorbidity on Healthcare Utilisation and Out-Of-Pocket Expenditures in Middle-Income Countries: Cross Sectional Analysis. PLoS ONE 2015, 10, e127199. [Google Scholar] [CrossRef]
- Ryu, H.; Young, W.B.; Park, C. Korean American health insurance and health services utilization. Res. Nurs. Health 2001, 24, 494–505. [Google Scholar] [CrossRef]
- Van der Wielen, N.; Channon, A.A.; Falkingham, J. Does insurance enrolment increase healthcare utilisation among rural-dwelling older adults? Evidence from the National Health Insurance Scheme in Ghana. BMJ Glob. Health 2018, 3, e590. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Gao, J.; Fox, A.; Rao, K.; Xu, K.; Xu, L.; Zhang, Y. Measuring the equity of inpatient utilization in Chinese rural areas. BMC Health Serv. Res. 2011, 11, 201. [Google Scholar] [CrossRef] [PubMed]
- Kawabuchi, K. Payment systems and considerations of case mix--are diagnosis-related groups applicable in Japan? Pharmacoeconomics 2000, 18 (Suppl. 1), 95–110. [Google Scholar] [CrossRef]
- National Health and Family Planning Commission of the People’s Republic of China. 2013 An Analysis Report of National Health Services Survey in China; Peking Union Medical College Press: Beijing, China, 2013. [Google Scholar]
- National Health and Family Planning Commission of the People’s Republic of China. 2017 China Statistical Yearbook of Health and Family Planning; Peking Union Medical College Press: Beijing, China, 2017. [Google Scholar]
- Zhang, Y.; Niu, Y.; Zhang, L. Determinants of patient choice for hospital readmission after township hospitalisation: A population-based retrospective study in China. BMJ Open 2018, 8, e021516. [Google Scholar] [CrossRef] [PubMed]
- Long, Q.; Zhang, T.; Hemminki, E.; Tang, X.; Huang, K.; Xiao, S.; Tolhurst, R. Utilisation, contents and costs of prenatal care under a rural health insurance (New Co-operative Medical System) in rural China: Lessons from implementation. BMC Health Serv. Res. 2010, 10, 301. [Google Scholar] [CrossRef]
- Li, H.M.; Chen, Y.C.; Gao, H.X.; Zhang, Y.; Chen, L.; Chang, J.J.; Su, D.; Lei, S.H.; Jiang, D.; Hu, X.M. Effectiveness evaluation of quota payment for specific diseases under global budget: A typical provider payment system reform in rural China. BMC Health Serv. Res. 2018, 18, 635. [Google Scholar] [CrossRef]
- He, R.; Miao, Y.; Ye, T.; Zhang, Y.; Tang, W.; Li, Z.; Zhang, L. The effects of global budget on cost control and readmission in rural China: A difference-in-difference analysis. J. Med. Econ. 2017, 20, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Si, L.; Jiang, Q.C. Challenges to the Chinese health insurance system: users’ and service providers’ perspectives. Chin. Med. J. 2015, 128, 571–573. [Google Scholar] [CrossRef]
- Quentin, W.; Scheller-Kreinsen, D.; Blumel, M.; Geissler, A.; Busse, R. Hospital payment based on diagnosis-related groups differs in Europe and holds lessons for the United States. Health Aff. 2013, 32, 713–723. [Google Scholar] [CrossRef] [PubMed]
- Abraham, J.M.; Karaca-Mandic, P.; Boudreaux, M. Sizing up the individual market for health insurance: A comparison of survey and administrative data sources. Med. Care Res. Rev. 2013, 70, 418–433. [Google Scholar] [CrossRef] [PubMed]
- Cantor, J.C.; Monheit, A.C.; DeLia, D.; Lloyd, K. Early impact of the Affordable Care Act on health insurance coverage of young adults. Health Serv. Res. 2012, 47, 1773–1790. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, Y.; Zhang, X.; Zhang, L. Current level and determinants of inappropriate admissions to township hospitals under the new rural cooperative medical system in China: A cross-sectional study. BMC Health Serv. Res. 2014, 14, 649. [Google Scholar] [CrossRef] [PubMed]
- Fretheim, A.; Soumerai, S.B.; Zhang, F.; Oxman, A.D.; Ross-Degnan, D. Interrupted time-series analysis yielded an effect estimate concordant with the cluster-randomized controlled trial result. J. Clin. Epidemiol. 2013, 66, 883–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buczak-Stec, E.; Gorynski, P.; Nitsch-Osuch, A.; Kanecki, K.; Tyszko, P. The impact of introducing a new hospital financing system (DRGs) in Poland on hospitalisations for atherosclerosis: An interrupted time series analysis (2004–2012). Health Policy 2017, 121, 1186–1193. [Google Scholar] [CrossRef]
- Bernal, J.L.; Cummins, S.; Gasparrini, A. Interrupted time series regression for the evaluation of public health interventions: A tutorial. Int. J. Epidemiol. 2017, 46, 348–355. [Google Scholar]
- Serumaga, B.; Ross-Degnan, D.; Avery, A.J.; Elliott, R.A.; Majumdar, S.R.; Zhang, F.; Soumerai, S.B. Effect of pay for performance on the management and outcomes of hypertension in the United Kingdom: Interrupted time series study. BMJ 2011, 342, d108. [Google Scholar] [CrossRef]
- Penfold, R.B.; Zhang, F. Use of interrupted time series analysis in evaluating health care quality improvements. Acad. Pediatr. 2013, 13, S38–S44. [Google Scholar] [CrossRef] [PubMed]
- McLean, A.; Wai, H.P.; Thu, A.M.; Khant, Z.S.; Indrasuta, C.; Ashley, E.A.; Kyaw, T.T.; Day, N.; Dondorp, A.; White, N.J.; et al. Malaria elimination in remote communities requires integration of malaria control activities into general health care: An observational study and interrupted time series analysis in Myanmar. BMC Med. 2018, 16, 183. [Google Scholar] [CrossRef]
- Cheng, L.; Liu, H.; Zhang, Y.; Shen, K.; Zeng, Y. The impact of health insurance on health outcomes and spending of the elderly: Evidence from China’s New Cooperative Medical Scheme. Health Econ. 2015, 24, 672–691. [Google Scholar] [CrossRef]
- Lei, X.; Lin, W. The New Cooperative Medical Scheme in rural China: Does more coverage mean more service and better health? Health Econ. 2009, 18 (Suppl. 2), S25–S46. [Google Scholar] [CrossRef]
- Hu, Y.; van Lenthe, F.J.; Hoffmann, R.; van Hedel, K.; Mackenbach, J.P. Assessing the impact of natural policy experiments on socioeconomic inequalities in health: How to apply commonly used quantitative analytical methods? BMC Med. Res. Methodol. 2017, 17, 68. [Google Scholar] [CrossRef] [PubMed]
- Baser, O. Too much ado about propensity score models? Comparing methods of propensity score matching. Value Health 2006, 9, 377–385. [Google Scholar] [CrossRef]
- Li, H.; Chen, Y.; Gao, H.; Zhang, Y.; Su, D.; Chang, J.; Jiang, D.; Hu, X.; Lei, S. Changes in inpatients’ distribution and benefits under institution level-based quota payment for specific diseases in rural China: An interrupted time-series analysis. Int. J. Health Plan. Manag. 2019, 34, e436–e446. [Google Scholar] [CrossRef]
- Yu, J.; Qiu, Y.; He, Z. Is universal and uniform health insurance better for China? Evidence from the perspective of supply-induced demand. Health Econ. Policy Law 2018, 1–16. [Google Scholar] [CrossRef]
- Wachter, R.M.; Katz, P.; Showstack, J.; Bindman, A.B.; Goldman, L. Reorganizing an academic medical service—Impact on cost, quality, patient satisfaction, and education. JAMA J. Am. Med. Assoc. 1998, 279, 1560–1565. [Google Scholar] [CrossRef]
- Brown, P.H.; Theoharides, C. Health-seeking behavior and hospital choice in China’s New Cooperative Medical System. Health Econ. 2009, 18 (Suppl. 2), S47–S64. [Google Scholar] [CrossRef] [PubMed]
- Yu, N.N.; Zhu, X. Affordable care encourages healthy living: Theory and evidence from China’s new cooperative medical scheme. Health Econ. 2018, 27, 2051–2066. [Google Scholar] [CrossRef] [PubMed]
- Beringer, T.; Flanagan, P. Acute medical bed usage by nursing-home residents. Ulst. Med. J. 1999, 68, 27. [Google Scholar] [CrossRef]
- Tsang, P.; Severs, M.P. A study of appropriateness of acute geriatric admissions and an assessment of the Appropriateness Evaluation Protocol. J. R. Coll. Physicians Lond. 1995, 29, 311–314. [Google Scholar] [PubMed]
- Panis, L.J.; Verheggen, F.W.; Pop, P. To stay or not to stay. The assessment of appropriate hospital stay: A Dutch report. Int. J. Qual. Health Care 2020, 14, 55–67. [Google Scholar] [CrossRef]
- Restuccia, J.; Shwartz, M.; Ash, A.; Payne, S. High hospital admission rates and inappropriate care. Health Aff. 1996, 15, 156–163. [Google Scholar] [CrossRef]
- Hammond, C.L.; Pinnington, L.L.; Phillips, M.F. A qualitative examination of inappropriate hospital admissions and lengths of stay. BMC Health Serv. Res. 2009, 9, 44. [Google Scholar] [CrossRef]
- De Cruppe, W.; Geraedts, M. Hospital choice in Germany from the patient’s perspective: A cross-sectional study. BMC Health Serv. Res. 2017, 17, 720. [Google Scholar] [CrossRef]
- Li, C.; Hou, Y.; Sun, M.; Lu, J.; Wang, Y.; Li, X.; Chang, F.; Hao, M. An evaluation of China’s new rural cooperative medical system: Achievements and inadequacies from policy goals. BMC Public Health 2015, 15, 1079. [Google Scholar] [CrossRef] [PubMed]
- Su, D.; Chen, Y.; Gao, H.; Li, H.; Chang, J.; Jiang, D.; Hu, X.; Lei, S.; Tan, M.; Chen, Z. Effect of integrated urban and rural residents medical insurance on the utilisation of medical services by residents in China: A propensity score matching with difference-in-differences regression approach. BMJ Open 2019, 9, e26408. [Google Scholar] [CrossRef]
- Silvestre, A.L.; Sue, V.M.; Allen, J.Y. If you build it, will they come? The Kaiser Permanente model of online health care. Health Aff. 2009, 28, 334–344. [Google Scholar] [CrossRef]
- Louis, D.Z.; Yuen, E.J.; Braga, M.; Cicchetti, A.; Rabinowitz, C.; Laine, C.; Gonnella, J.S. Impact of a DRG-based hospital financing system on quality and outcomes of care in Italy. Health Serv. Res. 1999, 34, 405–415. [Google Scholar]
- Scheller-Kreinsen, D.; Quentin, W.; Busse, R. DRG-based hospital payment systems and technological innovation in 12 European countries. Value Health 2011, 14, 1166–1172. [Google Scholar] [CrossRef] [PubMed]
- Bystrov, V.; Staszewska-Bystrova, A.; Rutkowski, D.; Hermanowski, T. Effects of DRG-based hospital payment in Poland on treatment of patients with stroke. Health Policy 2015, 119, 1119–1125. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Yang, J.; Wu, Y.; Pan, Z.; He, X.; Li, B.; Zhang, L. Challenges for the surgical capacity building of township hospitals among the Central China: A retrospective study. Int. J. Equity Health 2018, 17, 55. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Huining County | Dingyuan County |
|---|---|---|
| Population (thousands) | 576 | 982 |
| Area (square kilometres) | 6439 | 2998 |
| GDP (million) | 6276 | 18,337 |
| Per capita disposable income of urban residents throughout the year (RMB) | 17,123 | 23,180 |
| No. of county-level and township-level hospitals | 37 | 31 |
| No. of open beds per thousand people | 3.58 | 2.88 |
| No. of professional physicians per thousand people | 4.27 | 3.37 |
| GDP, Gross Domestic Product. RMB, ren min bi. | ||
| County | Dingyuan | Weiyuan |
|---|---|---|
| Payment type | Global budget (capitation prepayment); Payment for single disease (quota standard) | Global budget (specific diseases); Payment for single disease (quota standard) |
| Appropriateness treatment of disease range | 150 + N in county hospitals, 50 + N in township hospitals | 170 in county hospitals, 60 in central township hospitals 50 in general township hospitals |
| quota standard | Average cost in the past three years | Average cost in the past three years |
| Principle of cost reimbursement | 85% for county hospitals (quota standard) 90% for township hospitals (quota standard) | If actual cost < quota standard, 70% for county hospitals (autual cost) 80% for township hospitals (autual cost); If actual cost > quota standard, 70% for county hospitals (quota standard) 80% for township hospitals (quota standard) |
| Single payment limitation | - | 15,000 RMB for county hospitals 3,000 RMB for township hospitals |
| Annual Payment Limitation | 200,000 RMB | 80,000 RMB |
| Variables | DIC (%) | DIT (%) | ACRI (%) | |||
|---|---|---|---|---|---|---|
| Dingyuan | Weiyuan | Dingyuan | Weiyuan | Dingyuan | Weiyuan | |
| Single group | ||||||
| Preintervention trend | 0.04 (−0.23 to 0.30) | 0.21 ** (0.07 to 0.36) | −0.02 (−0.29 to 0.03) | −0.13 (−0.29 to 0.03) | −0.11 (−0.30 to 0.07) | −0.35 ** (−0.53 to −0.16) |
| Level change | −2.83 (−5.95 to 0.30) | −2.30 (−4.77 to 0.15) | 3.27 * (0.31 to 6.24) | 1.81 (−0.37 to 4.00) | 5.34 ** (0.31 to 6.24) | 7.72 *** (5.00 to 10.43) |
| Trend change | 0.18 (−0.19 to 0.56) | −0.02 (−0.24 to 0.21) | 0.01 (−0.29 to 0.30) | 0.24 * (0.04 to 0.45) | 0.40 (−0.10 to 0.91) | 0.89 *** (0.60 to 1.19) |
| Two groups comparison | ||||||
| Level difference prior to intervention | −0.48 (−3.70 to 2.75) | 0.14 (−2.01 to 2.30) | −0.61 (−2.68 to 2.56) | |||
| Slope difference prior to intervention | −0.17 (−0.47 to 0.12) | 0.11 (−0.08 to 0.30) | 0.23 (−0.02 to 0.50) | |||
| Level difference in the period immediately following intervention | 0.26 (−3.64 to 4.17) | 1.46 (−2.15 to 5.07) | −2.37 (−6.91 to 2.17) | |||
| Slope difference after intervention compared with preintervention | 0.04 (−0.36 to 0.45) | −0.24 (−0.59 to 0.11) | −0.49 (−1.06 to 0.09) | |||
| Variable | Dingyuan (N = 1552) | Weiyuan (N = 1486) | ||
|---|---|---|---|---|
| Mean | SD | Mean | SD | |
| AA | 1.44 | 0.50 | 1.45 | 0.50 |
| AD | 1.29 | 0.45 | 1.07 | 0.26 |
| Hospital level | 1.57 | 0.50 | 1.44 | 0.50 |
| Gender | 1.47 | 0.50 | 1.56 | 0.50 |
| Age | 56.20 | 22.46 | 45.81 | 20.96 |
| Occupation | 5.01 | 0.20 | 5.14 | 0.75 |
| Marital status | 1.85 | 0.37 | 1.83 | 0.45 |
| Admission department | 1.58 | 0.87 | 1.26 | 0.76 |
| Admission route | 1.30 | 0.46 | 1.30 | 0.46 |
| Length of stay | 6.11 | 4.68 | 6.19 | 1.86 |
| Admission status | 1.31 | 0.55 | 1.58 | 0.51 |
| Health status | 1.34 | 0.63 | 1.69 | 0.51 |
| History of disease | 0.46 | 0.50 | 0.19 | 0.39 |
| Chronic | 0.40 | 0.49 | 0.14 | 0.34 |
| History of surgery | 0.05 | 0.21 | 0.01 | 0.10 |
| Sample | Overall Balance | Matching Results | Bootstrap Results | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pseudo R2 | LR chi2 | P > chi2 | Mean Bias | Median Bias | ATT | S.E. | T-stat | S.E. | z-Value | p-Value | 95%CI (lower, upper) | |
| AA | ||||||||||||
| Raw sample before matching | 0.275 | 1321.76 | 0.000 | 32.2 | 25.7 | −0.01 | 0.02 | −0.68 | ||||
| kernel matching | 0.003 | 16.50 | 0.927 | 2.8 | 2.0 | −0.03 | 0.03 | −2.05 | 0.03 | −2.42 | 0.042 | −0.08 to 0.02 |
| k-nearest neighbor matching (k = 1) | 0.004 | 22.07 | 0.896 | 3.7 | 2.8 | −0.04 | 0.03 | −2.18 | 0.04 | −2.62 | 0.038 | −0.11 to 0.03 |
| local linear regression matching | 0.006 | 19.16 | 0.919 | 3.3 | 2.6 | −0.02 | 0.03 | −1.59 | 0.04 | −1.77 | 0.073 | −0.07 to 0.02 |
| AD | ||||||||||||
| Raw sample before matching | 0.233 | 879.57 | 0.000 | 30.2 | 21.3 | 0.22 | 0.01 | 16.57 | ||||
| kernel matching | 0.003 | 3.42 | 0.943 | 2.2 | 1.4 | 0.19 | 0.03 | 13.87 | 0.02 | 14.28 | 0.000 | 0.17 to 0.25 |
| k-nearest neighbor matching (k = 1) | 0.012 | 4.06 | 0.933 | 2.9 | 2.1 | 0.17 | 0.05 | 11.15 | 0.04 | 11.56 | 0.000 | 0.15 to 0.19 |
| local linear regression matching | 0.019 | 12.79 | 0.712 | 5.4 | 5.6 | 0.16 | 0.02 | 11.00 | 0.02 | 11.48 | 0.000 | 0.14 to 0.20 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, D.; Chen, Y.; Gao, H.; Li, H.; Chang, J.; Lei, S.; Jiang, D.; Hu, X.; Tan, M.; Chen, Z. Is There a Difference in the Utilisation of Inpatient Services Between Two Typical Payment Methods of Health Insurance? Evidence from the New Rural Cooperative Medical Scheme in China. Int. J. Environ. Res. Public Health 2019, 16, 1410. https://doi.org/10.3390/ijerph16081410
Su D, Chen Y, Gao H, Li H, Chang J, Lei S, Jiang D, Hu X, Tan M, Chen Z. Is There a Difference in the Utilisation of Inpatient Services Between Two Typical Payment Methods of Health Insurance? Evidence from the New Rural Cooperative Medical Scheme in China. International Journal of Environmental Research and Public Health. 2019; 16(8):1410. https://doi.org/10.3390/ijerph16081410
Chicago/Turabian StyleSu, Dai, Yingchun Chen, Hongxia Gao, Haomiao Li, Jingjing Chang, Shihan Lei, Di Jiang, Xiaomei Hu, Min Tan, and Zhifang Chen. 2019. "Is There a Difference in the Utilisation of Inpatient Services Between Two Typical Payment Methods of Health Insurance? Evidence from the New Rural Cooperative Medical Scheme in China" International Journal of Environmental Research and Public Health 16, no. 8: 1410. https://doi.org/10.3390/ijerph16081410
APA StyleSu, D., Chen, Y., Gao, H., Li, H., Chang, J., Lei, S., Jiang, D., Hu, X., Tan, M., & Chen, Z. (2019). Is There a Difference in the Utilisation of Inpatient Services Between Two Typical Payment Methods of Health Insurance? Evidence from the New Rural Cooperative Medical Scheme in China. International Journal of Environmental Research and Public Health, 16(8), 1410. https://doi.org/10.3390/ijerph16081410