Greenness Availability and Respiratory Health in a Population of Urbanised Children in North-Western Italy

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Population and Ethic Committee Approval
2.2. Questionnaire
2.3. Spirometry
2.4. Biological Analyses Cotinine and Creatinine
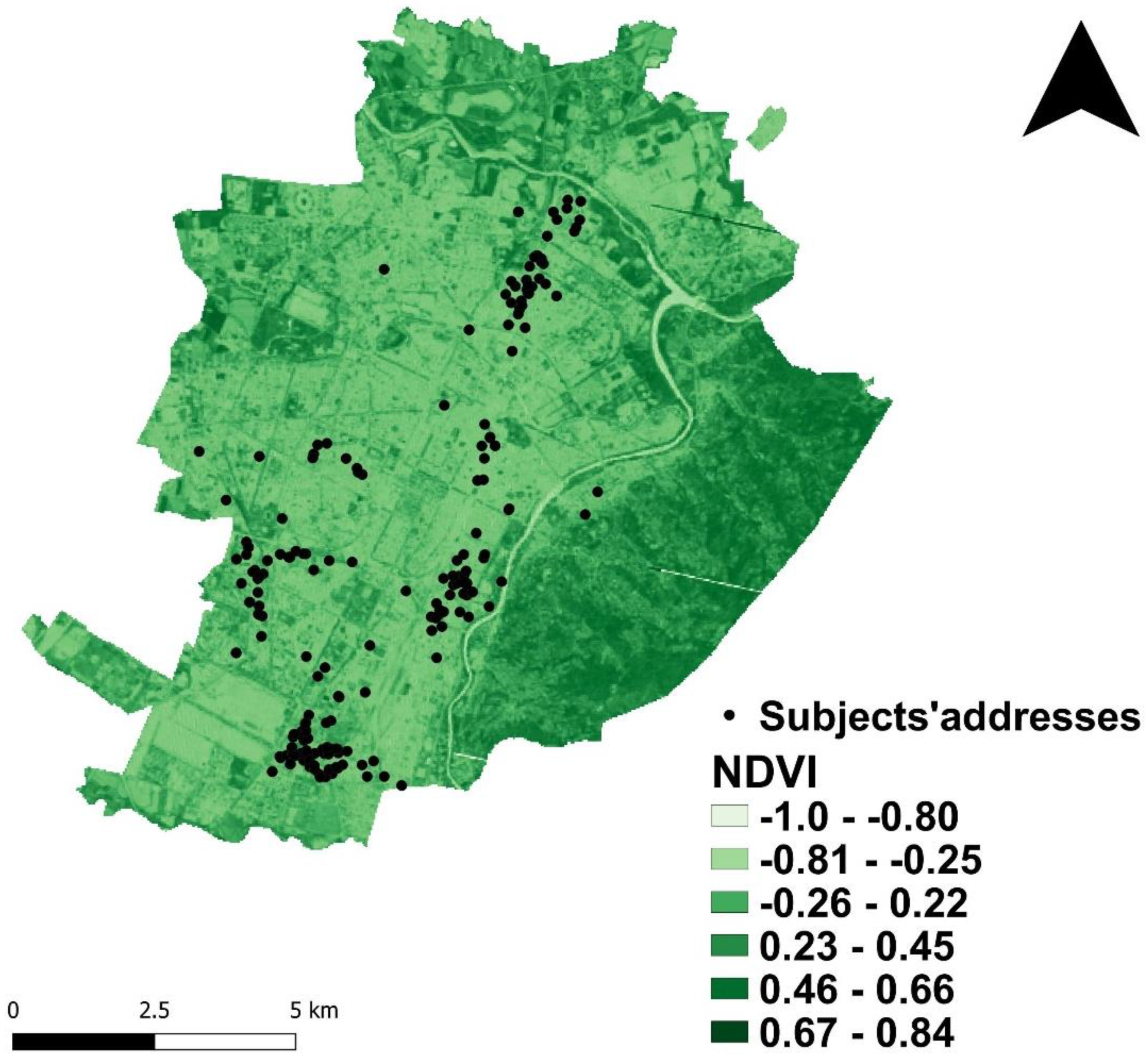
2.5. Green Exposure Assessment
2.6. Other Variables
2.7. Statistical Analyses
3. Results
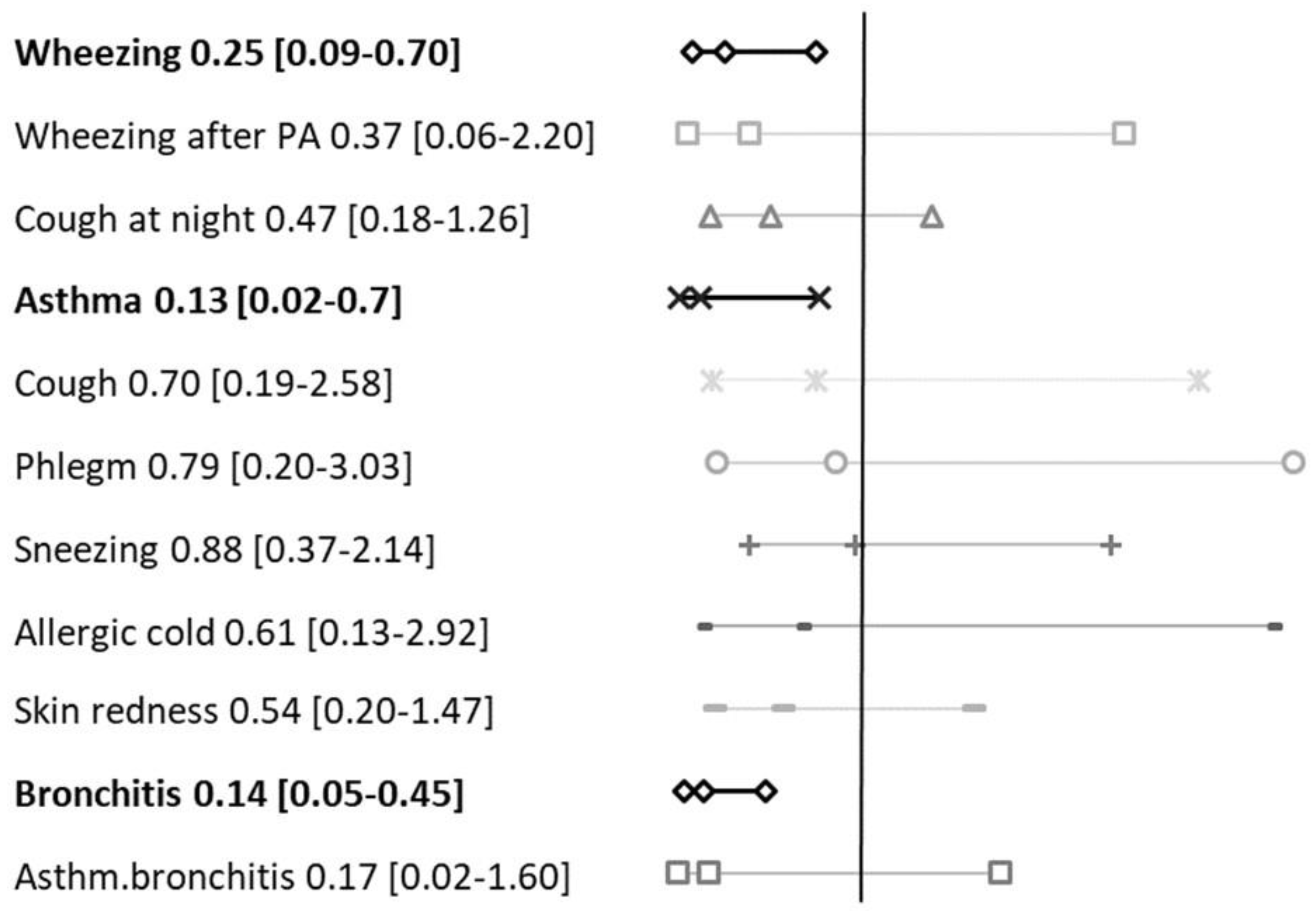
3.1. Respiratory Symptoms and Greenness
3.2. Respiratory Flows and Greenness
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Asher, I.; Pearce, N. Global burden of asthma among children. Int. J. Tuberc. Lung Dis. 2014, 18, 1269–1278. [Google Scholar] [CrossRef]
- Ferrante, G.; La Grutta, S. The Burden of Pediatric Asthma. Front. Pediatr. 2018, 6, 186. [Google Scholar] [CrossRef] [Green Version]
- Tischer, C.; Gascon, M.; Fernández-Somoano, A.; Tardón, A.; Lertxundi Materola, A.; Ibarluzea, J.; Ferrero, A.; Estarlich, M.; Cirach, M.; Vrijheid, M.; et al. Urban green and grey space in relation to respiratory health in children. Eur. Respir. J. 2017, 49, 1502112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Marco, R.; Cappa, V.; Accordini, S.; Rava, M.; Antonicelli, L.; Bortolami, O.; Braggion, M.; Bugiani, M.; Casali, L.; Cazzoletti, L.; et al. Trends in the prevalence of asthma and allergic rhinitis in Italy between 1991 and 2010. Eur. Respir. J. 2012, 39, 883–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asher, M.I.; Montefort, S.; Björkstén, B.; Lai, C.K.; Strachan, D.P.; Weiland, S.K.; Williams, H.; ISAAC Phase Three Study Group. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys. Lancet 2006, 368, 733–743. [Google Scholar] [CrossRef]
- Pearce, N.; Ait-Khaled, N.; Beasley, R.; Mallol, J.; Keil, U.; Mitchell, E.; Robertson, C. Worldwide trends in the prevalence of asthma symptoms: Phase III of the International Study of Asthma and Allergies in Childhood (ISAAC). Thorax 2007, 62, 758–766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stocks, J.; Sonnappa, S.; Lum, S. Lung function testing in children: Importance of race and ethnic-specific reference equations. Expert Rev. Respir. Med. 2014, 8, 527–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bui, D.S.; Burgess, J.A.; Lowe, A.J.; Perret, J.L.; Lodge, C.J.; Bui, M.; Morrison, S.; Thompson, B.R.; Thomas, P.S.; Giles, G.G.; et al. Childhood Lung Function Predicts Adult Chronic Obstructive Pulmonary Disease and Asthma–Chronic Obstructive Pulmonary Disease Overlap Syndrome. Am. J. Respir. Crit. Care Med. 2017, 196, 39–46. [Google Scholar] [CrossRef]
- Asif, M.; Mustafa, G.; Aslam, M.; Altaf, S. Predictors of pulmonary function test values for Pakistani children, aged 5–14 years. J. Pak. Med. Assoc. 2017, 67, 1323–1326. [Google Scholar]
- Sly, P.D.; Carpenter, D.O.; Van den Berg, M.; Stein, R.T.; Landrigan, P.J.; Brune-Drisse, M.-N.; Suk, W. Health Consequences of Environmental Exposures: Causal Thinking in Global Environmental Epidemiology. Ann. Glob. Health 2016, 82, 3. [Google Scholar] [CrossRef]
- Galassi, C.; De Sario, M.; Biggeri, A.; Bisanti, L.; Chellini, E.; Ciccone, G.; Petronio, M.G.; Piffer, S.; Sestini, P.; Rusconi, F.; et al. Changes in Prevalence of Asthma and Allergies Among Children and Adolescents in Italy: 1994–2002. Pediatrics 2006, 117, 34–42. [Google Scholar] [CrossRef] [PubMed]
- James, P.; Banay, R.F.; Hart, J.E.; Laden, F. A Review of the Health Benefits of Greenness. Curr. Epidemiol. Rep. 2015, 2, 131–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fong, K.C.; Hart, J.E.; James, P. A Review of Epidemiologic Studies on Greenness and Health: Updated Literature Through 2017. Curr. Environ. Health Rep. 2018, 5, 77–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franchini, M.; Mannucci, P.M. Mitigation of air pollution by greenness: A narrative review. Eur. J. Intern. Med. 2018, 55, 1–5. [Google Scholar] [CrossRef] [PubMed]
- van Dorn, A. Urban planning and respiratory health. Lancet Respir. Med. 2017, 5, 781–782. [Google Scholar] [CrossRef]
- Lambert, K.A.; Lodge, C.; Lowe, A.J.; Prendergast, L.A.; Thomas, P.S.; Bennett, C.M.; Abramson, M.J.; Dharmage, S.C.; Erbas, B. Pollen exposure at birth and adolescent lung function, and modification by residential greenness. Allergy 2019, 74, 1977–1984. [Google Scholar] [CrossRef]
- Gehring, U.; Gruzieva, O.; Agius, R.M.; Beelen, R.; Custovic, A.; Cyrys, J.; Eeftens, M.; Flexeder, C.; Fuertes, E.; Heinrich, J.; et al. Air Pollution Exposure and Lung Function in Children: The ESCAPE Project. Environ. Health Perspect. 2013, 121, 1357–1364. [Google Scholar] [CrossRef] [Green Version]
- Götschi, T.; Heinrich, J.; Sunyer, J.; Künzli, N. Long-Term Effects of Ambient Air Pollution on Lung Function. Epidemiology 2008, 19, 690–701. [Google Scholar] [CrossRef] [Green Version]
- Lambert, K.A.; Bowatte, G.; Tham, R.; Lodge, C.; Prendergast, L.; Heinrich, J.; Abramson, M.J.; Dharmage, S.C.; Erbas, B. Residential greenness and allergic respiratory diseases in children and adolescents—A systematic review and meta-analysis. Environ. Res. 2017, 159, 212–221. [Google Scholar] [CrossRef]
- Lambert, K.; Bowatte, G.; Tham, R.; Lodge, C.; Prendergast, L.; Heinrich, J.; Abramson, M.; Dharmage, S.; Erbas, B. Greenspace and Atopic Sensitization in Children and Adolescents—A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 2539. [Google Scholar] [CrossRef] [Green Version]
- Fong, K.; Kloog, I.; Coull, B.; Koutrakis, P.; Laden, F.; Schwartz, J.; James, P. Residential Greenness and Birthweight in the State of Massachusetts, USA. Int. J. Environ. Res. Public Health 2018, 15, 1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrusaityte, S.; Grazuleviciene, R.; Kudzyte, J.; Bernotiene, A.; Dedele, A.; Nieuwenhuijsen, M.J. Associations between neighbourhood greenness and asthma in preschool children in Kaunas, Lithuania: A case-control study. BMJ Open 2016, 6, e010341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lovasi, G.S.; O’Neil-Dunne, J.P.M.; Lu, J.W.T.; Sheehan, D.; Perzanowski, M.S.; MacFaden, S.W.; King, K.L.; Matte, T.; Miller, R.L.; Hoepner, L.A.; et al. Urban Tree Canopy and Asthma, Wheeze, Rhinitis, and Allergic Sensitization to Tree Pollen in a New York City Birth Cohort. Environ. Health Perspect. 2013, 121, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Bono, R.; Romanazzi, V.; Bellisario, V.; Tassinari, R.; Trucco, G.; Urbino, A.; Cassardo, C.; Siniscalco, C.; Marchetti, P.; Marcon, A. Air pollution, aeroallergens and admissions to pediatric emergency room for respiratory reasons in Turin, northwestern Italy. BMC Public Health 2016, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dadvand, P.; Villanueva, C.M.; Font-Ribera, L.; Martinez, D.; Basagaña, X.; Belmonte, J.; Vrijheid, M.; Gražulevičienė, R.; Kogevinas, M.; Nieuwenhuijsen, M.J. Risks and Benefits of Green Spaces for Children: A Cross-Sectional Study of Associations with Sedentary Behavior, Obesity, Asthma, and Allergy. Environ. Health Perspect. 2014, 122, 1329–1335. [Google Scholar] [CrossRef]
- Parmes, E.; Pesce, G.; Sabel, C.E.; Baldacci, S.; Bono, R.; Brescianini, S.; D’Ippolito, C.; Hanke, W.; Horvat, M.; Liedes, H.; et al. Influence of residential land cover on childhood allergic and respiratory symptoms and diseases: Evidence from 9 European cohorts. Environ. Res. 2019, 108953. [Google Scholar] [CrossRef]
- Fuertes, E.; Markevych, I.; Bowatte, G.; Gruzieva, O.; Gehring, U.; Becker, A.; Berdel, D.; von Berg, A.; Bergström, A.; Brauer, M.; et al. Residential greenness is differentially associated with childhood allergic rhinitis and aeroallergen sensitization in seven birth cohorts. Allergy 2016, 71, 1461–1471. [Google Scholar] [CrossRef] [Green Version]
- Eldeirawi, K.; Kunzweiler, C.; Zenk, S.; Finn, P.; Nyenhuis, S.; Rosenberg, N.; Persky, V. Associations of urban greenness with asthma and respiratory symptoms in Mexican American children. Ann. Allergy Asthma Immunol. 2019, 122, 289–295. [Google Scholar] [CrossRef]
- Lovasi, G.S.; Quinn, J.W.; Neckerman, K.M.; Perzanowski, M.S.; Rundle, A. Children living in areas with more street trees have lower prevalence of asthma. J. Epidemiol. Community Health 2008, 62, 647–649. [Google Scholar] [CrossRef] [Green Version]
- Sbihi, H.; Tamburic, L.; Koehoorn, M.; Brauer, M. Greenness and Incident Childhood Asthma: A 10-Year Follow-up in a Population-based Birth Cohort. Am. J. Respir. Crit. Care Med. 2015, 192, 1131–1133. [Google Scholar] [CrossRef]
- Hsieh, C.-J.; Yu, P.-Y.; Tai, C.-J.; Jan, R.-H.; Wen, T.-H.; Lin, S.-W.; Tseng, C.-C. Association between the First Occurrence of Asthma and Residential Greenness in Children and Teenagers in Taiwan. Int. J. Environ. Res. Public Health 2019, 16, 2076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilat, M.A.; McFarland, A.; Snelgrove, A.; Collins, K.; Waliczek, T.M.; Zajicek, J. The Effect of Tree Cover and Vegetation on Incidence of Childhood Asthma in Metropolitan Statistical Areas of Texas. Horttechnology 2012, 22, 631–637. [Google Scholar] [CrossRef] [Green Version]
- Marchetti, P.; Pesce, G.; Villani, S.; Antonicelli, L.; Ariano, R.; Attena, F.; Bono, R.; Bellisario, V.; Fois, A.; Gibelli, N.; et al. Pollen concentrations and prevalence of asthma and allergic rhinitis in Italy: Evidence from the GEIRD study. Sci. Total Environ. 2017, 584–585, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- Galassi, C.; Forastiere, F.; Biggeri, A.; Gabellini, C.; De Sario, M.; Ciccone, G.; Biocca, M.; Bisanti, L.; Gruppo Collaborativo SIDRIA-2. SIDRIA second phase: Objectives, study design and methods. Epidemiol. Prev. 2005, 29, 9–13. [Google Scholar]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Piccioni, P.; Tassinari, R.; Carosso, A.; Carena, C.; Bugiani, M.; Bono, R. Lung function changes from childhood to adolescence: A seven-year follow-up study. BMC Pulm. Med. 2015, 15, 31. [Google Scholar] [CrossRef] [Green Version]
- Squillacioti, G.; Bellisario, V.; Grignani, E.; Mengozzi, G.; Bardaglio, G.; Dalmasso, P.; Bono, R. The asti study: The induction of oxidative stress in a population of children according to their body composition and passive tobacco smoking exposure. Int. J. Environ. Res. Public Health 2019, 16, 490. [Google Scholar] [CrossRef] [Green Version]
- Alcaraz-Segura, D.; Cabello, J.; Paruelo, J. Baseline characterization of major Iberian vegetation types based on the NDVI dynamics. Plant Ecol. 2009, 202, 13–29. [Google Scholar] [CrossRef]
- Donovan, G.H.; Gatziolis, D.; Longley, I.; Douwes, J. Vegetation diversity protects against childhood asthma: Results from a large New Zealand birth cohort. Nat. Plants 2018, 4, 358–364. [Google Scholar] [CrossRef]
- Hanski, I.; von Hertzen, L.; Fyhrquist, N.; Koskinen, K.; Torppa, K.; Laatikainen, T.; Karisola, P.; Auvinen, P.; Paulin, L.; Makela, M.J.; et al. Environmental biodiversity, human microbiota, and allergy are interrelated. Proc. Natl. Acad. Sci. USA 2012, 109, 8334–8339. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Hart, J.; Coull, B.; Cao, S.; Spengler, J.; Adamkiewicz, G. Effect of Residential Greenness and Nearby Parks on Respiratory and Allergic Diseases among Middle School Adolescents in a Chinese City. Int. J. Environ. Res. Public Health 2019, 16, 991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartra, J.; Belmonte, J.; Torres-Rodriguez, J.M.; Cistero-Bahima, A. Sensitization to Alternaria in patients with respiratory allergy. Front. Biosci. 2009, 14, 3372–3379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DellaValle, C.T.; Triche, E.W.; Leaderer, B.P.; Bell, M.L. Effects of ambient pollen concentrations on frequency and severity of asthma symptoms among asthmatic children. Epidemiology 2012, 23, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corsini, E.; Sokooti, M.; Galli, C.L.; Moretto, A.; Colosio, C. Pesticide induced immunotoxicity in humans: A comprehensive review of the existing evidence. Toxicology 2013, 307, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Boeyen, J.; Callan, A.C.; Blake, D.; Wheeler, A.J.; Franklin, P.; Hall, G.L.; Shackleton, C.; Sly, P.D.; Hinwood, A. Investigating the relationship between environmental factors and respiratory health outcomes in school children using the forced oscillation technique. Int. J. Hyg. Environ. Health 2017, 220, 494–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellisario, V.; Piccioni, P.; Bugiani, M.; Squillacioti, G.; Levra, S.; Gulotta, C.; Mengozzi, G.; Perboni, A.; Grignani, E.; Bono, R. Tobacco Smoke Exposure, Urban and Environmental Factors as Respiratory Disease Predictors in Italian Adolescents. Int. J. Environ. Res. Public Health 2019, 16, 4048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuertes, E.; Markevych, I.; Berg, V. Greenness and allergies: Evidence of differential associations in two areas in Germany. J. Epihdemiol. Community Health 2014, 68, 787–790. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sex n (%) | Female 79 (42) | Male 108 (58) | p-Value | All n = 187 |
|---|---|---|---|---|
| Age (yrs) | 11.5 ± 0.7 | 11.6 ± 0.9 | 0.465 | 11.5 ± 0.8 |
| BMI (kg/m2) | 18.6 ± 3.2 | 19.7 ± 3.8 | 0.095 | 19.3 ± 3.6 |
| Weight (kg) | 41.6 ± 9.7 | 45.3 ± 11.9 | 0.077 | 43.8 ± 11.2 |
| Height (cm) | 148.8 ± 8.5 | 150.8 ± 9.4 | 0.205 | 150 ± 9.1 |
| Passive cigarettes (n/day) | 5.1 ± 1.2 | 4.8 ± 1.3 | 0.266 | 4.9 ±1.3 |
| Cotinine (ng/mgCREA) | 0.38 ± 1.5 | 0.36 ± 0.86 | 0.870 | 0.61 ± 0.59 |
| FEV1 (L) | 2.2 ± 0.4 | 2.4 ± 0.5 | <0.001 | 2.3 ± 0.5 |
| FVC (L) | 2.5 ± 0.5 | 2.9 ± 0.6 | <0.001 | 2.7 ± 0.6 |
| FEV1/FVC (%) | 86.1 ± 7.3 | 85.7 ± 5.7 | 0.085 | 85.9 ± 6.4 |
| FEF25 (L/sec) | 1.4 ± 0.5 | 1.6 ± 0.6 | 0.210 | 1.5 ± 0.6 |
| FEF25–75 (L/sec) | 2.5 ± 0.7 | 2.7 ± 0.8 | 0.201 | 2.6 ± 0.7 |
| FEF50 (L/sec) | 2.9 ± 0.8 | 3.1 ± 0.8 | 0.089 | 3.0 ± 0.8 |
| FEFmax (L/sec) | 4.3 ± 1.0 | 4.7 ± 1.0 | 0.010 | 4.5 ± 1.0 |
| PM10 (µg/m3) | 48.7 ± 6.5 | 48.9 ± 7.0 | 0.934 | 48.8 ± 6.8 |
| NO2 (µg/m3) | 55.8 ± 14.2 | 55.4 ± 14.8 | 0.934 | 55.6 ± 14.5 |
| NO (µg/m3) | 45.3 ± 15.1 | 45.5 ± 16.2 | 0.934 | 45.4 ± 15.7 |
| NDVI | 0.25 ± 0.07 | 0.26 ± 0.07 | 0.445 | 0.25 ± 0.07 |
| Variables | B | C.I. 95% | p-Value |
|---|---|---|---|
| Intercept | 2.11 | 1.32–2.90 | <0.001 |
| BMI | 0.01 | −0.02–0.04 | 0.370 |
| Age | 0.30 | 0.18–0.42 | <0.001 |
| Sex | 0.12 | −0.08–0.31 | 0.245 |
| PM10 | 0.01 | −0.01–0.03 | 0.073 |
| Cigarettes/day | −0.21 | −0.01–0.06 | 0.595 |
| NDVI 1st tertile | 0.06 | −0.19–0.30 | 0.640 |
| NDVI 2nd tertile | −2.40 | −0.48–0.01 | 0.049 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Squillacioti, G.; Bellisario, V.; Levra, S.; Piccioni, P.; Bono, R. Greenness Availability and Respiratory Health in a Population of Urbanised Children in North-Western Italy. Int. J. Environ. Res. Public Health 2020, 17, 108. https://doi.org/10.3390/ijerph17010108
Squillacioti G, Bellisario V, Levra S, Piccioni P, Bono R. Greenness Availability and Respiratory Health in a Population of Urbanised Children in North-Western Italy. International Journal of Environmental Research and Public Health. 2020; 17(1):108. https://doi.org/10.3390/ijerph17010108
Chicago/Turabian StyleSquillacioti, Giulia, Valeria Bellisario, Stefano Levra, Pavilio Piccioni, and Roberto Bono. 2020. "Greenness Availability and Respiratory Health in a Population of Urbanised Children in North-Western Italy" International Journal of Environmental Research and Public Health 17, no. 1: 108. https://doi.org/10.3390/ijerph17010108
APA StyleSquillacioti, G., Bellisario, V., Levra, S., Piccioni, P., & Bono, R. (2020). Greenness Availability and Respiratory Health in a Population of Urbanised Children in North-Western Italy. International Journal of Environmental Research and Public Health, 17(1), 108. https://doi.org/10.3390/ijerph17010108