Optimal Initial Blood Pressure in Intensive Care Unit Patients with Non-Traumatic Intracranial Hemorrhage

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population
2.3. Blood Pressure Data
2.4. Death Identification
2.5. Covariates
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Charidimou, A.; Morotti, A.; Valenti, R.; Giese, A.K.; Boulouis, G.; Pasi, M.; Roongpiboonsopit, D.; Lauer, A.; Xiong, L.; Van Harten, T.W.; et al. Journal Club: Time trends in incidence, case fatality, and mortality of intracerebral haemorrhage. Neurology 2016, 86, e206–e209. [Google Scholar] [CrossRef] [PubMed]
- Hemphill, J.C.; Greenberg, S.M.; Anderson, C.S.; Becker, K.; Bendok, B.R.; Cushman, M.; Fung, G.L.; Goldstein, J.N.; Macdonald, R.L.; Mitchell, P.H.; et al. Guidelines for the management of spontaneous intracerebral hemorrhage: A guideline for healthcare professionals From the American Heart Association/American Stroke Association. Stroke 2015, 46, 2032–2060. [Google Scholar] [CrossRef] [PubMed]
- Hemphill, J.C.; Bonovich, D.C.; Besmertis, L.; Manley, G.T.; Johnston, S.C. The ICH score: A simple, reliable grading scale for intracerebral haemorrhage. Stroke 2001, 32, 891–897. [Google Scholar] [CrossRef] [PubMed]
- Broderick, J.; Connolly, S.; Feldmann, E.; Hanley, D.; Kase, C.; Krieger, D.; Mayberg, M.; Morgenstern, L.; Ogilvy, C.S.; Vespa, P.; et al. Guidelines for the management of spontaneous intracerebral haemorrhage in adults: 2007 update: A guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group. Stroke 2007, 38, 2001–2023. [Google Scholar]
- Anderson, C.S.; Huang, Y.; Wang, J.G.; Arima, H.; Neal, B.; Peng, B.; Heeley, E.; Skulina, C.; Parsons, M.W.; Kim, J.S.; et al. Intensive blood pressure reduction in acute cerebral haemorrhage trial (INTERACT): A randomised pilot trial. Lancet. Neurol. 2001, 7, 391–399. [Google Scholar] [CrossRef]
- Takeda, R.; Ogura, T.; Ooigawa, H.; Fushihara, G.; Yoshikawa, S.; Okada, D.; Araki, R.; Kurita, H. A practical prediction model for early hematoma expansion in spontaneous deep ganglionic intracerebral haemorrhage. Clin. Neurol. Neurosurg. 2013, 115, 1028–1031. [Google Scholar] [CrossRef]
- Johnson, A.E.; Pollard, T.J.; Shen, L.; Lehman, L.W.; Feng, M.; Ghassemi, M.; Moody, B.; Szolovits, P.; Celi, L.A.; Mark, R.G. MIMIC-III, a freely accessible critical care database. Sci. Data 2016, 3, 160035. [Google Scholar] [CrossRef]
- Barrio, I.; Arostegui, I.; Quintana, J.M.; Group IC. Use of generalised additive models to categorise continuous variables in clinical prediction. BMC Med. Res. Methodol. 2013, 13, 83. [Google Scholar] [CrossRef]
- Anderson, C.S.; Huang, Y.; Arima, H.; Heeley, E.; Skulina, C.; Parsons, M.W.; Peng, B.; Li, Q.; Su, S.; Tao, Q.L.; et al. Effects of early intensive blood pressure-lowering treatment on the growth of hematoma and perihematomal edema in acute intracerebral haemorrhage: The Intensive Blood Pressure Reduction in Acute Cerebral Haemorrhage Trial (INTERACT). Stroke 2010, 41, 307–312. [Google Scholar] [CrossRef]
- Anderson, C.S.; Heeley, E.; Huang, Y.; Wang, J.; Stapf, C.; Delcourt, C.; Lindley, R.; Robinson, T.; Lavados, P.; Neal, B.; et al. Rapid blood-pressure lowering in patients with acute intracerebral haemorrhage. N. Engl. J. Med. 2013, 368, 2355–2365. [Google Scholar] [CrossRef]
- Heeley, E.; Anderson, C.S.; Woodward, M.; Arima, H.; Robinson, T.; Stapf, C.; Parsons, M.; Lavados, P.M.; Huang, Y.; Wang, Y.; et al. Poor utility of grading scales in acute intracerebral haemorrhage: Results from the INTERACT2 trial. Int. J. Stroke 2015, 10, 1101–1107. [Google Scholar] [CrossRef]
- Antihypertensive Treatment of Acute Cerebral Haemorrhage (ATACH) Investigators. Antihypertensive treatment of acute cerebral haemorrhage. Crit. Care Med. 2010, 38, 637–648. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, A.I. Antihypertensive treatment of acute cerebral haemorrhage (ATACH). Neurocrit. Care 2007, 6, 56. [Google Scholar] [CrossRef]
- Qureshi, A.; Palesch, Y. Antihypertensive treatment of acute cerebral haemorrhage (ATACH) II: Design, methods, and rationale. Neurocrit. Care 2011, 15, 559–576. [Google Scholar] [CrossRef]
- Alrahbi, S.; Alaraimi, R.; Alzaabi, A.; Gosselin, S. Intensive blood-pressure lowering in patients with acute cerebral haemorrhage. CJEM 2018, 20, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Li, H.; Lin, S.; Ma, J.; Guo, R.; Ma, L.; Fang, Y.; Tian, M.; Liu, M.; You, C. Perioperative antihypertensive treatment in patients with spontaneous intracerebral haemorrhage. Stroke 2017, 48, 216–218. [Google Scholar] [CrossRef]
- Qureshi, A.I.; Palesch, Y.Y.; Barsan, W.G.; Hanley, D.F.; Hsu, C.Y.; Martin, R.L.; Moy, C.S.; Silbergleit, R.; Steiner, T.; Suarez, J.I.; et al. Intensive blood-pressure lowering in patients with acute cerebral hemorrhage. N. Engl. J. Med. 2016, 375, 1033–1043. [Google Scholar] [CrossRef]
- Steiner, T.; Bösel, J. Options to restrict hematoma expansion after spontaneous intracerebral haemorrhage. Stroke 2010, 41, 402–409. [Google Scholar] [CrossRef]
- Rodriguez-Luna, D.; Piñeiro, S.; Rubiera, M.; Ribo, M.; Coscojuela, P.; Pagola, J.; Flores, A.; Muchada, M.; Ibarra, B.; Meler, P.; et al. Impact of blood pressure changes and course on hematoma growth in acute intracerebral haemorrhage. Eur. J. Neurol. 2013, 20, 1277–1283. [Google Scholar] [CrossRef]
- Arima, H.; Heeley, E.; Delcourt, C.; Hirakawa, Y.; Wang, X.; Woodward, M.; Robinson, T.; Stapf, C.; Parsons, M.; Lavados, P.M.; et al. INTERACT2 Investigators Optimal achieved blood pressure in acute intracerebral haemorrhage: INTERACT2. Neurology 2015, 84, 464–471. [Google Scholar] [CrossRef]
- Koch, S.; Romano, J.G.; Forteza, A.M.; Otero, C.M.; Rabinstein, A.A. Rapid blood pressure reduction in acute intracerebral hemorrhage: Feasibility and safety. Neurocrit. Care 2008, 8, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Butcher, K.S.; Jeerakathil, T.; Hill, M.; Demchuk, A.M.; Dowlatshahi, D.; Coutts, S.B.; Gould, B.; McCourt, R.; Asdaghi, N.; Findlay, J.M.; et al. The intracerebral haemorrhage acutely decreasing arterial pressure trial. Stroke 2013, 44, 620–626. [Google Scholar] [CrossRef] [PubMed]
- Boulouis, G.; Morotti, A.; Goldstein, J.N.; Charidimou, A. Intensive blood pressure lowering in patients with acute intracerebral haemorrhage: Clinical outcomes and haemorrhage expansion. Systematic review and meta-analysis of randomised trials. J. Neurol. Neurosurg. Psychiatry 2017, 88, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.S.; Selim, M.H.; Molina, C.A.; Qureshi, A.I. Intensive blood pressure lowering in intracerebral hemorrhage. Stroke 2017, 48, 2034–2037. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Non-Traumatic Hemorrhage | Mortality Event (Row Percent) | ||
|---|---|---|---|
| n (Column Percent) | 3-Day | 14-Day | |
| All | 1493 (100%) | 204 (13.66%) | 369 (24.72%) |
| Sex | |||
| Female | 635 (42.53%) | 92 (14.49%) | 173 (27.24%) |
| Male | 858 (57.47%) | 112 (13.05%) | 196 (22.84%) |
| Marital status | |||
| Missing | 109 (7.30%) | 35 (32.11%) | 59 (54.13%) |
| Unmarried | 311 (20.83%) | 27 (8.68%) | 47 (15.11%) |
| Married | 764 (51.17%) | 98 (12.83%) | 181 (23.69%) |
| Widowed | 207 (13.86%) | 27 (13.04%) | 49 (23.67%) |
| Divorced | 79 (5.29%) | 8 (10.13%) | 22 (27.85%) |
| Others | 23 (1.54%) | 9 (39.13%) | 11 (47.83%) |
| Ethnicity | |||
| White | 1084 (72.61%) | 140 (12.92%) | 259 (23.89%) |
| Black | 111 (7.43%) | 13 (11.71%) | 23 (20.72%) |
| Hispanic or Latino | 59 (3.95%) | 10 (16.95%) | 15 (25.42%) |
| Asian | 56 (3.75%) | 12 (21.43%) | 17 (30.36%) |
| Others | 55 (3.68%) | 6 (10.91%) | 12 (21.82%) |
| Unknown | 128 (8.57%) | 23 (17.97%) | 43 (33.59%) |
| Admission type | |||
| Elective | 35 (2.34%) | 1 (2.86%) | 2 (5.71%) |
| Emergency | 1436 (96.18%) | 201 (14.00%) | 363 (25.28%) |
| Urgent | 22 (1.47%) | 2 (9.09%) | 4 (18.18%) |
| Insurance | |||
| Government | 42 (2.81%) | 2 (4.76%) | 4 (9.52%) |
| Medicaid | 110 (7.37%) | 12 (10.91%) | 22 (20.00%) |
| Medicare | 856 (57.33%) | 128 (14.95%) | 249 (29.09%) |
| Private | 463 (31.01%) | 53(11.45%) | 84 (18.14%) |
| Self-pay | 22 (1.47%) | 9 (40.91%) | 10 (45.45%) |
| Care unit | |||
| CCU | 57 (3.82%) | 9 (15.79%) | 19 (33.33%) |
| CSRU | 22 (1.47%) | 5 (22.73%) | 7 (31.82%) |
| MICU | 298 (19.96%) | 41 (13.76%) | 86 (28.86%) |
| SICU | 850 (56.93%) | 104 (12.24%) | 190 (22.35%) |
| TSICU | 266 (17.82%) | 45 (16.92%) | 67 (25.19%) |
| Age at admission (years) | |||
| 18–34 | 47 (3.15%) | 7 (14.89%) | 8 (17.02%) |
| 35–49 | 168 (11.25%) | 18 (10.71%) | 29 (17.26%) |
| 50–64 | 419 (28.06%) | 56 (13.37%) | 87 (20.76%) |
| 65–79 | 531 (35.57%) | 73 (13.75%) | 142 (26.74%) |
| 80–99 | 328 (21.97%) | 50 (15.24%) | 103 (31.40%) |
| Diabetes | |||
| No | 1183 (79.24%) | 156 (13.19%) | 290 (24.51%) |
| Yes | 310 (20.76%) | 48 (15.48%) | 79 (25.48%) |
| Explicit sepsis | |||
| No | 1423 (95.31%) | 193 (13.56%) | 340 (23.89%) |
| Yes | 70 (4.69%) | 11 (15.71%) | 29 (41.43%) |
| SOFA score | |||
| 0–8 | 177 (11.86%) | 8 (4.52%) | 19 (10.73%) |
| 8–10 | 645 (43.2%) | 44 (6.82%) | 98 (15.19%) |
| 10–11 | 230 (15.41%) | 31 (13.48%) | 52 (22.61%) |
| ≥11 | 441 (29.54%) | 121 (27.44%) | 200 (45.35%) |
| GCS score | |||
| Missing | 1 (0.07%) | 1 (100.00%) | 1 (100.00%) |
| 3–8 | 726 (48.63%) | 186 (25.62%) | 310 (42.70%) |
| 9–12 | 215 (14.40%) | 8 (3.72%) | 26 (12.09%) |
| 13–15 | 551 (36.91%) | 9 (1.63%) | 32 (5.81%) |
| Surgery for ICH | |||
| No | 1190 (79.71%) | 186 (15.63%) | 323 (27.14%) |
| Yes | 303 (20.29%) | 18 (5.94%) | 46 (15.18%) |
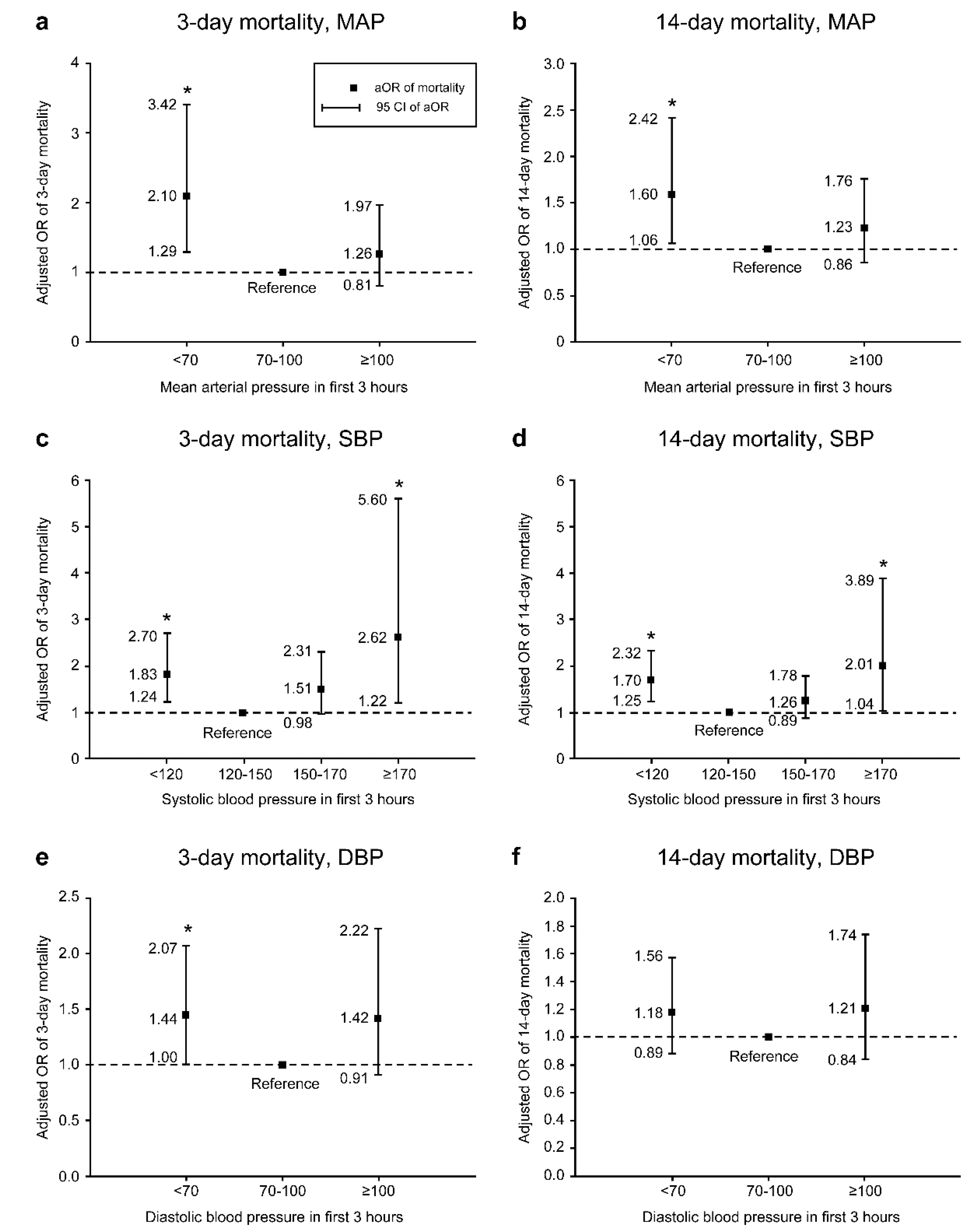
| 3-Day Mortality Rate | 14-Day Mortality Rate | |||
|---|---|---|---|---|
| Death (%) | Crude OR (95% CI) | Death (%) | Crude OR (95% CI) | |
| MAP, mmHg | ||||
| <70 (n = 133) | 31 (23.31%) | 2.15 (1.39–3.34) | 51 (38.35%) | 2.07 (1.42–3.02) |
| 70–100 (n = 1140) | 141 (12.37%) | Reference | 263 (23.07%) | Reference |
| ≥100 (n = 220) | 32 (14.55%) | 1.21 (0.80–1.83) | 55 (25.00%) | 1.11 (0.80–1.55) |
| SBP, mmHg | ||||
| <120 (n = 346) | 60 (17.34%) | 1.65 (1.16–2.35) | 110 (31.79%) | 1.72 (1.30–2.28) |
| 120–150 (n = 826) | 93 (11.26%) | Reference | 176 (21.31%) | Reference |
| 150–170 (n = 275) | 39 (14.18%) | 1.30 (0.87–1.95) | 65 (23.64%) | 1.14 (0.83–1.58) |
| ≥170 (n = 46) | 12 (26.09%) | 2.78 (1.39–5.56) | 18 (39.13%) | 2.37 (1.28–4.39) |
| DBP, mmHg | ||||
| <60 (n = 427) | 72 (16.86%) | 1.54 (1.11–2.14) | 127 (29.74%) | 1.46 (1.12–1.91) |
| 60–100 (n = 824) | 96 (11.65%) | Reference | 185 (22.45%) | Reference |
| ≥100 (n = 242) | 36 (14.88%) | 1.33 (0.88–2.00) | 57 (23.55%) | 1.06 (0.76–1.49) |
| aOR (95% CI) of 14-Day Mortality after ICU Admission | ||||
|---|---|---|---|---|
| Levels of MAP, mmHg | ||||
| <70 | 70–100 | ≥100 | ||
| Age subgroups | ||||
| 18–64 years | 2.62 (1.25–5.51) | Reference | 0.89 (0.49–1.61) | |
| 65–99 years | 1.32 (0.80–2.18) | Reference | 1.46 (0.92–2.31) | |
| pinteraction = 0.1080 | ||||
| Sex subgroup | ||||
| Women | 1.77 (0.99–3.19) | Reference | 1.92 (1.14–3.22) | |
| Men | 1.38 (0.75–2.53) | Reference | 0.80 (0.47–1.34) | |
| pinteraction = 0.0712 | ||||
| GCS subgroup | ||||
| 3–8 | 1.52 (0.89–2.59) | Reference | 1.13 (0.73–1.75) | |
| 9–15 | 1.43 (0.59–3.44) | Reference | 0.59 (0.20–1.73) | |
| pinteraction = 0.2563 | ||||
| Levels of SBP, mmHg | ||||
| <120 | 120–150 | 150–170 | ≥170 | |
| Age subgroups | ||||
| 18–64 years | 1.93 (1.16–3.22) | Reference | 1.01 (0.52–1.95) | 0.97 (0.26–3.61) |
| 65–99 years | 1.58 (1.06–2.37) | Reference | 1.36 (0.90–2.06) | 2.50 (1.16–5.43) |
| pinteraction = 0.7159 | ||||
| Sex subgroup | ||||
| Women | 1.84 (1.15–2.94) | Reference | 1.77 (1.05–2.97) | 2.29 (0.86–6.11) |
| Men | 1.60 (1.05–2.45) | Reference | 0.99 (0.61–1.60) | 1.53 (0.61–3.80) |
| pinteraction = 0.4187 | ||||
| GCS subgroup | ||||
| 3–8 | 1.61 (1.08–2.40) | Reference | 1.16 (0.75–1.79) | 2.82 (1.20–6.65) |
| 9–15 | 1.49 (0.75–2.94) | Reference | 1.13 (0.51–2.46) | All survived |
| pinteraction = 0.8902 | ||||
| Levels of DBP, mmHg | ||||
| <60 | 60–100 | ≥100 | ||
| Age subgroups | ||||
| 18–64 years | 1.35 (0.77–2.37) | Reference | 1.01 (0.58–1.77) | |
| 65–99 years | 1.18 (0.84–1.66) | Reference | 1.33 (0.81–2.20) | |
| pinteraction = 0.3854 | ||||
| Sex subgroup | ||||
| Women | 0.93 (0.60–1.43) | Reference | 1.76 (1.01–3.08) | |
| Men | 1.42 (0.95–2.12) | Reference | 0.85 (0.51–1.39) | |
| pinteraction = 0.0281 | ||||
| GCS subgroup | ||||
| 3–8 | 1.14 (0.79–1.66) | Reference | 1.06 (0.68–1.65) | |
| 9–15 | 1.09 (0.59–2.02) | Reference | 0.68 (0.25–1.87) | |
| pinteraction = 0.6010 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, M.-C.; Kornelius, E.; Chou, Y.-H.; Yang, Y.-S.; Huang, J.-Y.; Huang, C.-N. Optimal Initial Blood Pressure in Intensive Care Unit Patients with Non-Traumatic Intracranial Hemorrhage. Int. J. Environ. Res. Public Health 2020, 17, 3436. https://doi.org/10.3390/ijerph17103436
Wei M-C, Kornelius E, Chou Y-H, Yang Y-S, Huang J-Y, Huang C-N. Optimal Initial Blood Pressure in Intensive Care Unit Patients with Non-Traumatic Intracranial Hemorrhage. International Journal of Environmental Research and Public Health. 2020; 17(10):3436. https://doi.org/10.3390/ijerph17103436
Chicago/Turabian StyleWei, Ming-Cheng, Edy Kornelius, Ying-Hsiang Chou, Yi-Sun Yang, Jing-Yang Huang, and Chien-Ning Huang. 2020. "Optimal Initial Blood Pressure in Intensive Care Unit Patients with Non-Traumatic Intracranial Hemorrhage" International Journal of Environmental Research and Public Health 17, no. 10: 3436. https://doi.org/10.3390/ijerph17103436
APA StyleWei, M.-C., Kornelius, E., Chou, Y.-H., Yang, Y.-S., Huang, J.-Y., & Huang, C.-N. (2020). Optimal Initial Blood Pressure in Intensive Care Unit Patients with Non-Traumatic Intracranial Hemorrhage. International Journal of Environmental Research and Public Health, 17(10), 3436. https://doi.org/10.3390/ijerph17103436