Treatment of Dysphagia in Parkinson’s Disease: A Systematic Review

 ,
,  , and
, and
Abstract
:1. Introductions
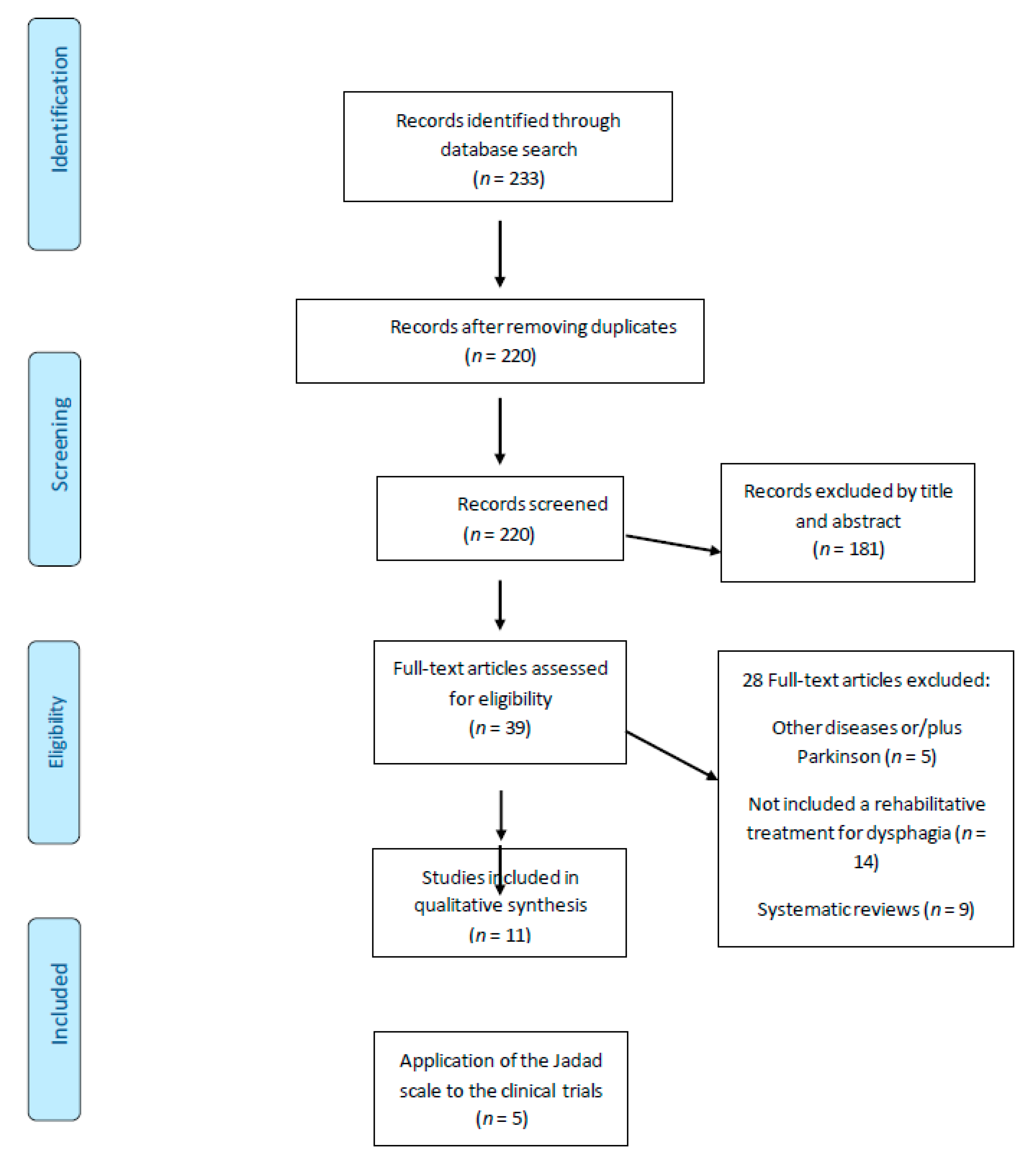
2. Methods
3. Results
3.1. Type of Study
3.2. Application of the Jadad Scale
3.3. Treatment/Intervention or Rehabilitation Techniques
4. Discussion
Limitations and Future Perspectives
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Gómez-Regueira, N.; Escobar-Velando, G. Tratamiento fisioterapéutico de las alteraciones posturales en la enfermedad de Parkinson. Revisión sistemática. Fisioterapia 2017, 39, 33–43. [Google Scholar] [CrossRef]
- Ba, X.-H. Therapeutic effects of GM1 on Parkinson’s disease in rats and its mechanism. Int. J. Neurosci. 2015, 126, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Tysnes, O.-B.; Storstein, A. Epidemiology of Parkinson’s disease. J. Neural Transm. 2017, 124, 901–905. [Google Scholar] [CrossRef] [PubMed]
- Wirdefeldt, K.; Adami, H.-O.; Cole, P.; Trichopoulos, D.; Mandel, J.S. Epidemiology and etiology of Parkinson’s disease: A review of the evidence. Eur. J. Epidemiol. 2011, 26, 1–58. [Google Scholar] [CrossRef] [PubMed]
- León, J.B. Epidemiología de la enfermedad de Parkinson en España y su contextualización mundial. Revista de Neurología 2018, 66, 125. [Google Scholar] [CrossRef]
- Yoritaka, A.; Shimo, Y.; Takanashi, M.; Fukae, J.; Hatano, T.; Nakahara, T.; Miyamato, N.; Urabe, T.; Mori, H.; Hattori, N. Motor and non-motor symptoms of 1453 patients with Parkinson’s disease: Prevalence and risks. Park. Relat. Disord. 2013, 19, 725–731. [Google Scholar] [CrossRef] [Green Version]
- Sato, K.; Hatano, T.; Yamashiro, K.; Kagohashi, M.; Nishioka, K.; Izawa, N.; Mochizuki, H.; Hattori, N.; Mori, H.; Mizuno, Y.; et al. Prognosis of Parkinson’s disease: Time to stage III, IV, V, and to motor fluctuations. Mov. Disord. 2006, 21, 1384–1395. [Google Scholar] [CrossRef] [PubMed]
- Langmore, S.; Terpenning, M.S.; Schork, A.; Chen, Y.; Murray, J.T.; Lopatin, D.; Loesche, W.J. Predictors of aspiration pneumonia: How important is dysphagia? Dysphagia 1998, 13, 69–81. [Google Scholar] [CrossRef] [Green Version]
- Heijnen, B.J.; Speyer, R.; Baijens, L.W.J.; Bogaardt, H. Neuromuscular electrical stimulation versus traditional therapy in patients with parkinson’s disease and oropharyngeal dysphagia: Effects on quality of life. Dysphagia 2011, 27, 336–345. [Google Scholar] [CrossRef] [Green Version]
- Nagaya, M.; Kachi, T.; Yamada, T.; Igata, A. videofluorographic study of swallowing in parkinson’s disease. Dysphagia 1998, 13, 95–100. [Google Scholar] [CrossRef]
- Van Hooren, M.R.A.; Baijens, L.; Voskuilen, S.; Oosterloo, M.; Kremer, B. Treatment effects for dysphagia in Parkinson’s disease: A systematic review. Park. Relat. Disord. 2014, 20, 800–807. [Google Scholar] [CrossRef]
- Ransmayr, G. Physical, occupational, speech and swallowing therapies and physical exercise in Parkinson’s disease. J. Neural Transm. 2011, 118, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Russell, J.A.; Ciucci, M.R.; Connor, N.P.; Schallert, T. Targeted exercise therapy for voice and swallow in persons with Parkinson’s disease. Brain Res. 2010, 1341, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Sharkawi, A.E.; Ramig, L.; Logemann, J.A.; Pauloski, B.R.; Rademaker, A.W.; Smith, C.H.; Pawlas, A.; Baum, S.; Werner, C. Swallowing and voice effects of Lee Silverman Voice. J. Neurol. Neurosurg. Psychiatry 2002, 72, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Evatt, M.L. Nutritional therapies in Parkinson’s disease. Curr. Treat. Options Neurol. 2007, 9, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Crary, M.A.; Sura, L.; Madhavan, A.; Carnaby-Mann, G. Dysphagia in the elderly: Management and nutritional considerations. Clin. Interv. Aging 2012, 7, 287–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizek, P.; Kumar, N.; Jog, M. An update on the diagnosis and treatment of Parkinson disease. Can. Med. Assoc. J. 2016, 188, 1157–1165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Roos, P.; Bloem, B.R.; Kelley, T.A.; Antonini, A.; Dodel, R.; Hagell, P.; Marras, C.; Martinez-Martin, P.; Mehta, S.H.; Odin, P.; et al. A Consensus set of outcomes for Parkinson’s disease from the international consortium for health outcomes measurement. J. Park. Dis. 2017, 7, 533–543. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, U.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Clark, H.D.; Wells, G.A.; Huët, C.; McAlister, F.A.; Salmi, L.R.; Fergusson, D.; Laupacis, A. Assessing the quality of randomized trials: Reliability of the Jadad scale. Control. Clin. Trials 1999, 20, 448–452. [Google Scholar] [CrossRef]
- Troche, M.S.; Sapienza, C.M.; Rosenbek, J.C. Effects of bolus consistency on timing and safety of swallow in patients with Parkinson’s disease. Dysphagia 2007, 23, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Byeon, H. Effect of simultaneous application of postural techniques and expiratory muscle strength training on the enhancement of the swallowing function of patients with dysphagia caused by Parkinson’s disease. J. Phys. Ther. Sci. 2016, 28, 1840–1843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manor, Y.; Mootanah, R.; Freud, D.; Giladi, N.; Cohen, J.T. Video-assisted swallowing therapy for patients with Parkinson’s disease. Park. Relat. Disord. 2013, 19, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Baijens, L.; Speyer, R.; Passos, V.L.; Pilz, W.; Van Der Kruis, J.; Haarmans, S.; Desjardins-Rombouts, C. Surface electrical stimulation in dysphagic parkinson patients: A randomized clinical trial. Laryngoscope 2013, 123, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Argolo, N.; Sampaio, M.; Pinho, P.; Melo, A.; Nóbrega, A.C. Do swallowing exercises improve swallowing dynamic and quality of life in Parkinson’s disease? Neurorehabilitation 2013, 32, 949–955. [Google Scholar] [CrossRef]
- Felix, V.N.; Corrêa, S.M.A.; Soares, R.J. A therapeutic maneuver for oropharyngeal dysphagia in patients with Parkinson’s disease. Clinics 2008, 63, 661–666. [Google Scholar] [CrossRef] [Green Version]
- Baijens, L.; Speyer, R.; Passos, V.L.; Pilz, W.; Roodenburg, N.; Clavé, P. The effect of surface electrical stimulation on swallowing in dysphagic Parkinson patients. Dysphagia 2012, 27, 528–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troche, M.S.; Okun, M.S.; Rosenbek, J.C.; Musson, N.; Fernandez, H.H.; Rodriguez, R.; Romrell, J.; Pitts, T.; Hegland, K.W.; Sapienza, C.M. Aspiration and swallowing in Parkinson disease and rehabilitation with EMST: A randomized trial. Neurology 2010, 75, 1912–1919. [Google Scholar] [CrossRef] [Green Version]
- Pitts, T.; Bolser, D.; Rosenbek, J.; Troche, M.; Okun, M.S.; Sapienza, C. Impact of Expiratory Muscle Strength Training on Voluntary Cough and Swallow Function in Parkinson Disease. Chest 2009, 135, 1301–1308. [Google Scholar] [CrossRef] [Green Version]
- Regan, J.; Walshe, M.; Tobin, W.O. Immediate effects of thermal–tactile stimulation on timing of swallow in idiopathic Parkinson’s disease. Dysphagia 2009, 25, 207–215. [Google Scholar] [CrossRef]
- Smith, S.K.; Roddam, H.; Sheldrick, H. Rehabilitation or compensation: Time for a fresh perspective on speech and language therapy for dysphagia and Parkinson’s disease? Int. J. Lang. Commun. Disord. 2012, 47, 351–364. [Google Scholar] [CrossRef] [PubMed]
- Borrione, P.; Tranchita, E.; Sansone, P.; Parisi, A. Effects of physical activity in Parkinson’s disease: A new tool for rehabilitation. World J. Methodol. 2014, 4, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Fox, C.; Ebersbach, G.; Ramig, L.; Sapir, S. LSVT LOUD and LSVT BIG: Behavioral treatment programs for speech and body movement in Parkinson disease. Park. Dis. 2012, 2012, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Jöbges, E.M.; Spittler-Schneiders, H.; Renner, C.; Hummelsheim, H. Clinical relevance of rehabilitation programs for patients with idiopathic Parkinson syndrome. II: Symptom-specific therapeutic approaches. Park. Relat. Disord. 2007, 13, 203–213. [Google Scholar] [CrossRef]
- Tassorelli, C.; Buscone, S.; Sandrini, G.; Pacchetti, C.; Furnari, A.; Zangaglia, R.; Bartolo, M.; Nappi, G.; Martignoni, E. The role of rehabilitation in deep brain stimulation of the subthalamic nucleus for Parkinson’s disease: A pilot study. Park. Relat. Disord. 2009, 15, 675–681. [Google Scholar] [CrossRef]
- Jiang, Y.; Norman, K.E. Effects of visual and auditory cues on gait initiation in people with Parkinson’s disease. Clin. Rehabil. 2006, 20, 36–45. [Google Scholar] [CrossRef]
- Gadenz, C.D.; Capobianco, D.M.; Cassol, M.; Moreira, T.D.C. Effects of repetitive transcranial magnetic stimulation in the rehabilitation of communication and deglutition disorders: Systematic review of randomized controlled trials. Folia Phoniatr. Logop. 2015, 67, 97–105. [Google Scholar] [CrossRef]
- Dias, A.E.; Barbosa, E.R.; Coracini, K.; Maia, F.; Marcolin, M.A.; Fregni, F. Effects of repetitive transcranial magnetic stimulation on voice and speech in Parkinson’s disease. Acta Neurol. Scand. 2006, 113, 92–99. [Google Scholar] [CrossRef]


{kind=link}
| Search in the Databases | Results |
|---|---|
| SCOPUS | |
| (Parkinson disease) AND (deglutition disorders) AND (rehabilitation) | 33 |
| (Parkinson’s disease) OR (Parkinson and disorders) AND (deglutition disorders) OR (dysphagia) AND (physical therapy specialty) or (physiotherapy) OR (physiotherapy modalities) | 35 |
| Medline | |
| Disease of Parkinson AND dysphagia AND rehabilitation | 37 |
| Disease of Parkinson AND deglutition disorders AND rehabilitation | 28 |
| (Parkinson disorders OR Parkinson’s disease) AND (dysphagia OR oral care OR deglutition disorders) AND (physiotherapy OR physical therapy) AND treatment | 25 |
| Elsevier | |
| Parkinson AND disfagia AND fisioterapia | 47 |
| Pubmed | |
| ((Parkinson disorders OR Parkinson disease)) AND (dysphagia OR deglutition disorders)) AND ((physiotherapy OR physical therapy modalities)) AND mouth rehabilitation | 28 |
| Authors, Year | Type of Study and Participants | Description of Intervention and Duration. Results |
|---|---|---|
| Heijnen et al., 2012 [9] | Randomized Trial. 109 patients. 3 groups (30 patients). NMES vs. Traditional Therapy. | Intervention: Group 1: oral motor exercises, airway protection maneuvers and postural compensation. Group 2 and 3: previous exercises as group 1 plus NMES of the suprahyoid muscle (frequency 80 Hz, pulse width 700 µs). Group 2 received stimulation at the motor level and Group 3 at sensory level. Duration: 13–15 sessions of half an hour each, for five consecutive days per week (3–5 weeks). Evaluation after 3 months of treatment. Results: All groups showed significant effects on the severity scale of dysphagia (Group 1, median = 59, p < 0.001; Group 2, median = 72, p < 0.001; Group 3, median = 74, p = 0.005), as well as improvements in SWAL-QOL (p = 0.001) and MDADI (Global assessment p < 0.001). Minor changes were recorded among the groups. A more comprehensive study may be necessary to clarify these preliminary findings. |
| Troche et al., 2010 [21] | Randomized trial. 60 Parkinson patients. EG = 30 CG = 30 | Intervention: The 30 participants of EG completed EMST. It was a device through which air flows for the expiratory muscles. Duration: 4 weeks, 5 days/week, 20 min/day. For the CG, the device provided little or no load. Results: There were no differences between the pre-treatment groups (p = 0.881). The EMST group (EG) demonstrated an improvement in oropharyngeal function during swallowing (0.61; 95% CI 0.10 to 1.11), these findings were not evident for the CG. |
| Byeon, 2016 [22] | Clinical trial. 33 patients. Group A: 18 only EMST Group B: 15 “postural techniques plus EMST” | Intervention: EMST: the nose was blocked with clips and later, with a mouthpiece, the patients were asked to perform different exercises (inspiration and expiration fast and maximum). Applied for 20 min/day, 5 days/ week. Postural techniques: tilting of the chin, rotation of the head, tilting of the head, bringing the head to extension and flexion, for 30 min/ session and 5 days/week. Duration: 4 weeks. Results: the simultaneous performance of postural techniques and EMST is more effective than using only EMST in dysphagia (22.5 vs. 16.2; p < 0.05). These postural techniques are effective for the swallowing rehabilitation of PD patients who have limited movements of the tongue base or weakened laryngeal raise. |
| Manor et al., 2013 [23] | A randomized study. 42 patients. GE = 21 GC = 21 | Interventions: swallowing exercises and compensatory therapy technique. The only difference was the implementation of the video-assisted tool during each therapy session, for education and assistance in GE. Evaluation at baseline, at 4 weeks and 6 months. Duration: Both groups underwent 6 interventional sessions of 30 min. Results: Both conventional swallowing therapy and VAST approaches proved effectiveness (14.27 vs. 14.65; p = 0.25). The VAST highlights the connection between patients’ level of quality of life, degree of pleasure of eating and the level of satisfaction with the therapy. |
| Baijens et al., 2013 [24] | Randomized controlled trial. N = 90 patients. Three groups. | Intervention: The three groups received traditional speech therapy: diverse airway protecting maneuvers; postural compensation maneuvers; bolus modification and oral intake of different sort of food; swallowing saliva; and oral motor exercises. In addition, two groups received SES, either motor- or sensory-level stimulation. Duration: Daily 30 min, 15 days. Results: No statistically significant differences in FEES (2.67; 95% CI [1.65,4.33]) and VFS (11.30; 95% CI [6.47,19.71] outcome variables were found between any of the three treatment groups (no significant). A therapeutic effect of traditional therapy is suggested, without any additional influence of SES. Further research is required. |
| Argolo et al., 2013 [25] | A before–after trial. 15 consecutive patients | Intervention: Motor swallowing exercises (increase of the strength and range of motion of the mouth, larynx and pharyngeal structures, coordination between breathing and swallowing, and airway protection). Duration: Twice a day, 5 days/week, 5 weeks. Results: Motor swallowing exercises may reduce swallowing disorders in PD patients without lingual pumping and dental absence (beta standardized coefficient = −16.6, 26.2; p = 0.02, 0.002, respectively). Reduction in swallowing disorders was not related with QOL improvement (0.13, [95% CI, 0.6–0.4], p = 0.63). |
| Felix et al., 2008 [26] | A pilot study 10 patients. EG: 4 patients CG: 6 patients | Intervention: Swallow maneuver with effort and biofeedback. Each session included 8 maneuvers: 4 involved saliva and the other 4 solids (cookies). This effort maneuver was induced by requesting “swallow contracting the muscles of the mouth and throat with the greatest possible force”. In addition, a biofeedback device was adapted. Duration: daily sessions (2 weeks) during which a biofeedback resource was used. Results: Patients who had problems with water intake did not show such a problem after rehabilitation, unlike the CG. There was a numerical similarity of the results obtained with the swallowing of saliva or of biscuits (variance = 4.41). None of the patients exhibited difficulty in coughing, drowning or voice disturbance as a result of swallowing after the rehabilitation program (p < 0.001). The effortful swallow maneuver reinforced by using biofeedback was a therapeutic resource. An additional assessment with a larger number of patients is warranted. |
| Baijens et al., 2012 [27] | A pilot study Idiopathic Parkinson’s disease n = 10 Healthy control subjects n = 10 | Intervention: a session of SES using three different electrode positions during videofluoroscopy of swallowing. Temporal, spatial, and visuoperceptual variables were scored. Duration: a single session. Results: showed that SES could alter swallowing in Parkinson’s disease. However, these effects may have been caused mainly by the placebo effect. The changes measured from SES were found in both healthy control subjects and Parkinson patients and the direction of change would not likely benefit swallowing (p > 0.05). Laryngeal vestibule duration (seconds), Position I versus II: 0.03 (−0.013, 0.07) N.S.; Position III versus I: 0.022 (−0.025, 0.069) N.S. Duration horizontal hyoid motion (seconds), Position II versus III: 0.488 (−0.139, 1.116) N.S.; Position III versus I: 0.248 (−0.379, 0.876) N.S. |
| Troche et al., 2008 [28] | Prospective cohort study. 10 patients | Intervention: The study quantified the effects of bolus consistency on specific aspects of movement and bolus flow abnormalities (thin and thick bolus), including swallowing time and number of tongue pumps. Duration: six thin and six pudding-thick boluses were analyzed. Results: a significant difference in oral transit time as a function of bolus thickness, with increased oral transit time with thicker boluses (6.70 vs. 14.30; p = 0.004). No significant difference in pharyngeal transit time between the two consistencies was found (10.35 vs. 10.65; p = 0.910). |
| Pitts et al., 2009 [29] | Prospective cohort study. 10 patients | Intervention: EMST was applied to improve cough and swallow function at home. Duration: 4 weeks, 5 days/week, 5 sets of 5 breaths a day. Results: EMST was an effective treatment for PD patients with risk of aspiration. There was a significant decrease in the compression phase duration (Z = 2.803; p = 0.005) and expiratory phase rise time (Z = 2.492; p = 0.01) (which resulted in a significant increase in cough volume acceleration (Z = 2.497; p = 0.01)). |
| Regan et al., 2010 [30] | A cohort study 13 patients | Intervention: TTS requires little clinical training and has few known contraindications. A Thermo-StimTM (Luminaud, Mentor, OH) implement was employed. Liquid barium and barium paste were the two chosen consistencies. Duration: measures before and after TTS. Results: TTS significantly reduced pharyngeal transit time (0.20 s; p = 0.004), total transit time (0.48 s; p = 0.049), and pharyngeal delay time during swallowing (0.20 s; p = 0.002). |
| Article | The Study Was Described as Randomized | The Method Used to Generate the Sequence of Randomization and Its Appropriation | Study Described as Double-Blind | The Method of Blinding Is Described and Appropriate | There is a Description of Follow-Up and Drop-Out Losses | TOTAL <3/5 Low Quality |
|---|---|---|---|---|---|---|
| Heijnen et al., 2012 [9] | YES | YES | NO | NO | YES | 3/5 |
| Troche et al., 2010 [21] | YES | YES | YES | YES | YES | 5/5 |
| Byeon, 2016 [22] | YES | YES | NO | NO | NO | 2/5 |
| Manor et al., 2013 [23] | YES | YES | YES | YES | NO | 4/5 |
| Baijens et al., 2013 [24] | YES | YES | YES | YES | YES | 5/5 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Liria, R.; Parra-Egeda, J.; Vega-Ramírez, F.A.; Aguilar-Parra, J.M.; Trigueros-Ramos, R.; Morales-Gázquez, M.J.; Rocamora-Pérez, P. Treatment of Dysphagia in Parkinson’s Disease: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4104. https://doi.org/10.3390/ijerph17114104
López-Liria R, Parra-Egeda J, Vega-Ramírez FA, Aguilar-Parra JM, Trigueros-Ramos R, Morales-Gázquez MJ, Rocamora-Pérez P. Treatment of Dysphagia in Parkinson’s Disease: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(11):4104. https://doi.org/10.3390/ijerph17114104
Chicago/Turabian StyleLópez-Liria, Remedios, Jennifer Parra-Egeda, Francisco A. Vega-Ramírez, José Manuel Aguilar-Parra, Rubén Trigueros-Ramos, María José Morales-Gázquez, and Patricia Rocamora-Pérez. 2020. "Treatment of Dysphagia in Parkinson’s Disease: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 11: 4104. https://doi.org/10.3390/ijerph17114104
APA StyleLópez-Liria, R., Parra-Egeda, J., Vega-Ramírez, F. A., Aguilar-Parra, J. M., Trigueros-Ramos, R., Morales-Gázquez, M. J., & Rocamora-Pérez, P. (2020). Treatment of Dysphagia in Parkinson’s Disease: A Systematic Review. International Journal of Environmental Research and Public Health, 17(11), 4104. https://doi.org/10.3390/ijerph17114104