The Retail Food Sector and Indigenous Peoples in High-Income Countries: A Systematic Scoping Review

 , , and
, , and
Abstract
:1. Introduction
2. Methods
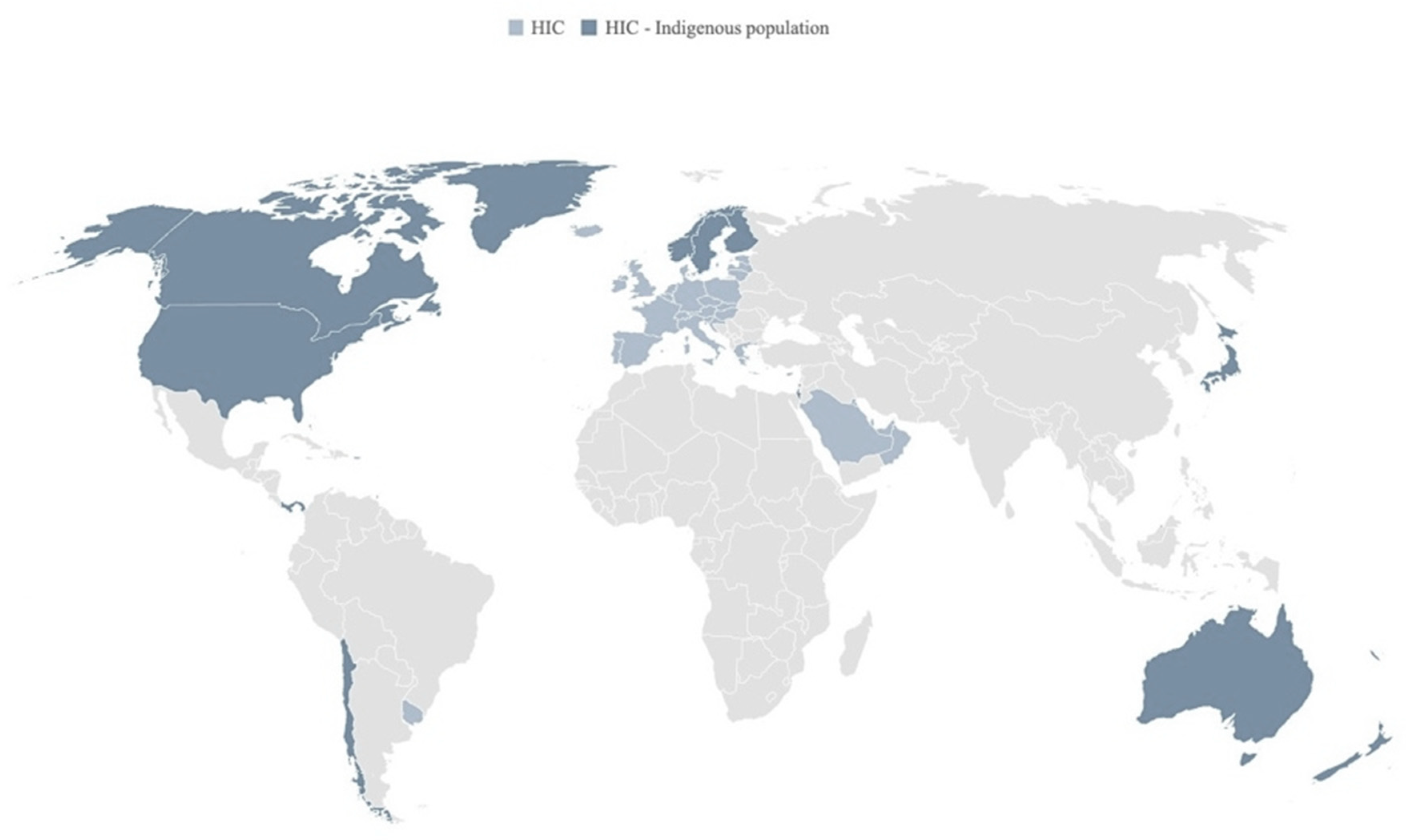
2.1. Context: Indigenous Peoples in HICs
2.2. Literature Review
2.2.1. Systematic Scoping Review
2.2.2. Search Strategy
2.2.3. Eligibility Criteria
2.2.4. Screening
2.2.5. Data Charting
- Retail food supply, including supply chain (i.e., food processing, distribution, transport, warehousing); stores (i.e., characteristics of local food stores, including the geographic density/distribution, and vendor characteristics); food supply (i.e., items available in the store, including their availability (i.e., the presence and diversity of food items in the stores surveyed), affordability (function of food prices, income, and perceptions of value), quality/acceptability (i.e., structured assessments of product properties and perceptions about the appeal, value and convenience of the food supply) and in-store placement/promotion (e.g., shelf space allocation, labels and posters, announcements, etc.));
- Consumers (e.g., store sale records, shopping behavior)
- Interventions and initiatives (e.g., store-based and multisectoral interventions, food pricing policies and subsidies).
3. Results
3.1. Overview of Included Studies
3.1.1. Where has the research been conducted, and which populations have been involved?
3.1.2. How Has the Research Been Undertaken (Indigenous Participation and Study Design)?
3.1.3. What Dimensions and Domains of the Retail Food Sector Have Been Examined?
3.2. Retail Food Sector—Food Supply Chains and Food Imports
3.3. Retail Food Sector—Food Stores
3.3.1. Store Availability and Geographic Accessibility (Type, Number, and/or Location of Stores)
3.3.2. Vendor Characteristics (Store Operation and Management)
3.3.3. Relating Store-Level Factors to Food Supply and Health
3.4. Retail Food Sector—Food Supply
3.4.1. Food Availability
3.4.2. Food Affordability
3.4.3. Food Quality
3.4.4. Point of Purchase Promotion and Information

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Setting 1 | Store(s) Surveyed | Methods | Food Supply 2 | Connection to Diet and Health | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Country | Geography | Number of Stores/Communities | Store Type | Timepoints | Survey Tools 3 (Number and/or Type of Items) | Availability | Affordability (Cost) | Quality | Point of Purchase Promotion | ||
| [94] | US | Rural | 18/2 | Convenience store | Single | NEMS-TCS (ready to eat foods) | ✓ | ✓ | ✓ | ✓ | |
| [83] | US | Rural | 27/1 | Several store types | Single | NEMS-S (68 items) | ✓ | ✓ | |||
| [87] | NZ | Rural; Urban | 392/98 | Supermarket | Single | NEMS-S (5 items—regular vs. healthier choice) | ✓ | ✓ Relative price | ✓ BMI | ||
| [82] | GU | Not specified | 114/ | Large and small stores | Single | NEMS-S (Healthful and less healthful) | ✓ | ✓ Relative price | ✓ | ||
| [26] | CA | Arctic and northern | /6 | Community stores | Seasonal | RNFB (+items based on local diets) | ✓ Nutrition economics | ✓ Not reported | |||
| [93] | US | Arctic and northern | /13 | Community stores | Single | NEMS-S (Fresh produce only) Alaska Food Cost Survey | ✓ | ✓ | ✓ | BMI and diet reported but not related to food supply | |
| [73] | US | Not specified. Comparison on vs. off reservation | 50/22 | Several store types | Single | TFP market basket (68 items) | ✓ | ✓ | |||
| [91] | AU | Several categories | 92/ | Not specified (stores previously surveyed) | Single (compared to 1998) | HFAB | ✓ | ✓ | |||
| [111] | AU | Several categories | 144/ | Grocery stores and community stores | Single | HFAB (430 items costed;13 items for quality) | ✓ | ✓ Based on industry standards | |||
| [71] | US | Rural; Remote | 72/ | Several store types | Single | NEMS-S (Healthful and less healthful) | ✓ | ✓ Relative price | ✓ | ||
| [64] | GU, NC | Capital city | Country-level | Large stores (or chains) | Single | Protocol based on collaboration on nutrients in processed foods (3438 items) | ✓ Country of origin | ✓ Food labels (nutrient data, promotional claims) | |||
| [77] | GU | Not specified | 100/ | Large and small stores | Single | In style of NEMS-S (9 items) | ✓ Sodium content | ||||
| [102] | AU | Remote-compared to capital cities | 20/ | Community stores | Single | 453 items (63% of food expenditure) | ✓ | ||||
| [103] | CA | Remote-compared to capital city | /3 | Community stores | Fall and winter | TNFB + additional foods (22 items) | ✓ | ||||
| [56] | GL | Arctic and northern | 5/5 | Community stores | Single | NEMS-S Freedman Grocery Store Survey | ✓ | ||||
| Reference | Setting 1 | Participants | Food Supply 2 | Consumer and Shopping-Related Issues Discussed by Respondents | ||||
|---|---|---|---|---|---|---|---|---|
| Country | Geography | Availability | Affordability | Quality | Point of Purchase Promotion | |||
| [113] | CA | Arctic and northern | Dene/Métis adults | ✓ | ✓ Expensive | ✓ Lack of freshness | ||
| [59] | US | Rural |
| ✓ | ✓ Higher cost of healthy food | ✓ Quality of meat |
| |
| [96] | CA | Urban | Caregivers of Métis and off-reserve First Nations children | ✓ Unaffordability of both healthy and unhealthy |
| |||
| [98] | CA | Six Nations of the Grand River | Adults (from Six Nations Reserve) | ✓ | ✓ CAD 151/week to feed household |
| ||
| [89] | NZ | Auckland and Wellington | Māori and Pacific shoppers | ✓ | ✓ Higher cost of healthy food | ✓ |
| |
| [84] | US | Rural | American Indian adults | ✓ | ✓ | ✓ |
| |
| [114] | US | Urban; Rural | Tribal leaders (American Indian) |
| ||||
| [115] | AU | Remote | Adults (Aboriginal) | ✓ High cost of food and competing demands for money |
| |||
| [60] | CA | Arctic and northern |
| ✓ | ✓ | ✓ |
| |
| [116] | CA | Arctic and northern |
| ✓ | ✓ | ✓ | ||
| [117] | US | Urban | American Indian women |
| ||||
| [57] | CA | Arctic and northern |
| ✓ | ✓ |
| ||
| [88] | US | Navajo Nation |
| ✓ Predominant foods available are convenient and unhealthy | ✓ |
| ||
| [62] | CA | Arctic and northern | Community members | ✓ | ✓ | ✓ |
| |
| [118] | CA | Arctic and northern |
| ✓ | ||||
| [95] | CA | Arctic and northern | Indigenous women (First Nation, Dene/Métis, Inuit) | ✓ | ||||
| [119] | CA | Arctic and northern (Rural) | Adults (First Nations) |
| ||||
3.5. Consumers
3.5.1. Shopping Location (in/out of Community and by Store Type)
3.5.2. Shopping Frequency and Cycles
3.5.3. Consumer Decision-Making
3.5.4. Store Sales Records
3.6. Improving the Retail Sector
3.6.1. Food System/Security/Sovereignty Priority Setting and Planning
3.6.2. Multi-Sector/Strategies Involving the Retail Sector
3.6.3. Food Pricing Policies (Discounts/Subsidies, Taxes, and Vouchers)
3.6.4. Other Initiatives
| Intervention Name Goal/Type | Setting 4 | Number of Intervention Stores/ Communities 5 | Intervention 6 | Process Evaluation | Evaluation and Impacts Examined 6 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Country | Geography or Location | Availability | Affordability | Quality | Point of Purchase Promotion | Design | Psychosocial | Diet or Purchase | Health | |||
| AHS: Apache Healthy Stores [152,153] Food store-based obesity and chronic disease risk reduction program (dietary improvement) | US | White Mountain and San Carlos Reservation | 11 (6)/2 reservations | ✓ | ✓ | Differed by level. At the store level: high level of dose and reach, and a moderate to high level of fidelity | Quasi-experimental design (pre-test/post-test longitudinal study) | ✓ | ✓ | |||
| CHILE: Child Health Initiative for Lifelong Eating and Exercise [80,162,163,166] Multicomponent obesity prevention intervention for children in Head Start Centers | US | Rural | /6 American Indian sites | ✓ | ✓ | Participant engagement, recruitment and retention | Group randomized controlled trial | ✓ BMI | ||||
| Healthy Communities Project [168] Multicomponent pilot health promotion project (reduce sugary drink consumption and increase water consumption) | AU | Remote | /3 | ✓ Drink availability | Qualitative and quantitative evaluation | ✓
| ✓ Store drink sales (water vs. sugary drink) | |||||
| HFH: Healthy Foods Hawaii [161] Multicomponent obesity risk reduction and dietary improvement intervention for children (includes local producers/distributors) | US | Hawaii | 5/2 (2) | ✓ | ✓ | High fidelity and moderate reach and dose reported | Pre/post-assessment of child-caregiver dyads in intervention and comparison communities | ✓ Knowledge and the perception that healthy foods are convenient (caregiver) | ✓ Healthy Eating Index (HEI) score (children) | |||
| HFN: Healthy Foods North [154,155,156] Multicomponent chronic disease risk reduction and dietary improvement intervention (nutrition and physical activity) | CA | Arctic and northern | 9 food stores + 3 convenience stores /4(2) | ✓ | ✓ | Pre/post-assessment in intervention and comparison communities | ✓ Food related self-efficacy and intentions | ✓ Unhealthy food acquisition frequency | ✓ BMI | |||
| Looma Healthy Lifestyle Program [79] Community-directed healthy lifestyle program to reduce risk of chronic disease (reduce coronary heart disease through dietary modification) | AU | Remote | 1/1 | ✓ | ✓ Appointment of community member as store manager to improve quality of the food supply | Trends in risk factors across the community after the start of the intervention were examined in 3 cross-sectional surveys | ✓ Apparent diet (store turnover method) | ✓ Plasma markers of coronary heart disease risk that are associated with diet | ||||
| NHSI: Healthy Navajo Stores Initiative [125] Multifaceted intervention drawing from National “Healthy Corner Store” best practices (including a fruit and vegetable prescription/voucher program) | US | Navajo Nation (rural/remote) | Stores across Navajo Nation were invited to participate | ✓ Staff training on produce handling to maintain freshness | ✓ | Food environment assessment (fruits and vegetable index score) | Multi-phase longitudinal study; Cross sectional survey of shoppers at participating compared to non-participating stores | ✓ Fruit and vegetable purchasing | ||||
| NHS: Navajo Healthy Stores [157] Multicomponent food environment intervention to increase the availability of healthier foods and | US | Navajo Nation (rural/remote) | Total of 10 store regions across the Navajo Nation (5 immediate, 5 delayed) | ✓ | ✓ | Store-region randomized controlled intervention/ Pre-post differences by intervention group and by intervention exposure level | ✓ Healthy food intentions | ✓ Healthy food acquisition | ✓ BMI | |||
| OPREVENT: Obesity Prevention and Evaluation of InterVention Effectiveness in NaTive North Americans [160] Multicomponent obesity (and related comorbidity) reduction initiative | US | Rural | 25/total 5 (3 immediate, 2 delayed) | ✓ | ✓ |
| Community randomized controlled trial | ✓ | ✓ Dietary assessment | ✓ Anthropometry | ||
| SHOP: Supermarket Healthy Options [112,136,164,172] Multicomponent (price discount and nutrition education) intervention (and pilot study) to promote healthier food purchasing | NZ | Urban | 8/3 (pilot: 1/1) | ✓ Price discounts (with and without nutrition education) | Factorial randomized controlled trial | ✓ Individualized electronic shopping data (healthy food purchasing and percentage energy from saturated fat) | ||||||
| SHOP: Supermarket Healthy Options Project @RIC (Remote Indigenous Communities) [81,176] Multicomponent (price discount and nutrition education) intervention to promote healthier food purchasing | NZ | Not specified | 20/20 | ✓ Price discounts (with and without nutrition education) | A stepped wedge randomized controlled trial | ✓ Weekly store sales data on all food and drinks sold | ✓ Disability Adjusted Life Years (and cost effectiveness) | |||||
| THRIVE: Tribal Health and Resilience in Vulnerable Environments [61,94] Initiative to improve the tribal food environment through interventions in tribally owned convenience stores | US | Rural | 4 (4)/2 Nations | ✓ Variety and convenience | ✓ Reduced pricing | ✓ | . High fidelity across strategies in the intervention reported | Cluster-controlled trial design with treatment conditions at the store level; Mixed-effects linear regression pre- to postintervention changes | ✓ | ✓ Purchasing andfruit and vegetable intake | ||
| ZATPD:Zhiiwapenewin Akino’maagewin: Teaching to Prevent Diabetes [158,159] Multicomponent diabetes prevention (feasibility study) building on the Sandy Lake Health and Diabetes Program and others [184] | CA | Arctic and northern (remote and semi-remote) | /7 First Nations in 4 sites total (2 delayed intervention) | ✓ | ✓ | Moderate fidelity at the store-level | Quasi-experimental pretest/post-test evaluation between intervention and comparison communities | ✓ | ✓ Healthy food acquisition | ✓ Anthropometry | ||
4. Discussion
4.1. Retail/Consumer Food Environment/Supply Issues
4.2. Common Structural Issues Across Regions
4.3. Towards Equitable Food Systems
4.4. Research Gaps, Methodological Considerations and Future Research
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Bank Indigenous Peoples Overview. Available online: https://www.worldbank.org/en/topic/indigenouspeoples (accessed on 4 October 2020).
- Kuhnlein, H.V.; Erasmus, B.; Spigelski, D. Indigenous Peoples’ Food Systems: The Many Dimensions of Culture, Diversity and Environment for Nutrition and Health; Food and Agriculture Organization of the United Nations, Centre for Indigenous Peoples’ Nutrition and Environment: Rome, Italy, 2009; ISBN 9789251060711. [Google Scholar]
- UNPFII Indigenous Peoples, Indigenous Voices. Fact Sheet. Who are Indigenous Peoples? Available online: https://www.un.org/esa/socdev/unpfii/documents/5session_factsheet1.pdf (accessed on 25 May 2020).
- APF; OHCHR. The United Nations Declaration on the Rights of Indigenous Peoples: A Manual for National Human Rights Institutions; Asia Pacific Forum of National Human Rights Institutions and the Office of the United Nations High Commissioner for Human Rights: Sydney, Australia; Geneva, Switzerland, 2013; pp. 1–152. [Google Scholar]
- Osborn, D.; Cutter, A.; Ullah, F. Universal Sustainable Development Goals: Understanding the Transformational Challenge for Developed Countries. Available online: https://sustainabledevelopment.un.org/content/documents/1684SF_-_SDG_Universality_Report_-_May_2015.pdf (accessed on 5 January 2020).
- Reading, C.L.; Wien, F. Health Inequalities and the Social Determinants of Aboriginal Peoples’ Health; National Collaborating Centre for Aboriginal Health: Prince George, BC, Canada, 2009.
- Vos, T.; Barker, B.; Begg, S.; Stanley, L.; Lopez, A.D. Burden of disease and injury in Aboriginal and Torres Strait Islander Peoples: The Indigenous health gap. Int. J. Epidemiol. 2009, 38, 470–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Browne, J.; Hayes, R.; Gleeson, D. Aboriginal health policy: Is nutrition the ‘gap’ in ‘Closing the Gap’? Aust. N. Zeal. J. Public Health 2014, 38, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Council of Canadian Academies. Aboriginal Food Security in Northern Canada: An Assessment of the State of Knowledge; Council of Canadian Academies: Ottawa, ON, Canada, 2014; p. 290. [Google Scholar]
- Jernigan, V.B.B.; Huyser, K.R.; Valdes, J.; Simonds, V.W. Food Insecurity Among American Indians and Alaska Natives: A National Profile Using the Current Population Survey–Food Security Supplement. J. Hunger. Environ. Nutr. 2016, 12, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paradies, Y. Colonisation, racism and indigenous health. J. Popul. Res. 2016, 33, 83–96. [Google Scholar] [CrossRef]
- Albala, C.; Vio, F.; Kain, J.; Uauy, R. Nutrition transition in Chile: Determinants and consequences. Public Health Nutr. 2002, 5, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Lourenço, A.E.P.; Santos, R.V.; Orellana, J.D.Y.; Coimbra, C.E.A., Jr. Nutrition transition in Amazonia: Obesity and socioeconomic change in the Suruí Indians from Brazil. Am. J. Hum. Biol. 2008, 20, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Hughes, R.G.; Lawrence, M. Globalisation, food and health in Pacific Island countries. Asia Pac. J. Clin. Nutr. 2005, 14, 298–305. [Google Scholar] [PubMed]
- Whiting, S.J.; MacKenzie, M.L. Assessing the changing diet of indigenous peoples. Nutr. Rev. 1998, 56, 248–250. [Google Scholar] [CrossRef] [PubMed]
- Kenny, T.-A.; Hu, X.F.; Kuhnlein, H.V.; Wesche, S.; Chan, H.M. Dietary sources of energy and nutrients in the contemporary diet of Inuit adults: Results from the 2007–08 Inuit Health Survey. Public Health Nutr. 2018, 21, 1319–1331. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, M.; Brown, C.; Georga, C.; Miles, E.; Wilson, A.; Brimblecombe, J. Traditional food availability and consumption in remote Aboriginal communities in the Northern Territory, Australia. Aust. N. Zeal. J. Public Health 2017, 25, 585. [Google Scholar] [CrossRef] [PubMed]
- Neitzel, A.L.; Smalls, B.L.; Walker, R.J.; Dawson, A.Z.; Campbell, J.A.; Egede, L.E. Examination of dietary habits among the indigenous Kuna Indians of Panama. Nutr. J. 2019, 18, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brimblecombe, J.; Ferguson, M.; Liberato, S.C.; O’Dea, K.; Riley, M. Optimisation Modelling to Assess Cost of Dietary Improvement in Remote Aboriginal Australia. PLoS ONE 2013, 8, e83587. [Google Scholar] [CrossRef] [PubMed]
- Rosol, R.; Huet, C.; Wood, M.; Lennie, C.; Osborne, G.; Egeland, G.M. Prevalence of affirmative responses to questions of food insecurity: International Polar Year Inuit Health Survey, 2007–2008. Int. J. Circumpolar Health 2011, 70, 488–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huet, C.; Rosol, R.; Egeland, G.M. The Prevalence of Food Insecurity Is High and the Diet Quality Poor in Inuit Communities. J. Nutr. 2012, 142, 541–547. [Google Scholar] [CrossRef]
- Pollard, C.M.; Nyaradi, A.; Lester, M.; Sauer, K. Understanding food security issues in remote Western Australian Indigenous communities. Health Promot. J. Aust. 2014, 25, 83–89. [Google Scholar] [CrossRef]
- Brimblecombe, J.; Ferguson, M.M.; Liberato, S.C.; O’Dea, K. Characteristics of the community-level diet of Aboriginal people in remote northern Australia. Med. J. Aust. 2013, 198, 380–384. [Google Scholar] [CrossRef] [Green Version]
- Kuhnlein, H.V.; Receveur, O.; Soueida, R.; Berti, P.R. Unique patterns of dietary adequacy in three cultures of Canadian Arctic indigenous peoples. Public Health Nutr. 2007, 11, 349–360. [Google Scholar] [CrossRef] [Green Version]
- Pakseresht, M.; Lang, R.; Rittmueller, S.; Roache, C.; Sheehy, T.; Batal, M.; Corriveau, A.; Sharma, S. Food expenditure patterns in the Canadian Arctic show cause for concern for obesity and chronic disease. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 51. [Google Scholar] [CrossRef] [Green Version]
- Kenny, T.-A.; Fillion, M.; MacLean, J.; Wesche, S.D.; Chan, H.M. Calories are cheap, nutrients are expensive—The challenge of healthy living in Arctic communities. Food Policy 2018, 80, 39–54. [Google Scholar] [CrossRef]
- CIA. The World Factbook; CIA: Langley, VA, USA, 2020.
- The Northwest Company. Our Community Promise. Available online: https://www.northwest.ca/about-us/company-profile (accessed on 5 January 2020).
- Caspi, C.E.; Sorensen, G.; Subramanian, S.; Kawachi, I. The local food environment and diet: A systematic review. Health Place 2012, 18, 1172–1187. [Google Scholar] [CrossRef] [Green Version]
- Morland, K.B.; Evenson, K.R. Obesity prevalence and the local food environment. Health Place 2009, 15, 491–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caspi, C.E.; Lenk, K.; Pelletier, J.E.; Barnes, T.L.; Harnack, L.; Erickson, D.J.; Laska, M.N. Association between store food environment and customer purchases in small grocery stores, gas-marts, pharmacies and dollar stores. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Freedman, D.A. Local Food Environments: They’re All Stocked Differently. Am. J. Community Psychol. 2009, 44, 382–393. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A. Nutrient density: Addressing the challenge of obesity. Br. J. Nutr. 2017, 120, S8–S14. [Google Scholar] [CrossRef] [Green Version]
- Drewnowski, A.; Darmon, N. The economics of obesity: Dietary energy density and energy cost. Am. J. Clin. Nutr. 2005, 82, 265S–273S. [Google Scholar] [CrossRef]
- Drewnowski, A.; Specter, S.E. Poverty and obesity: The role of energy density and energy costs. Am. J. Clin. Nutr. 2004, 79, 6–16. [Google Scholar] [CrossRef]
- Pulker, C.E.; Thornton, L.E.; Trapp, G. What is known about consumer nutrition environments in Australia? A scoping review of the literature. Obes. Sci. Pr. 2018, 4, 318–337. [Google Scholar] [CrossRef]
- Ni Mhurchu, C.; Vandevijvere, S.; Waterlander, W.; Thornton, L.E.; Kelly, B.; Cameron, A.J.; Snowdon, W.; Swinburn, B.; INFORMAS. Monitoring the availability of healthy and unhealthy foods and non-alcoholic beverages in community and consumer retail food environments globally. Obes. Rev. 2013, 14, 108–119. [Google Scholar] [CrossRef]
- Turner, C.; Kalamatianou, S.; Drewnowski, A.; Kulkarni, B.; Kinra, S.; Kadiyala, S. Food Environment Research in Low- and Middle-Income Countries: A Systematic Scoping Review. Adv. Nutr. 2019, 18, 93. [Google Scholar] [CrossRef]
- Turner, C.; Aggarwal, A.; Walls, H.; Herforth, A.; Drewnowski, A.; Coates, J.; Kalamatianou, S.; Kadiyala, S. Concepts and critical perspectives for food environment research: A global framework with implications for action in low- and middle-income countries. Glob. Food Secur. 2018, 18, 93–101. [Google Scholar] [CrossRef]
- Olstad, D.L.; Campbell, N.R.; Raine, K.D. Diet quality in Canada: Policy solutions for equity. Can. Med. Assoc. J. 2019, 191, E100–E102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lana, V.; Guest, E.; Dana, L.O.; Vanderlee, L.; Olstad, D.L. Commentary—Food environment and vulnerable populations: Challenges and opportunities for policy. Health Promot. Chronic Dis. Prev. Can. 2018, 37, 321–322. [Google Scholar] [CrossRef] [Green Version]
- Pollard, C.M.; Begley, A.; Landrigan, T.J. The Rise of Food Inequality in Australia. Food Poverty Insecurity Int. Food Inequal. 2015, 38, 89–103. [Google Scholar] [CrossRef]
- HLPE. Nutrition and Food Systems; A Report by the High Level Panel of Experts on Food Security and Nutrition of the Committee on World Food Security (HLPE); HLPE: Rome, Italy, 2017. [Google Scholar]
- Luongo, G.; Skinner, K.; Phillipps, B.; Yu, Z.; Martin, D.H.; Mah, C.L. The Retail Food Environment, Store Foods, and Diet and Health among Indigenous Populations: A Scoping Review. Curr. Obes. Rep. 2020, 374, 1–19. [Google Scholar] [CrossRef]
- Browne, J.; Lock, M.; Walker, T.; Egan, M.; Backholer, K. Effects of food policy actions on Indigenous Peoples’ nutrition-related outcomes: A systematic review. BMJ Glob. Health 2020, 5, e002442. [Google Scholar] [CrossRef]
- Cisneros-Montemayor, A.M.; Pauly, D.; Weatherdon, L.V.; Ota, Y. A Global Estimate of Seafood Consumption by Coastal Indigenous Peoples. PLoS ONE 2016, 11, e0166681. [Google Scholar] [CrossRef]
- Litvinoff, M.P.T.; Anderson, B. World Directory of Minorities and Indigenous Peoples. Available online: https://www.emerald.com/insight/content/doi/10.1108/RR-12-2015-0298/full/html (accessed on 11 March 2019).
- eHRAF World Cultures. Available online: https://ehrafworldcultures.yale.edu/ehrafe/ (accessed on 1 October 2019).
- Anderson, I.; Robson, B.; Connolly, M.; Al-Yaman, F.; Bjertness, E.; King, A.; Tynan, M.; Madden, R.; Bang, A.; Coimbra, C.E.A.; et al. Indigenous and tribal peoples’ health (The Lancet–Lowitja Institute Global Collaboration): A population study. Lancet 2016, 388, 131–157. [Google Scholar] [CrossRef]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Peters, M.D.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid. Based Health 2015, 13, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [Green Version]
- Penchansky, R.; Thomas, J.W. The concept of access: Definition and relationship to consumer satisfaction. Med. Care 1981, 19, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Glanz, K.; Sallis, J.F.; Saelens, B.E.; Frank, L.D. Healthy Nutrition Environments: Concepts and Measures. Am. J. Health Promot. 2005, 19, 330–333. [Google Scholar] [CrossRef] [PubMed]
- Goldhar, C.; Ford, J.D.; Berrang-Ford, L. Prevalence of food insecurity in a Greenlandic community and the importance of social, economic and environmental stressors. Int. J. Circumpolar Health 2012, 69, 285–303. [Google Scholar] [CrossRef] [PubMed]
- Watson, Z.A.; Shanks, C.B.; Miles, M.P.; Rink, E. The Grocery Store Food Environment in Northern Greenland and Its Implications for the Health of Reproductive Age Women. J. Community Health 2018, 43, 175–185. [Google Scholar] [CrossRef]
- Mead, E.; Gittelsohn, J.; Kratzmann, M.; Roache, C.; Sharma, S. Impact of the changing food environment on dietary practices of an Inuit population in Arctic Canada. J. Hum. Nutr. Diet. 2010, 23, 18–26. [Google Scholar] [CrossRef]
- Piltch, E.M.; Shin, S.S.; Houser, R.F.; Griffin, T. The complexities of selling fruits and vegetables in remote Navajo Nation retail outlets: Perspectives from owners and managers of small stores. Public Health Nutr. 2020, 23, 1638–1646. [Google Scholar] [CrossRef]
- Brown, M.C.; Shrestha, U.; Huber, C.; Best, L.G.; O’Leary, M.; Howard, B.; Beresford, S.; Fretts, A.M. Characterizing the local food environment and grocery-store decision making among a large American Indian community in the north-central USA: Qualitative results from the Healthy Foods Healthy Families Feasibility Study. Public Health Nutr. 2019, 22, 2653–2661. [Google Scholar] [CrossRef]
- Ford, J.D.; Beaumier, M. Feeding the family during times of stress: Experience and determinants of food insecurity in an Inuit community. Geogr. J. 2011, 177, 44–61. [Google Scholar] [CrossRef]
- Jernigan, V.B.B.; Salvatore, A.L.; Williams, M.; Wetherill, M.; Taniguchi, T.; Jacob, T.; Cannady, T.; Grammar, M.; Standridge, J.; Fox, J.; et al. A Healthy Retail Intervention in Native American Convenience Stores: The THRIVE Community-Based Participatory Research Study. Am. J. Public Health 2019, 109, 132–139. [Google Scholar] [CrossRef]
- Parker, B.; Burnett, K.; Hay, T.; Skinner, K. The Community Food Environment and Food Insecurity in Sioux Lookout, Ontario: Understanding the Relationships between Food, Health, and Place. J. Hunger. Environ. Nutr. 2018, 14, 762–779. [Google Scholar] [CrossRef]
- Jernigan, V.B.B.; Salvatore, A.L.; Styne, D.M.; Winkleby, M. Addressing food insecurity in a Native American reservation using community-based participatory research. Health Educ. Res. 2012, 27, 645–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snowdon, W.; Raj, A.; Reeve, E.; Guerrero, R.L.; Fesaitu, J.; Cateine, K.; Guignet, C. Processed foods available in the Pacific Islands. Glob. Health 2013, 9, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chodur, G.M.; Shen, Y.; Kodish, S.; Oddo, V.M.; Antiporta, D.A.; Jock, B.; Jones-Smith, J.C. Food Environments around American Indian Reservations: A Mixed Methods Study. PLoS ONE 2016, 11, e0161132. [Google Scholar] [CrossRef] [PubMed]
- Burnett, K.; Skinner, K.; Hay, T.; Leblanc, J.; Chambers, L. Retail food environments, shopping experiences, First Nations and the provincial Norths. Health Promot. Chronic Dis. Prev. Can. 2017, 37, 333–341. [Google Scholar] [CrossRef] [PubMed]
- DyckFehderau, D.; Holt, N.; Ball, G.D.; Willows, N.D. Feasibility study of asset mapping with children: Identifying how the community environment shapes activity and food choices in Alexander First Nation. Rural. Remote. Health 2013, 13, 2289. [Google Scholar] [PubMed]
- Fleischhacker, S.E.; Rodriguez, D.A.; Evenson, K.R.; Henley, A.C.; Gizlice, Z.; Soto, D.; Ramachandran, G. Evidence for validity of five secondary data sources for enumerating retail food outlets in seven American Indian Communities in North Carolina. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 137. [Google Scholar] [CrossRef] [Green Version]
- Smoyer-Tomic, K.E.; Spence, J.C.; Raine, K.D.; Amrhein, C.; Cameron, N.; Yasenovskiy, V.; Cutumisu, N.; Hemphill, E.; Healy, J. The association between neighborhood socioeconomic status and exposure to supermarkets and fast food outlets. Health Place 2008, 14, 740–754. [Google Scholar] [CrossRef]
- Sumner, J.; Tarhan, M.D.; McMurtry, J.J. Eating in Place: Mapping Alternative Food Procurement in Canadian Indigenous Communities. J. Agric. Food Syst. Community Dev. 2019, 9, 239–250. [Google Scholar] [CrossRef]
- Kumar, G.; Jim-Martin, S.; Piltch, E.; Onufrak, S.J.; McNeil, C.; Adams, L.N.; Williams, N.I.; Blanck, H.M.; Curley, L. Healthful Nutrition of Foods in Navajo Nation Stores. Am. J. Health Promot. 2016, 30, 501–510. [Google Scholar] [CrossRef]
- Matanane, L.; Fialkowski, M.K.; Silva, J.; Li, F.; Nigg, C.; Guerrero, R.T.L.; Novotny, R. Para I Famagu’on-Ta: Fruit and Vegetable Intake, Food Store Environment, and Childhood Overweight/Obesity in the Children’s Healthy Living Program on Guam. Hawai’i J. Med. Public Health J. Asia Pac. Med. Public Health 2017, 76, 225–233. [Google Scholar]
- O’Connell, M.; Buchwald, D.S.; Duncan, G.E. Food Access and Cost in American Indian Communities in Washington State. J. Am. Diet. Assoc. 2011, 111, 1375–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galloway, T. Canada’s northern food subsidy Nutrition North Canada: A comprehensive program evaluation. Int. J. Circumpolar Health 2017, 76, 1279451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, S.; Kamal, A.G.; Alam, M.A.; Wiebe, J. Community Development to Feed the Family in Northern Manitoba Communities: Evaluating Food Activities based on Their Food Sovereignty, Food Security, and Sustainable Livelihood Outcomes. Can. J. Nonprofit Soc. Econ. Res. 2012, 3, 43. [Google Scholar] [CrossRef] [Green Version]
- Brimblecombe, J.; Bailie, R.; Boogaard, C.V.D.; Wood, B.; Liberato, S.; Ferguson, M.; Coveney, J.; Jaenke, R.; Ritchie, J. Feasibility of a novel participatory multi-sector continuous improvement approach to enhance food security in remote Indigenous Australian communities. SSM—Popul. Health 2017, 3, 566–576. [Google Scholar] [CrossRef] [PubMed]
- Jackson, S.L. Sodium in Store and Restaurant Food Environments—Guam, 2015. MMWR. Morb. Mortal. Wkly. Rep. 2016, 65, 510–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holden, S.; Ferguson, M.; Brimblecombe, J.; Palermo, C. Can a community of practice equip public health nutritionists to work with remote retail to improve the food supply? Rural. Remote Health 2015, 15, 1–11. [Google Scholar]
- Rowley, K.G.; Su, Q.; Cincotta, M.; Skinner, M.; Skinner, K.; Pindan, B.; White, G.A.; O’Dea, K. Improvements in circulating cholesterol, antioxidants, and homocysteine after dietary intervention in an Australian Aboriginal community. Am. J. Clin. Nutr. 2001, 74, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.M.; Sanders, S.G.; Fitzgerald, C.A.; Keane, P.C.; Canaca, G.F.; Volker-Rector, R. CHILE: An evidence-based preschool intervention for obesity prevention in Head Start. J. Sch. Health 2013, 83, 223–229. [Google Scholar] [CrossRef] [Green Version]
- Brimblecombe, J.; Ferguson, M.M.; Chatfield, M.M.D.; Liberato, S.C.; Gunther, A.; Ball, K.; Moodie, D.P.M.; Miles, E.; Magnus, P.A.; Ni Mhurchu, C.; et al. Effect of a price discount and consumer education strategy on food and beverage purchases in remote Indigenous Australia: A stepped-wedge randomised controlled trial. Lancet Public Health 2017, 2, e82–e95. [Google Scholar] [CrossRef] [Green Version]
- Lundeen, E.A.; VanFrank, B.K.; Jackson, S.L.; Harmon, B.; Uncangco, A.; Luces, P.; Dooyema, C.; Park, S. Availability and Promotion of Healthful Foods in Stores and Restaurants—Guam, 2015. Prev. Chronic Dis. 2017, 14, E56. [Google Scholar] [CrossRef] [Green Version]
- Fretts, A.M.; Huber, C.; Best, L.G.; O’Leary, M.; Lebeau, L.; Howard, B.V.; Siscovick, D.S.; Beresford, S.A. Availability and Cost of Healthy Foods in a Large American Indian Community in the North-Central United States. Prev. Chronic Dis. 2018, 15, E03. [Google Scholar] [CrossRef] [Green Version]
- Love, C.V.; Taniguchi, T.E.; Williams, M.B.; Noonan, C.J.; Wetherill, M.S.; Salvatore, A.L.; Jacob, T.; Cannady, T.K.; Standridge, J.; Spiegel, J.; et al. Diabetes and Obesity Associated with Poor Food Environments in American Indian communities: The THRIVE study. Curr. Dev. Nutr. 2019. [Google Scholar] [CrossRef] [Green Version]
- Mullany, B.; Neault, N.; Tsingine, D.; Powers, J.; Lovato, V.; Clitso, L.; Massey, S.; Talgo, A.; Speakman, K.; Barlow, A. Food insecurity and household eating patterns among vulnerable American-Indian families: Associations with caregiver and food consumption characteristics. Public Health Nutr. 2013, 16, 752–760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, K.W.; Widome, R.; Himes, J.H.; Smyth, M.; Rock, B.H.; Hannan, P.J.; Story, M. High Food Insecurity and Its Correlates Among Families Living on a Rural American Indian Reservation. Am. J. Public Health 2012, 102, 1346–1352. [Google Scholar] [CrossRef] [PubMed]
- Jani, R.; Rush, E.; Crook, N.; Simmons, D. Availability and price of healthier food choices and association with obesity prevalence in New Zealand Māori. Asia Pac. J. Clin. Nutr. 2018, 27, 1357–1365. [Google Scholar] [PubMed]
- Cunningham-Sabo, L.; Bauer, M.; Pareo, S.; Phillips-Benally, S.; Roanhorse, J.; Garcia, L. Qualitative Investigation of Factors Contributing to Effective Nutrition Education for Navajo Families. Matern. Child. Health J. 2008, 12, 68–75. [Google Scholar] [CrossRef]
- Eyles, H.; Ni Mhurchu, C.; Wharemate, L.; Funaki-Tahifote, M.; Lanumata, T.; Rodgers, A. Developing nutrition education resources for a multi-ethnic population in New Zealand. Health Educ. Res. 2009, 24, 558–574. [Google Scholar] [CrossRef] [PubMed]
- Verrall, T.; Napash, L.; Leclerc, L.; Mercure, S.; Gray-Donald, K. Community-based communication strategies to promote infant iron nutrition in northern Canada. Int. J. Circumpolar Health 2006, 65, 65–78. [Google Scholar] [CrossRef]
- Lee, A.; Darcy, A.M.; Leonard, D.; Groos, A.D.; Stubbs, C.O.; Lowson, S.K.; Dunn, S.M.; Coyne, T.; Riley, M.D. Food availability, cost disparity and improvement in relation to accessibility and remoteness in Queensland. Aust. N. Zeal. J. Public Health 2002, 26, 266–272. [Google Scholar] [CrossRef]
- Wendimu, M.A.; Desmarais, A.A.; Martens, T.R. Access and affordability of “healthy” foods in northern Manitoba? The need for Indigenous food sovereignty. Can. Food Stud./La Revue Can. des Études sur L’alimentation 2018, 5, 44–72. [Google Scholar] [CrossRef] [Green Version]
- Johnson, J.S.; Nobmann, E.D.; Asay, E. Factors related to fruit, vegetable and traditional food consumption which may affect health among Alaska Native People in Western Alaska. Int. J. Circumpolar Health 2012, 71, 17345. [Google Scholar] [CrossRef] [PubMed]
- Wetherill, M.S.; Williams, M.B.; Taniguchi, T.; Salvatore, A.L.; Jacob, T.; Cannady, T.; Grammar, M.; Standridge, J.; Fox, J.; Spiegel, J.; et al. A Nutrition Environment Measure to Assess Tribal Convenience Stores: The THRIVE Study. Health Promot. Pr. 2020, 21, 410–420. [Google Scholar] [CrossRef] [PubMed]
- Lambden, J.; Receveur, O.; Marshall, J.; Kuhnlein, H.V. Traditional and market food access in Arctic Canada is affected by economic factors. Int. J. Circumpolar Health 2006, 65, 331–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhawra, J.; Cooke, M.J.; Hanning, R.M.; Wilk, P.; Gonneville, S.L.H. Community perspectives on food insecurity and obesity: Focus groups with caregivers of Métis and Off-reserve First Nations children. Int. J. Equity Health 2015, 14, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Jahns, L.; McDonald, L.; Wadsworth, A.; Morin, C.; Liu, Y.; Nicklas, T. Barriers and facilitators to following the Dietary Guidelines for Americans reported by rural, Northern Plains American-Indian children. Public Health Nutr. 2015, 18, 482–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joseph, P.; Davis, A.D.; Miller, R.; Hill, K.; McCarthy, H.; Banerjee, A.; Chow, C.K.; Mente, A.; Anand, S.S. Contextual determinants of health behaviours in an aboriginal community in Canada: Pilot project. BMC Public Health 2012, 12, 952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiff, R.; Brunger, F. Northern Food Networks: Building Collaborative Efforts for Food Security in Remote Canadian Aboriginal Communities. J. Agric. Food Syst. Community Dev. 2013, 121–138. [Google Scholar] [CrossRef] [Green Version]
- McCarthy, L.; Chang, A.B.; Brimblecombe, J. Food Security Experiences of Aboriginal and Torres Strait Islander Families with Young Children in An Urban Setting: Influencing Factors and Coping Strategies. Int. J. Environ. Res. Public Health 2018, 15, 2649. [Google Scholar] [CrossRef] [Green Version]
- Brimblecombe, J.K.; O’Dea, K. The role of energy cost in food choices for an Aboriginal population in northern Australia. Med. J. Aust. 2009, 190, 549–551. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, M.; O’Dea, K.; Chatfield, M.; Moodie, M.; Altman, J.; Brimblecombe, J. The comparative cost of food and beverages at remote Indigenous communities, Northern Territory, Australia. Aust. N. Zeal. J. Public Health 2016, 40, S21–S26. [Google Scholar] [CrossRef] [Green Version]
- Campbell, M.L.; Diamant, R.M.F.; MacPherson, B.D.; Halladay, J.L. The Contemporary Food Supply of Three Northern Manitoba Cree Communities. Can. J. Public Health 1997, 88, 105–108. [Google Scholar] [CrossRef] [PubMed]
- Mackay, S.; Buch, T.; Vandevijvere, S.; Goodwin, R.; Korohina, E.; Funaki-Tahifote, M.; Lee, A.; Swinburn, B. Cost and Affordability of Diets Modelled on Current Eating Patterns and on Dietary Guidelines, for New Zealand Total Population, Māori and Pacific Households. Int. J. Environ. Res. Public Health 2018, 15, 1255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandevijvere, S.; Young, N.; Mackay, S.; Swinburn, B.; Gahegan, M. Modelling the cost differential between healthy and current diets: The New Zealand case study. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Lewis, M. Testing the Price of Healthy and Current Diets in Remote Aboriginal Communities to Improve Food Security: Development of the Aboriginal and Torres Strait Islander Healthy Diets ASAP (Australian Standardised Affordability and Pricing) Methods. Int. J. Environ. Res. Public Health 2018, 15, 2912. [Google Scholar] [CrossRef] [Green Version]
- Johnson-Down, L.; Willows, N.; Kenny, T.-A.; Ing, A.; Fediuk, K.; Sadik, T.; Chan, H.M.; Batal, M. Optimisation modelling to improve the diets of First Nations individuals. J. Nutr. Sci. 2019, 8, S32. [Google Scholar] [CrossRef] [Green Version]
- Ni Mhurchu, C.; Eyles, H.; Schilling, C.; Yang, Q.; Kaye-Blake, W.; Genç, M.; Blakely, T. Food Prices and Consumer Demand: Differences across Income Levels and Ethnic Groups. PLoS ONE 2013, 8, e75934. [Google Scholar] [CrossRef] [Green Version]
- Gawn, G.; Innes, R.; Rausser, G.C.; Zilberman, D. Nutrient demand and the allocation of time: Evidence from Guam. Appl. Econ. 1993, 25, 811–830. [Google Scholar] [CrossRef]
- Richards, T.J.; Patterson, P.M. Native American Obesity: An Economic Model of the “Thrifty Gene” Theory. Am. J. Agric. Econ. 2006, 88, 542–560. [Google Scholar] [CrossRef]
- Pollard, C.M.; Landrigan, T.J.; Ellies, P.L.; Kerr, D.A.; Lester, M.L.U.; Goodchild, S.E. Geographic factors as determinants of food security: A Western Australian food pricing and quality study. Asia Pac. J. Clin. Nutr. 2014, 23, 1–11. [Google Scholar]
- Eyles, H.; Rodgers, A.; Ni Mhurchu, C. Use of electronic sales data to tailor nutrition education resources for an ethnically diverse population. J. Hum. Nutr. Diet. 2010, 23, 38–47. [Google Scholar] [CrossRef]
- Simoneau, N.; Receveur, O. Attributes of Vitamin A- and Calcium-Rich Food Items Consumed in K’asho Got’ine, Northwest Territories, Canada. J. Nutr. Educ. 2000, 32, 84–93. [Google Scholar] [CrossRef]
- Fleischhacker, S.E.; Vu, M.; Ries, A.; McPhail, A. Engaging Tribal Leaders in an American Indian Healthy Eating Project Through Modified Talking Circles. Fam. Community Health 2011, 34, 202–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brimblecombe, J.; Maypilama, E.; Colles, S.; Scarlett, M.; Dhurrkay, J.G.; Ritchie, J.; O’Dea, K. Factors Influencing Food Choice in an Australian Aboriginal Community. Qual. Health Res. 2014, 24, 387–400. [Google Scholar] [CrossRef] [PubMed]
- Beaumier, M.C.; Ford, J.D. Food Insecurity among Inuit Women Exacerbated by Socio-economic Stresses and Climate Change. Can. J. Public Health 2010, 101, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Dammann, K.W.; Smith, C. Food-Related Environmental, Behavioral, and Personal Factors Associated with Body Mass Index among Urban, Low-Income African-American, American Indian, and Caucasian Women. Am. J. Health Promot. 2011, 25, e1–e10. [Google Scholar] [CrossRef]
- Beaumier, M.C.; Ford, J.D.; Tagalik, S. The food security of Inuit women in Arviat, Nunavut: The role of socio-economic factors and climate change. Polar Rec. 2015, 51, 550–559. [Google Scholar] [CrossRef]
- Stroink, M.L. Understanding Local Food Behaviour and Food Security in Rural First Nation Communities: Implications for Food Policy. J. Rural Community Dev. 2012, 7, 65–82. [Google Scholar]
- Gittelsohn, J.; Toporoff, E.G.; Story, M.; Evans, M.; Anliker, J.; Davis, S.; Sharma, A.; White, J. Food Perceptions and Dietary Behavior of American-Indian Children, Their Caregivers, and Educators: Formative Assessment Findings from Pathways. J. Nutr. Educ. 2000, 32, 2–13. [Google Scholar] [CrossRef] [Green Version]
- Sowerwine, J.; Mucioki, M.; Sarna-Wojcicki, D.; Hillman, L. Reframing food security by and for Native American communities: A case study among tribes in the Klamath River basin of Oregon and California. Food Secur. 2019, 11, 579–607. [Google Scholar] [CrossRef]
- Vaughan, L.A.; Benyshek, D.C.; Martin, J.F. Food Acquisition Habits, Nutrient Intakes, and Anthropometric Data of Havasupai Adults. J. Am. Diet. Assoc. 1997, 97, 1275–1282. [Google Scholar] [CrossRef]
- Genuis, S.K.; Willows, N.; Jardine, C.; Nation, A.F. Through the lens of our cameras: Children’s lived experience with food security in a Canadian Indigenous community. Child. Care Health Dev. 2015, 41, 600–610. [Google Scholar] [CrossRef] [PubMed]
- Wycherley, T.P.; Van Der Pols, J.C.; Daniel, M.; Howard, N.J.; O’Dea, K.; Brimblecombe, J. Associations between Community Environmental-Level Factors and Diet Quality in Geographically Isolated Australian Communities. Int. J. Environ. Res. Public Health 2019, 16, 1943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacKenzie, O.W.; George, C.V.; Pérez-Escamilla, R.; Lasky-Fink, J.; Piltch, E.M.; Sandman, S.M.; Clark, C.; Avalos, Q.J.; Carroll, D.S.; Wilmot, T.M.; et al. Healthy Stores Initiative Associated with Produce Purchasing on Navajo Nation. Curr. Dev. Nutr. 2019, 3, e80973. [Google Scholar] [CrossRef] [PubMed]
- Rowse, T.; Scrimgeour, D.; Knight, S.; Thomas, D. Food-purchasing behaviour in an Aboriginal community. 1. Results of a survey. Aust. J. Public Health 1994, 18, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Wycherley, T.P.; Pekarsky, B.A.; Ferguson, M.M.; O’Dea, K.; Brimblecombe, J.K. Fluctuations in money availability within an income cycle impacts diet quality of remote Indigenous Australians. Public Health Nutr. 2017, 80, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Scelza, B.A.; Bird, D.W.; Bird, R.B. Bush Tucker, Shop Tucker: Production, Consumption, and Diet at an Aboriginal Outstation. Ecol. Food Nutr. 2014, 53, 98–117. [Google Scholar] [CrossRef] [PubMed]
- Scelza, B.A. Food scarcity, not economic constraint limits consumption in a rural Aboriginal community. Aust. J. Rural. Health 2012, 20, 108–112. [Google Scholar] [CrossRef]
- Gittelsohn, J.; Anliker, J.A.; Sharma, S.; Vastine, A.E.; Caballero, B.; Ethelbah, B. Psychosocial Determinants of Food Purchasing and Preparation in American Indian Households. J. Nutr. Educ. Behav. 2006, 38, 163–168. [Google Scholar] [CrossRef]
- Dressler, H.; Smith, C. Health and Eating Behavior Differs between Lean/Normal and Overweight/Obese Low-Income Women Living in Food-Insecure Environments. Am. J. Health Promot. 2013, 27, 358–365. [Google Scholar] [CrossRef]
- Lee, A.J.; O’Dea, K.; Mathews, J.D. Apparent dietary intake in remote Aboriginal communities. Aust. J. Public Health 2010, 18, 190–197. [Google Scholar] [CrossRef]
- Brimblecombe, J.; Liddle, R.; O’Dea, K. Use of point-of-sale data to assess food and nutrient quality in remote stores. Public Health Nutr. 2012, 16, 1159–1167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMahon, E.; Wycherley, T.; O’Dea, K.; Brimblecombe, J. A comparison of dietary estimates from the National Aboriginal and Torres Strait Islander Health Survey to food and beverage purchase data. Aust. N. Zeal. J. Public Health 2017, 41, 598–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wycherley, T.P.; Ferguson, M.; O’Dea, K.; McMahon, E.J.; Liberato, S.; Brimblecombe, J. Store turnover as a predictor of food and beverage provider turnover and associated dietary intake estimates in very remote Indigenous communities. Aust. N. Zeal. J. Public Health 2016, 40, 569–571. [Google Scholar] [CrossRef] [Green Version]
- Ni Mhurchu, C.; Blakely, T.; Wall, J.; Rodgers, A.; Jiang, Y.; Wilton, J. Strategies to promote healthier food purchases: A pilot supermarket intervention study. Public Health Nutr. 2007, 10, 608–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, A.J.; Smith, A.; Bryce, S.; O’Dea, K.; Rutishauser, I.H.; Mathews, J.D. Measuring dietary intake in remote australian aboriginal communities. Ecol. Food Nutr. 1995, 34, 19–31. [Google Scholar] [CrossRef]
- Brimblecombe, J.; Mackerras, D.; Clifford, P.; O’Dea, K. Does the store-turnover method still provide a useful guide to food intakes in Aboriginal communities? Aust. N. Zeal. J. Public Health 2006, 30, 444–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wakegijig, J.; Osborne, G.; Statham, S.; Issaluk, M.D. Collaborating toward improving food security in Nunavut. Int. J. Circumpolar Health 2013, 72. [Google Scholar] [CrossRef]
- Rogers, A.; Ferguson, M.M.; Ritchie, J.; Boogaard, C.V.D.; Brimblecombe, J.K. Strengthening food systems with remote Indigenous Australians: Stakeholders’ perspectives. Health Promot. Int. 2018, 33, 38–48. [Google Scholar] [CrossRef] [Green Version]
- Brimblecombe, J.; Boogaard, C.H.V.D.; Ritchie, J.; Bailie, R.; Coveney, J.; Liberato, S.C. From targets to ripples: Tracing the process of developing a community capacity building appraisal tool with remote Australian indigenous communities to tackle food security. BMC Public Health 2014, 14, 914. [Google Scholar] [CrossRef] [Green Version]
- Skinner, K.; Hanning, R.M.; Desjardins, E.; Tsuji, L.J.S. Giving voice to food insecurity in a remote indigenous community in subarctic Ontario, Canada: Traditional ways, ways to cope, ways forward. BMC Public Health 2013, 13, 427. [Google Scholar] [CrossRef] [Green Version]
- Calancie, L.; Stowers, K.C.; Palmer, A.; Frost, N.; Calhoun, H.; Piner, A.; Webb, K. Toward a Community Impact Assessment for Food Policy Councils: Identifying Potential Impact Domains. J. Agric. Food Syst. Community Dev. 2018, 8, 1–14. [Google Scholar] [CrossRef]
- Signal, L.; Walton, M.D.; Ni Mhurchu, C.; Maddison, R.; Bowers, S.G.; Carter, K.N.; Gorton, D.; Heta, C.; Lanumata, T.S.; McKerchar, C.W.; et al. Tackling ’wicked’ health promotion problems: A New Zealand case study. Health Promot. Int. 2013, 28, 84–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, H.M.; Fediuk, K.; Hamilton, S.; Rostas, L.; Caughey, A.; Kuhnlein, H.; Egeland, G.; Loring, E. Food security in Nunavut, Canada: Barriers and recommendations. Int. J. Circumpolar Health 2006, 65, 416–431. [Google Scholar] [CrossRef] [PubMed]
- Skinner, K.; Hanning, R.M.; Sutherland, C.; Edwards-Wheesk, R.; Tsuji, L.J.S. Using a SWOT Analysis to Inform Healthy Eating and Physical Activity Strategies for a Remote First Nations Community in Canada. Am. J. Health Promot. 2012, 26, e159–e170. [Google Scholar] [CrossRef] [PubMed]
- Brimblecombe, J.; Boogaard, C.V.D.; Wood, B.; Liberato, S.C.; Brown, J.; Barnes, A.; Rogers, A.; Coveney, J.; Ritchie, J.; Bailie, R. Development of the good food planning tool: A food system approach to food security in indigenous Australian remote communities. Health Place 2015, 34, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, K.R.; McLachlan, S.M. Seeking Indigenous food sovereignty: Origins of and responses to the food crisis in northern Manitoba, Canada. Local Environ. 2013, 18, 1079–1098. [Google Scholar] [CrossRef]
- McDonald, E.L.; Bailie, R.S.; Morris, P.S. Participatory systems approach to health improvement in Australian Aboriginal children. Health Promot. Int. 2017, 32, 62–72. [Google Scholar] [CrossRef] [Green Version]
- Sowerwine, J.; Sarna-Wojcicki, D.; Mucioki, M.; Hillman, L.; Lake, F.K.; Friedman, E. Enhancing Food Sovereignty: A Five-year Collaborative Tribal-University Research and Extension Project in California and Oregon. J. Agric. Food Syst. Community Dev. 2019, 9, 1–24. [Google Scholar] [CrossRef]
- Ferguson, M.; O’Dea, K.; Altman, J.; Moodie, M.; Brimblecombe, J. Health-Promoting Food Pricing Policies and Decision-Making in Very Remote Aboriginal and Torres Strait Islander Community Stores in Australia. Int. J. Environ. Res. Public Health 2018, 15, 2908. [Google Scholar] [CrossRef] [Green Version]
- Curran, S.; Gittelsohn, J.; Anliker, J.; Ethelbah, B.; Blake, K.; Sharma, S.; Caballero, B. Process evaluation of a store-based environmental obesity intervention on two American Indian Reservations. Health Educ. Res. 2005, 20, 719–729. [Google Scholar] [CrossRef] [Green Version]
- Vastine, A.; Gittelsohn, J.; Ethelbah, B.; Anliker, J.; Caballero, B. Formative Research and Stakeholder Participation in Intervention Development. Am. J. Health Behav. 2005, 29, 57–69. [Google Scholar] [CrossRef]
- Sharma, S.; Gittelsohn, J.; Rosol, R.; Beck, L. Addressing the public health burden caused by the nutrition transition through the Healthy Foods North nutrition and lifestyle intervention programme. J. Hum. Nutr. Diet. 2010, 23, 120–127. [Google Scholar] [CrossRef]
- Gittelsohn, J. Participatory Research for Chronic Disease Prevention in Inuit Communities. Am. J. Health Behav. 2010, 34, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Mead, E.L.; Gittelsohn, J.; Roache, C.; Corriveau, A.; Sharma, S. A Community-Based, Environmental Chronic Disease Prevention Intervention to Improve Healthy Eating Psychosocial Factors and Behaviors in Indigenous Populations in the Canadian Arctic. Health Educ. Behav. 2013, 40, 592–602. [Google Scholar] [CrossRef] [PubMed]
- Gittelsohn, J.; Kim, E.M.; He, S.; Pardilla, M. A Food Store–Based Environmental Intervention Is Associated with Reduced BMI and Improved Psychosocial Factors and Food-Related Behaviors on the Navajo Nation. J. Nutr. 2013, 143, 1494–1500. [Google Scholar] [CrossRef]
- Rosecrans, A.M.; Gittelsohn, J.; Ho, L.S.; Harris, S.B.; Naqshbandi, M.; Sharma, S. Process evaluation of a multi-institutional community-based program for diabetes prevention among First Nations. Health Educ. Res. 2008, 23, 272–286. [Google Scholar] [CrossRef] [Green Version]
- Ho, L.S.; Gittelsohn, J.; Rimal, R.; Treuth, M.S.; Sharma, S.; Rosecrans, A.; Harris, S.B. An Integrated Multi-Institutional Diabetes Prevention Program Improves Knowledge and Healthy Food Acquisition in Northwestern Ontario First Nations. Health Educ. Behav. 2008, 35, 561–573. [Google Scholar] [CrossRef] [PubMed]
- Redmond, L.C.; Jock, B.; Gadhoke, P.; Chiu, D.T.; Christiansen, K.; Pardilla, M.; Swartz, J.; Platero, H.; Caulfield, L.E.; Gittelsohn, J. OPREVENT (Obesity Prevention and Evaluation of InterVention Effectiveness in NaTive North Americans): Design of a Multilevel, Multicomponent Obesity Intervention for Native American Adults and Households. Curr. Dev. Nutr. 2019, 3, 81–93. [Google Scholar] [CrossRef]
- Gittelsohn, J.; Vijayadeva, V.; Davison, N.; Ramirez, V.; Cheung, L.W.; Murphy, S.; Novotny, R. A Food Store Intervention Trial Improves Caregiver Psychosocial Factors and Children’s Dietary Intake in Hawaii. Obesity 2010, 18, S84–S90. [Google Scholar] [CrossRef]
- Sussman, A.L.; Davis, S.M. Integrating Formative Assessment and Participatory Research. Am. J. Health Educ. 2010, 41, 244–249. [Google Scholar] [CrossRef] [Green Version]
- Cruz, T.H.; Davis, S.M.; Fitzgerald, C.A.; Canaca, G.F.; Keane, P.C. Engagement, recruitment, and retention in a trans-community, randomized controlled trial for the prevention of obesity in rural American Indian and Hispanic children. J. Prim. Prev. 2014, 35, 135–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blakely, T.; Ni Mhurchu, C.; Jiang, Y.; Matoe, L.; Funaki-Tahifote, M.; Eyles, H.; Foster, R.H.; McKenzie, S.; Rodgers, A. Do effects of price discounts and nutrition education on food purchases vary by ethnicity, income and education? Results from a randomised, controlled trial. J. Epidemiol. Community Health 2011, 65, 902–908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scrimgeour, D.; Rowse, T.; Knight, S. Food-purchasing behaviour in an Aboriginal community. 2. Evaluation of an intervention aimed at children. Aust. J. Public Health 1994, 18, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.M.; Myers, O.B.; Cruz, T.H.; Morshed, A.B.; Canaca, G.F.; Keane, P.C.; O’Donald, E.R. CHILE: Outcomes of a group randomized controlled trial of an intervention to prevent obesity in preschool Hispanic and American Indian children. Prev. Med. 2016, 89, 162–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrison, N.; Dooley, J. The Sioux Lookout Diabetes Program: Diabetes prevention and management in northwestern Ontario. Int. J. Circumpolar Health 1998, 57, 364–369. [Google Scholar] [PubMed]
- Fehring, E.; Ferguson, M.; Brown, C.; Murtha, K.; Laws, C.; Cuthbert, K.; Thompson, K.; Williams, T.; Hammond, M.; Brimblecombe, J. Supporting healthy drink choices in remote Aboriginal and Torres Strait Islander communities: A community-led supportive environment approach. Aust. N. Zeal. J. Public Health 2019, 43, 551–557. [Google Scholar] [CrossRef]
- Brown, C.; Laws, C.; Leonard, D.; Campbell, S.; Merone, L.; Hammond, M.; Thompson, K.; Canuto, K.; Brimblecombe, J. Healthy Choice Rewards: A Feasibility Trial of Incentives to Influence Consumer Food Choices in a Remote Australian Aboriginal Community. Int. J. Environ. Res. Public Health 2019, 16, 112. [Google Scholar] [CrossRef] [Green Version]
- Ni Mhurchu, C.; Eyles, H.; Dixon, R.; Matoe, L.; Teevale, T.; Meagher-Lundberg, P. Economic incentives to promote healthier food purchases: Exploring acceptability and key factors for success. Health Promot. Int. 2012, 27, 331–341. [Google Scholar] [CrossRef] [Green Version]
- Snowdon, W. Sugar-sweetened beverages in Pacific Island countries and territories: Problems and solutions? Pac. Health Dialog 2014, 20, 43–46. [Google Scholar]
- Ni Mhurchu, C.; Blakely, T.; Funaki-Tahifote, M.; McKerchar, C.; Wilton, J.; Chua, S.; Jiang, Y. Inclusion of indigenous and ethnic minority populations in intervention trials: Challenges and strategies in a New Zealand supermarket study. J. Epidemiol. Community Health 2009, 63, 850–855. [Google Scholar] [CrossRef]
- Black, A.P.; Vally, H.; Morris, P.S.; Daniel, M.; Esterman, A.J.; Smith, F.E.; O’Dea, K. Health outcomes of a subsidised fruit and vegetable program for Aboriginal children in northern New South Wales. Med. J. Aust. 2013, 199, 46–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, A.P.; Vally, H.; Morris, P.; Daniel, M.; Esterman, A.; Karschimkus, C.S.; O’Dea, K. Nutritional impacts of a fruit and vegetable subsidy programme for disadvantaged Australian Aboriginal children. Br. J. Nutr. 2013, 110, 2309–2317. [Google Scholar] [CrossRef] [Green Version]
- Magnus, A.; Moodie, M.L.; Ferguson, M.; Cobiac, L.J.; Liberato, S.C.; Brimblecombe, J. The economic feasibility of price discounts to improve diet in Australian Aboriginal remote communities. Aust. N. Zeal. J. Public Health 2016, 40, S36–S41. [Google Scholar] [CrossRef] [PubMed]
- Magnus, A.; Cobiac, L.; Brimblecombe, J.; Chatfield, M.; Gunther, A.; Ferguson, M.; Moodie, M. The cost-effectiveness of a 20% price discount on fruit, vegetables, diet drinks and water, trialled in remote Australia to improve Indigenous health. PLoS ONE 2018, 13, e0204005. [Google Scholar] [CrossRef] [PubMed]
- Ni Mhurchu, C.; Eyles, H.; Genç, M.; Scarborough, P.; Rayner, M.; Mizdrak, A.; Nnoaham, K.; Blakely, T. Effects of Health-Related Food Taxes and Subsidies on Mortality from Diet-Related Disease in New Zealand: An Econometric-Epidemiologic Modelling Study. PLoS ONE 2015, 10, e0128477. [Google Scholar] [CrossRef] [PubMed]
- Cueva, K.; Lovato, V.; Nieto, T.; Neault, N.; Barlow, A.; Speakman, K. Increasing Healthy Food Availability, Purchasing, and Consumption: Lessons Learned from Implementing a Mobile Grocery. Prog. Community Health Partnersh. Res. Educ. Action 2018, 12, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Lotoski, L.C.; Engler-Stringer, R.; Muhajarine, N. Cross-sectional analysis of a community-based cooperative grocery store intervention in Saskatoon, Canada. Can. J. Public Health 2015, 106, e147–e153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMahon, E.J.; Webster, J.; Brimblecombe, J. Effect of 25% Sodium Reduction on Sales of a Top-Selling Bread in Remote Indigenous Australian Community Stores: A Controlled Intervention Trial. Nutrition 2017, 9, 214. [Google Scholar] [CrossRef]
- McMahon, E.J.; Clarke, R.; Jaenke, R.; Brimblecombe, J. Detection of 12.5% and 25% Salt Reduction in Bread in a Remote Indigenous Australian Community. Nutrition 2016, 8, 169. [Google Scholar] [CrossRef]
- Nhung, N.T.H.; Blakely, T.; Cobiac, L.J.; Pearson, A.L.; Wilson, N. Health and Economic Impacts of Eight Different Dietary Salt Reduction Interventions. PLoS ONE 2015, 10, e0123915. [Google Scholar] [CrossRef]
- McMahon, E.J.; Webster, J.; O’Dea, K.; Brimblecombe, J. Dietary sodium and iodine in remote Indigenous Australian communities: Will salt-reduction strategies increase risk of iodine deficiency? A cross-sectional analysis and simulation study. BMC Public Health 2015, 15, 1318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, L.S.; Gittelsohn, J.; Harris, S.B.; Ford, E. Development of an integrated diabetes prevention program with First Nations in Canada. Health Promot. Int. 2006, 21, 88–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WorldBank. How Does the World Bank Classify Countries? Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/378834-how-does-the-world-bank-classify-countries (accessed on 20 September 2019).
- Lytle, L.A.; Sokol, R.L. Measures of the food environment: A systematic review of the field, 2007–2015. Health Place 2017, 44, 18–34. [Google Scholar] [CrossRef] [PubMed]
- Ploeg, M.V.; Wilde, P.E. How do food retail choices vary within and between food retail environments? Food Policy 2018, 79, 300–308. [Google Scholar] [CrossRef]
- Walker, R.E.; Keane, C.R.; Burke, J.G. Disparities and access to healthy food in the United States: A review of food deserts literature. Health Place 2010, 16, 876–884. [Google Scholar] [CrossRef] [PubMed]
- Dammann, K.W.; Smith, C. Factors Affecting Low-income Women’s Food Choices and the Perceived Impact of Dietary Intake and Socioeconomic Status on Their Health and Weight. J. Nutr. Educ. Behav. 2009, 41, 242–253. [Google Scholar] [CrossRef]
- Kaufman, P.; Dicken, C.; Williams, R. Measuring Access to Healthful, Affordable Food in American Indian and Alaska Native Tribal Areas; EIB-131; U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2014; pp. 1–35.
- Sacks, G.; Swinburn, B.; Kraak, V.I.; Downs, S.; Walker, C.; Barquera, S.; Friel, S.; Hawkes, C.; Kelly, B.; Kumanyika, S.; et al. A proposed approach to monitor private-sector policies and practices related to food environments, obesity and non-communicable disease prevention. Obes. Rev. 2013, 14, 38–48. [Google Scholar] [CrossRef] [Green Version]
- Castellari, E.; Moro, D.; Platoni, S.; Sckokai, P. Retailers’ strategies and food price dynamics: Evidence from dairy scanner data. Food Policy 2018, 74, 212–224. [Google Scholar] [CrossRef]
- Lee, A.J.; Bonson, A.P.; Powers, J.R. The effect of retail store managers on Aboriginal diet in remote communities. Aust. N. Zeal. J. Public Health 1996, 20, 212–214. [Google Scholar] [CrossRef]
- Ford, J.D.; Lardeau, M.-P.; Vanderbilt, W. The characteristics and experience of community food program users in arctic Canada: A case study from Iqaluit, Nunavut. BMC Public Health 2012, 12, 464. [Google Scholar] [CrossRef] [Green Version]
- Cooksey-Stowers, K.; Schwartz, M.B.; Brownell, K.D. Food Swamps Predict Obesity Rates Better Than Food Deserts in the United States. Int. J. Environ. Res. Public Health 2017, 14, 1366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hager, E.R.; Cockerham, A.; O’Reilly, N.; Harrington, D.; Harding, J.; Hurley, K.M.; Black, M.M. Food swamps and food deserts in Baltimore City, MD, USA: Associations with dietary behaviours among urban adolescent girls. Public Health Nutr. 2016, 20, 2598–2607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budzynska, K.; West, P.; Savoy-Moore, R.T.; Lindsey, D.; Winter, M.; Newby, P.K. A food desert in Detroit: Associations with food shopping and eating behaviours, dietary intakes and obesity. Public Health Nutr. 2013, 16, 2114–2123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trewin, D. National Aboriginal and Torres Strait Islander Health Survey, 2004–2005; Australian Bureau of Statistics: Melbourne, Australia, 2006.
- Zienczuk, N.; Young, T.K.; Cao, Z.R.; Egeland, G.M. Dietary correlates of an at-risk BMI among Inuit adults in the Canadian high arctic: Cross-sectional international polar year Inuit health survey, 2007–2008. Nutr. J. 2012, 11, 73. [Google Scholar] [CrossRef] [Green Version]
- Maru, Y.T.; Smith, M.S.; Sparrow, A.; Pinho, P.F.; Dube, O.P. A linked vulnerability and resilience framework for adaptation pathways in remote disadvantaged communities. Glob. Environ. Chang. 2014, 28, 337–350. [Google Scholar] [CrossRef]
- Singh-Peterson, L.; Lieske, S.; Underhill, S.J.R.; Keys, N. Food security, remoteness and consolidation of supermarket distribution centres: Factors contributing to food pricing inequalities across Queensland, Australia. Aust Geogr. 2015, 47, 89–102. [Google Scholar] [CrossRef]
- Novotny, R.; Vijayadeva, V.; Ramirez, V.; Lee, S.K.; Davison, N.; Gittelsohn, J. Development and Implementation of a Food System Intervention to Prevent Childhood Obesity in Rural Hawai‘i. Hawaii Med. J. 2011, 70, 42–46. [Google Scholar]
- Whyte, K. Food Sovereignty, Justice and Indigenous Peoples: An Essay on Settler Colonialism and Collective Continuance. In Oxford Handbook on Food Ethics; Barnhill, A., Doggett, T., Budolfson, M., Eds.; Oxford University Press: Oxford, UK, 2017; pp. 1–21. [Google Scholar]
- Daher, O.; Hannikainen, L.; Heikinheimo-Pérez, K. National Minorities in Finland–Richness of Cultures and Languages; Minority Rights Group Finland: London, UK, 2016. [Google Scholar]
- Daigle, M. Tracing the terrain of Indigenous food sovereignties. J. Peasant. Stud. 2017, 18, 1–19. [Google Scholar] [CrossRef]
- Coté, C. “Indigenizing” Food Sovereignty. Revitalizing Indigenous Food Practices and Ecological Knowledges in Canada and the United States. Humanities 2016, 5, 57. [Google Scholar] [CrossRef]
- Harder, M.T.; Wenzel, G.W. Inuit Subsistence, Social Economy and Food Security in Clyde River, Nunavut. Arctic 2012, 65, 305–318. [Google Scholar] [CrossRef]
- Wenzel, G.W. Inuit and modern hunter-gatherer subsistence. Études/Inuit/Studies 2013, 37, 181–200. [Google Scholar] [CrossRef] [Green Version]
- Jonasson, M.E.; Spiegel, S.J.; Thomas, S.; Yassi, A.; Wittman, H.; Takaro, T.; Afshari, R.; Markwick, M.; Spiegel, J.M. Oil pipelines and food sovereignty: Threat to health equity for Indigenous communities. J. Public Health Policy 2019, 40, 504–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, L. Toxic contamination undermining Indigenous food systems and Indigenous sovereignty. Pimatiziwin J. Aborig. Indig. Community Health 2003, 1, 130–134. [Google Scholar]
- Parlee, B.; Sandlos, J.; Natcher, D. Undermining subsistence: Barren-ground caribou in a “tragedy of open access”. Sci. Adv. 2018, 4, e1701611. [Google Scholar] [CrossRef] [Green Version]
- Whyte, K. Indigenous Food Sovereignty, Renewal and U.S. Settler Colonialism. In The Routledge Handbook of Food Ethics; Routledge: New York, NY, USA, 2016; pp. 354–365. [Google Scholar]
- Whyte, K. Indigenous Food Systems, Environmental Justice, and Settler-Industrial States. In Global Food, Global Justice: Essays on Eating under Globalization; Rawlinson, M., Ward, C., Eds.; Cambridge Scholars Publishing: Newcastle upon Tyne, UK, 2015; pp. 143–156. [Google Scholar]
- Seymour, J.D. Impact of nutrition environmental interventions on point-of-purchase behavior in adults: A review. Prev. Med. 2004, 39, 108–136. [Google Scholar] [CrossRef]
- Ni Mhurchu, C.; Blakely, T.; Jiang, Y.; Eyles, H.C.; Rodgers, A. Effects of price discounts and tailored nutrition education on supermarket purchases: A randomized controlled trial. Am. J. Clin. Nutr. 2010, 91, 736–747. [Google Scholar] [CrossRef] [Green Version]
- St-Germain, A.-A.F.; Galloway, T.; Tarasuk, V. Food insecurity in Nunavut following the introduction of Nutrition North Canada. Can. Med. Assoc. J. 2019, 191, E552–E558. [Google Scholar] [CrossRef] [Green Version]
- Socha, T.; Chambers, L.; Zahaf, M.; Abraham, R.; Fiddler, T. Food availability, food store management, and food pricing in a northern community First Nation community. Int. J. Humanit. Soc. Sci. 2011, 1, 49–61. [Google Scholar]
- Socha, T.; Zahaf, M.; Chambers, L.; Abraham, R.; Fiddler, T. Food Security in a Northern First Nations Community: An Exploratory Study on Food Availability and Accessibility. J. Aborig. Health 2012, 8, 5–14. [Google Scholar]
- Pollard, C.M. Selecting Interventions for Food Security in Remote Indigenous Communities. In Food Security in Australia; Springer: Berlin/Heidelberg, Germany, 2012; Volume 100, pp. 97–112. [Google Scholar]
- House of Representatives Standing Committee on Aboriginal and Torres Strait Islander Affairs. Everybody’s Business: Remote Aboriginal and Torres Strait Community Stores; The Parliament of the Commonwealth of Australia: Canberra, Australia, 2009.
- Niclasen, B.; Molcho, M.; Arnfjord, S.; Schnohr, C. Conceptualizing and contextualizing food insecurity among Greenlandic children. Int. J. Circumpolar Health 2013, 72, 19928. [Google Scholar] [CrossRef] [Green Version]
- Wetherill, M.S.; Williams, M.B.; Hartwell, M.L.; Salvatore, A.L.; Jacob, T.; Cannady, T.K.; Standridge, J.; Fox, J.; Spiegel, J.; Anderson, N.; et al. Food choice considerations among American Indians living in rural Oklahoma: The THRIVE study. Appetite 2018, 128, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Barr, T.L.; Reid, J.; Catska, P.; Varona, G.; Rout, M. Development of indigenous enterprise in a contemporary business environment—The Ngāi Tahu Ahikā approach. J. Enterp. Communities People Places Glob. Econ. 2018, 12, 454–471. [Google Scholar] [CrossRef]
- Reid, J.; Rout, M. Getting to know your food: The insights of indigenous thinking in food provenance. Agric. Hum. Values 2016, 33, 427–438. [Google Scholar] [CrossRef]
- Bodirsky, M.; Johnson, J. Decolonizing Diet: Healing by Reclaiming Traditional Indigenous Foodways. Cuizine J. Can. Food Cultures/Cuizine 2008, 1. [Google Scholar] [CrossRef]
- Figueroa-Helland, L.; Thomas, C.; Aguilera, A.P. Decolonizing Food Systems: Food Sovereignty, Indigenous Revitalization, and Agroecology as Counter-Hegemonic Movements. Perspect. Glob. Dev. Technol. 2018, 17, 173–201. [Google Scholar] [CrossRef]
- QIA. Food Sovereignty and Harvesting; Qikiqtani Inuit Association: Iqaluit, NU, Canada, 2019; pp. 1–24. [Google Scholar]
- Grey, S.; Newman, L. Beyond culinary colonialism: Indigenous food sovereignty, liberal multiculturalism, and the control of gastronomic capital. Agric. Hum. Values 2018, 35, 717–730. [Google Scholar] [CrossRef]
- Kuhnlein, H.; Erasmus, B.; Creed-Kanashiro, H.M.; Englberger, L.; Okeke, C.; Turner, N.; Allen, L.; Bhattacharjee, L. Indigenous peoples’ food systems for health: Finding interventions that work. Public Health Nutr. 2007, 9, 1013–1019. [Google Scholar] [CrossRef] [Green Version]
- Egeland, G.M. Inuit Health Survey 2007–2008: Inuvialuit Settlement Region; Centre for Indigenous Peoples’ Nutrition and Environment (CINE): Montreal, QC, Canada, 2010. [Google Scholar]
- Egeland, G.M. Inuit Health Survey 2007–2008: Nunatsiavut; Centre for Indigenous Peoples’ Nutrition and Environment (CINE): Montreal, QC, Canada, 2010. [Google Scholar]
- Egeland, G.M. Inuit Health Survey 2007–2008: Nunavut; Centre for Indigenous Peoples’ Nutrition and Environment (CINE): Montreal, QC, Canada, 2010. [Google Scholar]
- Reyes-García, V.; Powell, B.; Díaz-Reviriego, I.; Fernández-Llamazares, Á.; Gallois, S.; Gueze, M. Dietary transitions among three contemporary hunter-gatherers across the tropics. Food Secur. 2019, 11, 109–122. [Google Scholar] [CrossRef] [Green Version]
- Batal, M.; Johnson-Down, L.; Moubarac, J.-C.; Ing, A.; Fediuk, K.; Sadik, T.; Tikhonov, C.; Chan, L.; Willows, N. Quantifying associations of the dietary share of ultra-processed foods with overall diet quality in First Nations peoples in the Canadian provinces of British Columbia, Alberta, Manitoba and Ontario. Public Health Nutr. 2017, 21, 103–113. [Google Scholar] [CrossRef] [Green Version]
- First Nations Development Institute. Indian Country Food Price Index: Exploring Variation in Food Pricing Across Native Communities—A Working Paper; First Nations Development Institute: Fredericksburg, VA, USA, 2016; pp. 1–14. [Google Scholar]
- First Nations Development Institute. Indian Country Food Price Index: Exploring Variation in Food Pricing Across Native Communities—A Working Paper II; First Nations Development Institute: Fredericksburg, VA, USA, 2018; pp. 1–41. [Google Scholar]
- Grégoire, G.; Derderian, F.; Le Lorier, J. Selecting the language of the publications included in a meta-analysis: Is there a tower of babel bias? J. Clin. Epidemiol. 1995, 48, 159–163. [Google Scholar] [CrossRef]
- Kumanyika, S.K. Unraveling common threads in obesity risk among racial/ethnic minority and migrant populations. Public Health 2019, 172, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Searles, N. To sell or not to sell: Country food markets and Inuit identity in Nunavut. Food Foodways 2016, 24, 194–212. [Google Scholar] [CrossRef]
- Ford, J.D.; Macdonald, J.P.; Huet, C.; Statham, S.; MacRury, A. Food policy in the Canadian North: Is there a role for country food markets? Soc. Sci. Med. 2016, 152, 35–40. [Google Scholar] [CrossRef]
- David-Chavez, D.M.; Gavin, M.C. A global assessment of Indigenous community engagement in climate research. Environ. Res. Lett. 2018, 13, 123005. [Google Scholar] [CrossRef]
- ITK. An Inuit-Specific Approach for the Canadian Food Policy; Inuit Tapiriit Kanatami (ITK): Ottawa, ON, Canada, 2017; pp. 1–40. [Google Scholar]
- ICC-Alaska. Alaskan Inuit food SECURITY Conceptual Framework: How to assess the Arctic from an Inuit Perspective; Inuit Circumpolar Council (ICC)-Alaska: Anchorage, AL, USA, 2015. [Google Scholar]
- Ferguson, M.; King, A.; Brimblecombe, J. Time for a shift in focus to improve food affordability for remote customers. Med. J. Aust. 2016, 204, 409. [Google Scholar] [CrossRef] [PubMed]





| Reference | Setting 1 | Methods | Outcomes Examined | Conclusion | Relationship to Food Supply and/or Health | ||
|---|---|---|---|---|---|---|---|
| Country | Geography | Empirical | Respondent-Based | ||||
| [66] | CA | Arctic and northern | Mapping | Survey of retail experience |
| There is limited retail competition in most communities which lack year-round road access | Respondents expressed concerns regarding food supply (availability, cost, quality and freshness) |
| [65] | USA | Not specified | Mapping | Interviews (Tribal members) |
| Lower density of healthy food outlets in tribal areas compared to nontribal areas | Respondents perceived food environment negatively and ported barriers to the acquisition of healthy food |
| [67] | CA | Rural | Asset mapping (youth) |
| Gas station and convenience store were the only place to purchase groceries in the community | Available food was perceived to be of poor quality and recommended that healthier food be sold | |
| [68] | USA | Rural; Urban | Inventorying (secondary data; ground-truthing / site visitation) |
| Secondary data sources both over- and under- estimate the food environment especially for nontraditional retailers | ||
| [71] | USA | Rural; Remote | Inventorying (secondary data; telephone survey) |
| General characteristics of available stores (on Navajo Nation and Border Towns) are reported | Navajo convenience stores offered fewer healthier food options compared to Navajo supermarket | |
| [72] | Guam | Island | On site observations |
| The majority of stores within a mile from participants were small markets | Living near a small market was negatively correlated with body mass index (BMI); while living near a convenience store was positively correlated | |
| [73] | USA | Not specified | Inventorying (secondary data; telephone survey; site visitation) |
| Half of stores identified on 22 American Indian reservations were convenience stores. A total of 17 reservations did not have a supermarket on their reservation, and the nearest off-reservation supermarket was 10 miles from the tribe’s headquarters | Across all stores, about 38% of checklist items were available, with foods from the dairy and sugars/sweets groups being the most available, while fresh fruits/vegetables being the least available. Cost of the most commonly available items was lowest in supermarkets | |
| [69] | CA | Urban | Mapping (census and store location data) |
| Supermarket exposure did not differ in neighborhoods with a higher percentage of Indigenous residents | ||
| [70] | CA | General/National | Internet search |
| In total, 42 Indigenous food co-ops were identified (notably in northern Canada) | ||
| Dimension | Research Gaps and/or Challenge | Proposed Research Needs and/or Future Directions |
|---|---|---|
| Country |
|
|
| Geographic and populational setting |
|
|
| Temporal |
|
|
| Research approach and study design |
|
|
| Research tools |
|
|
| Domains of the food sector assessed |
|
|
| Food items included |
|
|
| Contextual factors |
|
|
| Equity informed methods |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kenny, T.-A.; Little, M.; Lemieux, T.; Griffin, P.J.; Wesche, S.D.; Ota, Y.; Batal, M.; Chan, H.M.; Lemire, M. The Retail Food Sector and Indigenous Peoples in High-Income Countries: A Systematic Scoping Review. Int. J. Environ. Res. Public Health 2020, 17, 8818. https://doi.org/10.3390/ijerph17238818
Kenny T-A, Little M, Lemieux T, Griffin PJ, Wesche SD, Ota Y, Batal M, Chan HM, Lemire M. The Retail Food Sector and Indigenous Peoples in High-Income Countries: A Systematic Scoping Review. International Journal of Environmental Research and Public Health. 2020; 17(23):8818. https://doi.org/10.3390/ijerph17238818
Chicago/Turabian StyleKenny, Tiff-Annie, Matthew Little, Tad Lemieux, P. Joshua Griffin, Sonia D. Wesche, Yoshitaka Ota, Malek Batal, Hing Man Chan, and Melanie Lemire. 2020. "The Retail Food Sector and Indigenous Peoples in High-Income Countries: A Systematic Scoping Review" International Journal of Environmental Research and Public Health 17, no. 23: 8818. https://doi.org/10.3390/ijerph17238818