Running and Physical Activity in an Air-Polluted Environment: The Biomechanical and Musculoskeletal Protocol for a Prospective Cohort Study 4HAIE (Healthy Aging in Industrial Environment—Program 4)

 , , , , ,
, , , , ,  , ,
, , 
 ,
,  and
and
Abstract
:1. Introduction
2. Material and Methods
2.1. Design
2.1.1. Inclusion Criteria for Active Runners
2.1.2. Inclusion Criteria for Inactive Controls
2.1.3. Exclusion Criteria
2.2. Experimental Set-Up
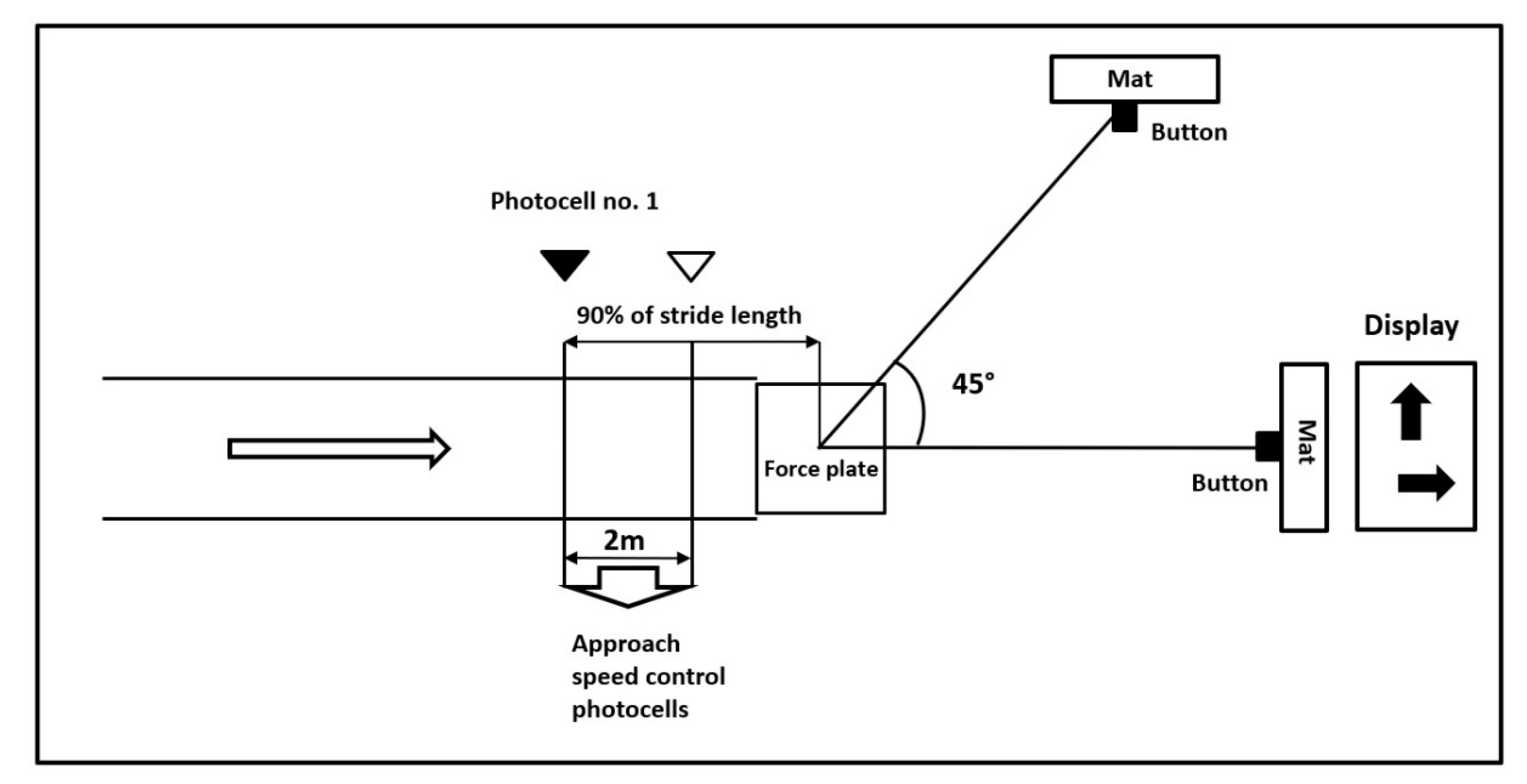
2.2.1. Biomechanical Set-Up
2.2.2. Magnetic Resonance Imaging Set-Up
2.3. Protocol
2.3.1. Global 4HAIE Protocol and Interactions
2.3.2. Biomechanical Protocol
2.3.3. Magnetic Resonance Imaging Protocol
2.3.4. Functional Testing Protocol
2.4. Data Analysis
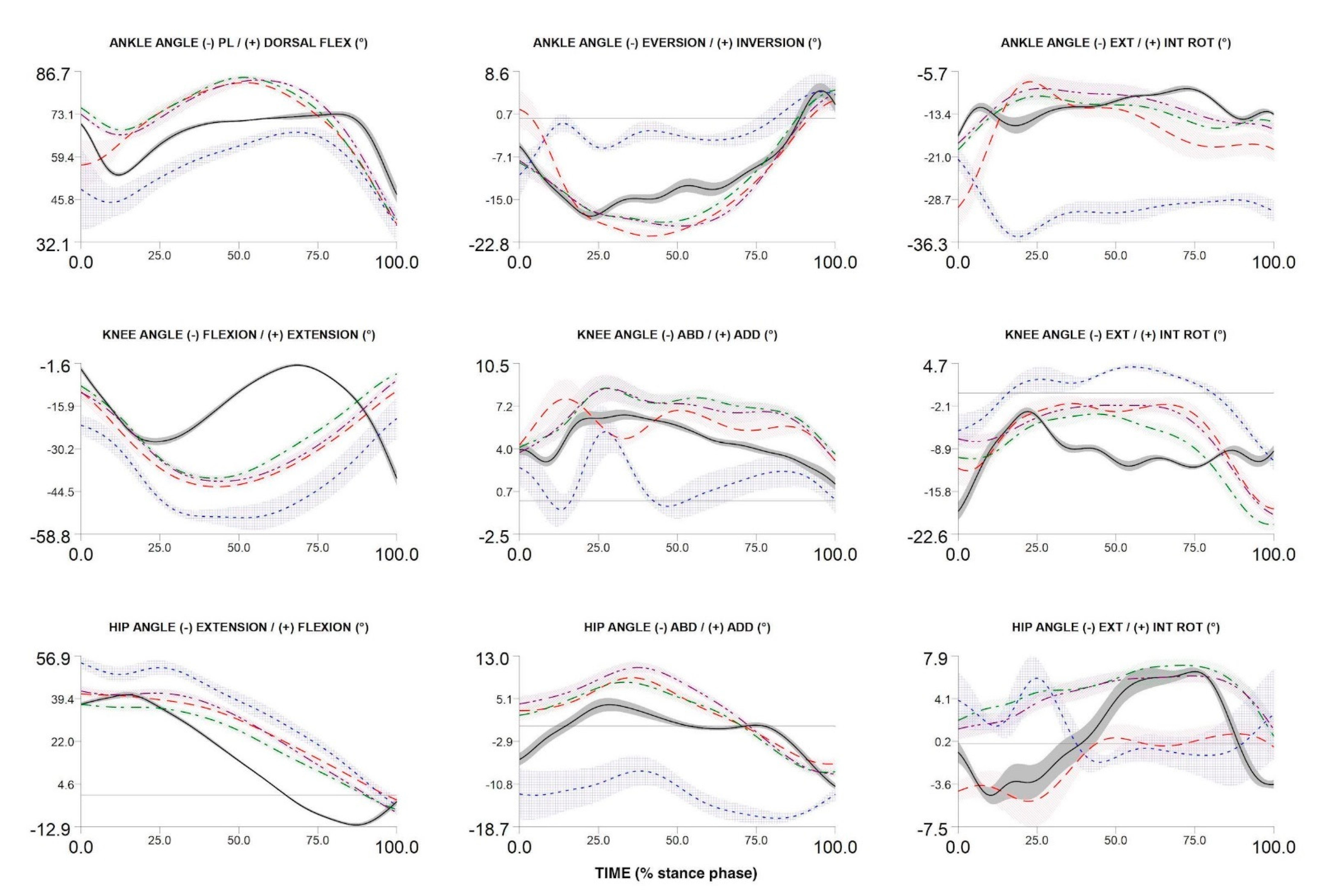
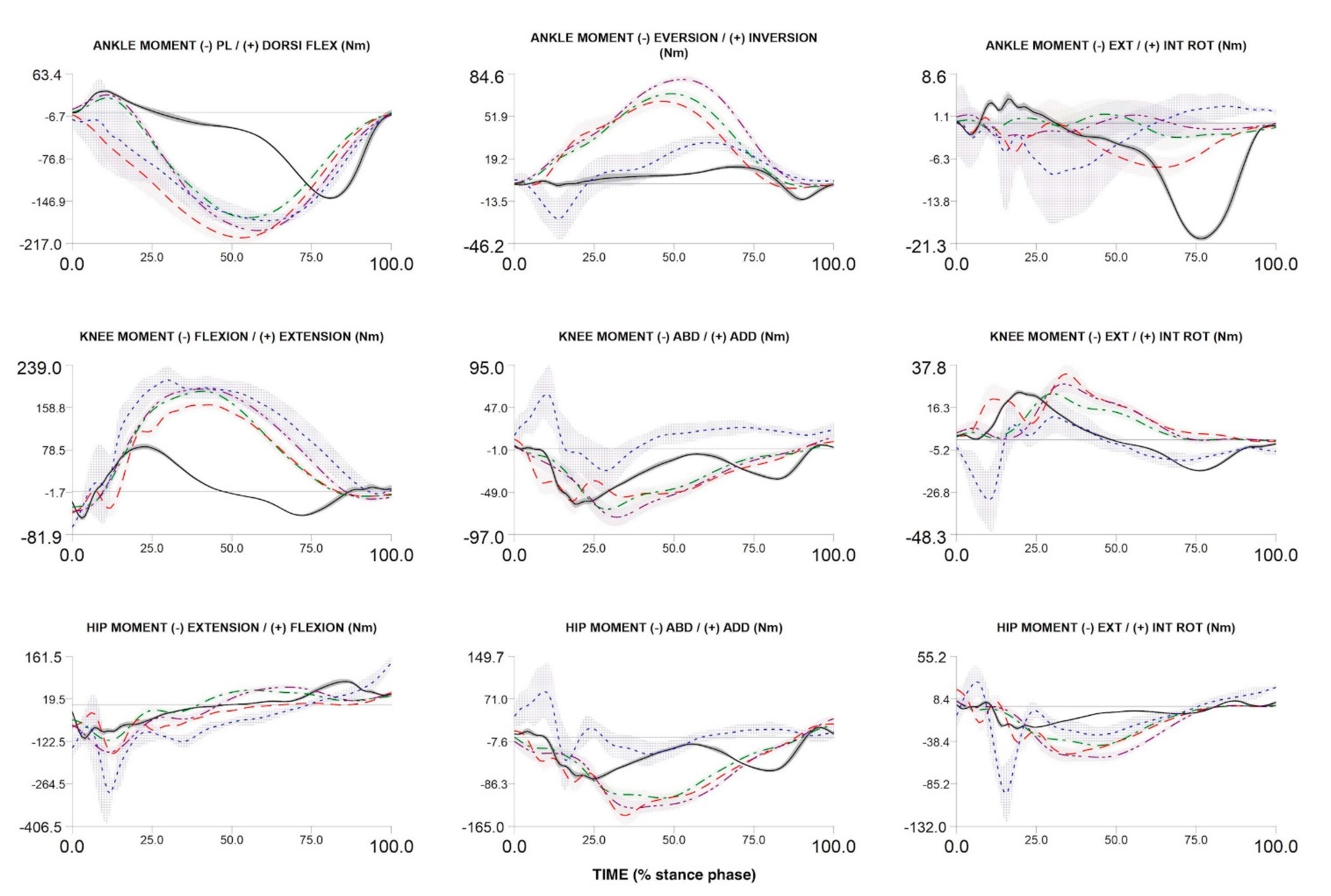
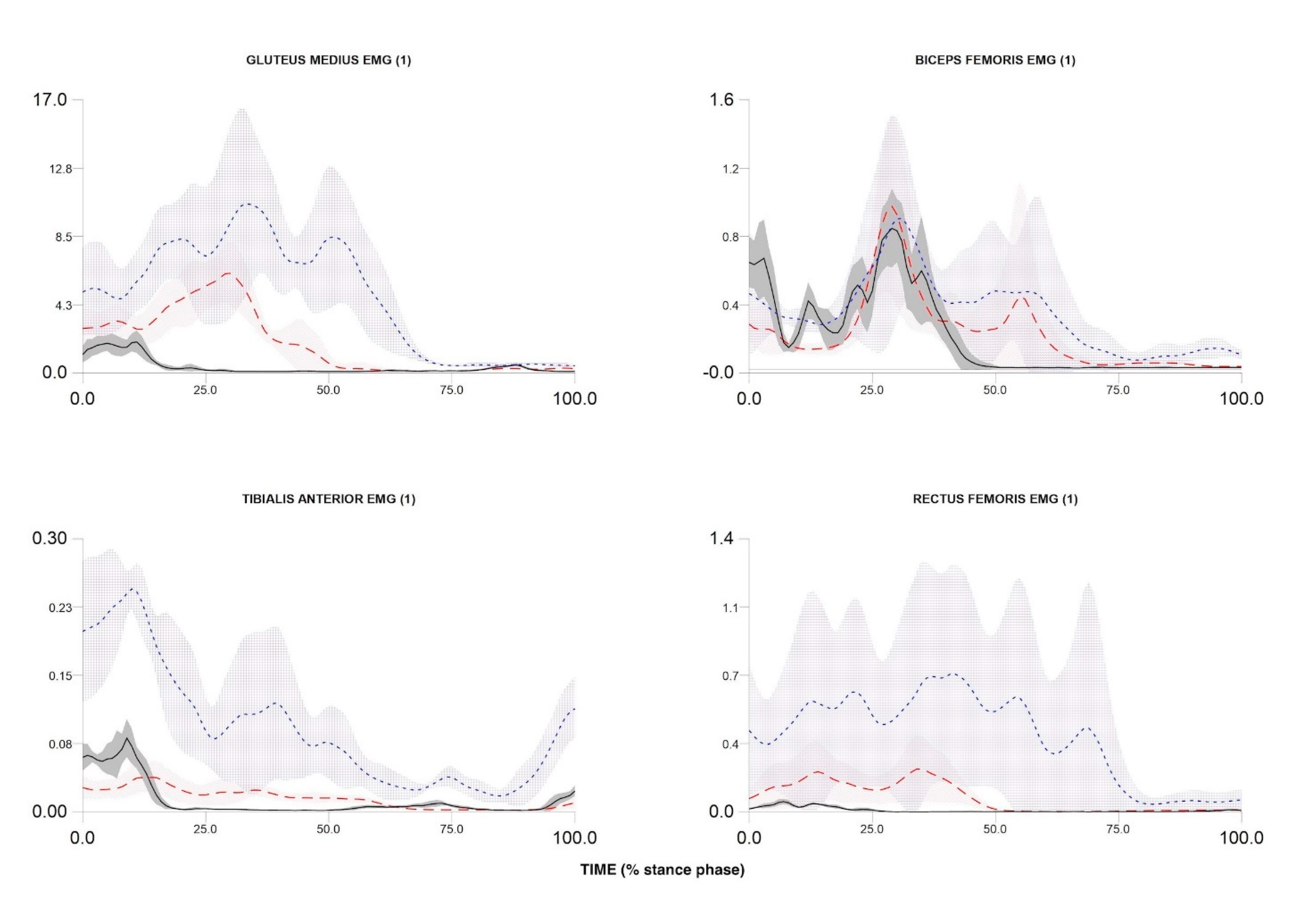
2.4.1. Biomechanics Data Analysis
2.4.2. Magnetic Resonance Imaging Data Analysis
3. Recruitment and Data Example
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Briggs, A.M.; Cross, M.J.; Hoy, D.G.; Sànchez-Riera, L.; Blyth, F.M.; Woolf, A.D.; March, L. Musculoskeletal Health Conditions Represent a Global Threat to Healthy Aging: A Report for the 2015 World Health Organization World Report on Ageing and Health. Gerontologist 2016, 56, S243–S255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Briggs, A.M.; Woolf, A.D.; Dreinhöfer, K.; Homb, N.; Hoy, D.G.; Kopansky-Giles, D.; Åkesson, K.; March, L. Reducing the global burden of musculoskeletal conditions. Bull. World Health Organ. 2018, 96, 366–368. [Google Scholar]
- Shepherd, A.; Mullins, J.T. Arthritis diagnosis and early-life exposure to air pollution. Environ. Pollut. 2019, 253, 1030–1037. [Google Scholar] [CrossRef] [PubMed]
- Mueller, N.; Rojas-Rueda, D.; Cole-Hunter, T.; de Nazelle, A.; Dons, E.; Gerike, R.; Götschi, T.; Int Panis, L.; Kahlmeier, S.; Nieuwenhuijsen, M. Health impact assessment of active transportation: A systematic review. Prev. Med. 2015, 76, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Tainio, M.; de Nazelle, A.J.; Götschi, T.; Kahlmeier, S.; Rojas-Rueda, D.; Nieuwenhuijsen, M.J.; de Sá, T.H.; Kelly, P.; Woodcock, J. Can air pollution negate the health benefits of cycling and walking? Prev. Med. 2016, 87, 233–236. [Google Scholar] [CrossRef] [Green Version]
- Peng, K.T.; Liu, J.F.; Chiang, Y.C.; Chen, P.C.; Chiang, M.H.; Shih, H.N.; Chang, P.J.; Lee, C.W. Particulate matter exposure aggravates osteoarthritis severity. Clin. Sci. 2019, 133, 2171–2187. [Google Scholar] [CrossRef] [Green Version]
- Hart, J.E.; Laden, F.; Puett, R.C.; Costenbader, K.H.; Karlson, E.W. Exposure to traffic pollution and increased risk of rheumatoid arthritis. Environ. Health Perspect. 2009, 117, 1065–1069. [Google Scholar] [CrossRef] [Green Version]
- Chang, K.H.; Hsu, C.C.; Muo, C.H.; Hsu, C.Y.; Liu, H.C.; Kao, C.H.; Chen, C.Y.; Chang, M.Y.; Hsu, Y.C. Air pollution exposure increases the risk of rheumatoid arthritis: A longitudinal and nationwide study. Environ. Int. 2016, 94, 495–499. [Google Scholar] [CrossRef]
- Neogi, T. The Epidemioloy and Impact of Pain in Osteoarthritis. Osteoarthr. Cartil. 2014, 21, 1145–1153. [Google Scholar] [CrossRef] [Green Version]
- Chehab, E.F.; Favre, J.; Erhart-Hledik, J.C.; Andriacchi, T.P. Baseline knee adduction and flexion moments during walking are both associated with 5year cartilage changes in patients with medial knee osteoarthritis. Osteoarthr. Cartil. 2014, 22, 1833–1839. [Google Scholar] [CrossRef] [Green Version]
- Hart, H.F.; Birmingham, T.B.; Primeau, C.A.; Pinto, R.; Leitch, K.; Giffin, J.R. Associations between cadence and knee loading in patients with knee osteoarthritis. Arthritis Care Res. 2020, 1–10. [Google Scholar] [CrossRef]
- Lee, D.C.; Brellenthin, A.G.; Thompson, P.D.; Sui, X.; Lee, I.M.; Lavie, C.J. Running as a Key Lifestyle Medicine for Longevity. Prog. Cardiovasc. Dis. 2017, 60, 45–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Health Impact of Air Pollution; An expert report of the International Society for Environmental Epidemiology and the European Respiratory Society. Available online: http://www.youreventinfo.org/ISEE/Documents/HZ_Positionspapier_ENG_190318.pdf (accessed on 5 December 2020).
- Dai, S.; Carroll, D.D.; Watson, K.B.; Paul, P.; Carlson, S.A.; Fulton, J.E. Participation in Types of Physical Activities Among US Adults--National Health and Nutrition Examination Survey 1999–2006. J. Phys. Act. Health 2015, 12, S128–S140. [Google Scholar] [CrossRef] [PubMed]
- Lopes, A.D.; Hespanhol Júnior, L.C.; Yeung, S.S.; Costa, L.O.P. What are the main running-related musculoskeletal injuries? A Systematic Review. Sports Med. 2012, 42, 891–905. [Google Scholar] [CrossRef] [PubMed]
- Saragiotto, B.T.; Yamato, T.P.; Hespanhol Junior, L.C.; Rainbow, M.J.; Davis, I.S.; Lopes, A.D. What are the main risk factors for running-related injuries? Sports Med. 2014, 44, 1153–1163. [Google Scholar] [CrossRef] [PubMed]
- Bredeweg, S.W.; Kluitenberg, B.; Bessem, B.; Buist, I. Differences in kinetic variables between injured and noninjured novice runners: A prospective cohort study. J. Sci. Med. Sport 2013, 16, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Bredeweg, S.W.; Buist, I.; Kluitenberg, B. Differences in kinetic asymmetry between injured and noninjured novice runners: A prospective cohort study. Gait Posture 2013, 38, 847–852. [Google Scholar] [CrossRef]
- Hamill, J.; Miller, R.; Noehren, B.; Davis, I. A prospective study of iliotibial band strain in runners. Clin. Biomech. 2008, 23, 1018–1025. [Google Scholar] [CrossRef]
- Ceyssens, L.; Vanelderen, R.; Barton, C.; Malliaras, P.; Dingenen, B. Biomechanical Risk Factors Associated with Running-Related Injuries: A Systematic Review. Sport. Med. 2019, 49, 1095–1115. [Google Scholar] [CrossRef] [Green Version]
- Boden, B.P.; Dean, G.S.; Feagin, J.A.; Garrett, W.E. Mechanisms of anterior cruciate ligament injury. Orthopedics 2000, 23, 573–578. [Google Scholar] [CrossRef]
- Arendt, E.A.; Agel, J.; Dick, R. Anterior Cruciate Ligament Injury Patterns among Collegiate Men and Women. J. Athl. Train. 1999, 34, 86–92. [Google Scholar]
- Bjordal, J.M.; Arnøy, F.; Hannestad, B.; Strand, T. Epidemiology of anterior cruciate ligament injuries in soccer. Am. J. Sports Med. 1997, 25, 341–345. [Google Scholar] [CrossRef]
- Messina, D.F.; Farney, W.C.; DeLee, J.C. The incidence of injury in Texas high school basketball: A prospective study among male and female athletes. Am. J. Sports Med. 1999, 27, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Lively, M.W.; Fethers, C.C. Increasing Prevalence of Anterior Cruciate Ligament Injuries in a Collegiate Population. W. Va. Med. J. 2012, 108, 8–11. [Google Scholar]
- Lin, C.C.; Yang, S.K.; Lin, K.C.; Ho, W.C.; Hsieh, W.S.; Shu, B.C.; Chen, P.C. Multilevel analysis of air pollution and early childhood neurobehavioral development. Int. J. Environ. Res. Public Health 2014, 11, 6827–6841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.; Zhang, J.; Zeng, X.; Zeng, Y.; Wang, S.; Chen, S. Association of traffic-related air pollution with children’s neurobehavioral functions in Quanzhou, China. Environ. Health Perspect. 2009, 117, 1612–1618. [Google Scholar] [CrossRef] [Green Version]
- Swanik, C.B.; Covassin, T.; Stearne, D.J.; Schatz, P. The relationship between neurocognitive function and noncontact anterior cruciate ligament injuries. Am. J. Sports Med. 2007, 35, 943–948. [Google Scholar] [CrossRef]
- Hůnová, I. Ambient air quality in the czech republic: Past and present. Atmosphere 2020, 11, 214. [Google Scholar] [CrossRef] [Green Version]
- Sram, R.J.; Binkova, B.; Dostal, M.; Merkerova-Dostalova, M.; Libalova, H.; Milcova, A.; Rossner, P.; Rossnerova, A.; Schmuczerova, J.; Svecova, V.; et al. Health impact of air pollution to children. Int. J. Hyg. Environ. Health 2013, 216, 533–540. [Google Scholar] [CrossRef]
- Šrám, R.J.; Beneš, I.; Binková, B.; Dejmek, J.; Horstman, D.; Kotěšovec, F.; Otto, D.; Perreault, S.D.; Rubeš, J.; Selevan, S.G.; et al. Teplice Program—The impact of air pollution on human health. Environ. Health Perspect. 1996, 104, 699–714. [Google Scholar] [CrossRef] [Green Version]
- CSO Czech Statistical Office. Available online: http://www.czso.cz/eng/redakce.nsf/i/bvz_ts (accessed on 1 December 2020).
- Air Quality Information System. Air Pollution in the Czech Republic 2018—Benzoapyren; CHMI: Prague, Czech Republic, 2018. [Google Scholar]
- WHO. Physical activity. Prim. Health Care 2003, 13, 1–8. [Google Scholar] [CrossRef]
- McClay, I.; Manal, K. Three-dimensional kinetic analysis of running: Significance of secondary planes of motion. Med. Sci. Sport. Exerc. 1999, 31, 1629–1637. [Google Scholar] [CrossRef] [PubMed]
- Portinaro, N.; Leardini, A.; Panou, A.; Monzani, V.; Caravaggi, P. Modifying the Rizzoli foot model to improve the diagnosis of pes-planus: Application to kinematics of feet in teenagers. J. Foot Ankle Res. 2014, 7, 754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leardini, A.; Benedetti, M.G.; Berti, L.; Bettinelli, D.; Nativo, R.; Giannini, S. Rear-foot, mid-foot and fore-foot motion during the stance phase of gait. Gait Posture 2007, 25, 453–462. [Google Scholar] [CrossRef] [PubMed]
- Samson, W.; Van Hamme, A.; Desroches, G.; Dohin, B.; Dumas, R.; Chèze, L. Biomechanical maturation of joint dynamics during early childhood: Updated conclusions. J. Biomech. 2013, 46, 2258–2263. [Google Scholar] [CrossRef] [PubMed]
- D’Août, K.; Pataky, T.C.; De Clercq, D.; Aerts, P. The effects of habitual footwear use: Foot shape and function in native barefoot walkers. Footwear Sci. 2009, 1, 81–94. [Google Scholar] [CrossRef]
- Hardcastle, P.; Nade, S. The significance of the Trendelenburg test. J. Bone Jt. Surg.Ser. B 1985, 67, 741–746. [Google Scholar] [CrossRef] [PubMed]
- Youdas, J.W.; Mraz, S.T.; Norstad, B.J.; Schinke, J.J.; Hollman, J.H. Determining meaningful changes in pelvic-on-femoral position during the trendelenburg test. J. Sport Rehabil. 2007, 16, 326–335. [Google Scholar] [CrossRef] [PubMed]
- Makhmalbaf, H.; Moradi, A.; Ganji, S.; Omidi-Kashani, F. Accuracy of lachman and anterior drawer tests. Arch Bone Jt. Surg. 2013, 94, 94–97. [Google Scholar] [CrossRef]
- Sun, K.; Tian, S.; Zhang, J.; Xia, C.; Zhang, C.; Yu, T. Anterior cruciate ligament reconstruction with BPTB autograft, irradiated versus non-irradiated allograft: A prospective randomized clinical study. Knee Surg. Sport. Traumatol. Arthrosc. 2009, 17, 464–474. [Google Scholar] [CrossRef]
- Lee, K.T.; Park, Y.U.; Jegal, H.; Park, J.W.; Choi, J.P.; Kim, J.S. New method of diagnosis for chronic ankle instability: Comparison of manual anterior drawer test, stress radiography and stress ultrasound. Knee Surg. Sport. Traumatol. Arthrosc. 2014, 22, 1701–1707. [Google Scholar] [CrossRef]
- Vicenzino, B.; Branjerdporn, M.; Teys, P.; Jordan, K. Initial changes in posterior talar glide and dorsiflexion of the ankle after mobilization with movement in individuals with recurrent ankle sprain. J. Orthop. Sports Phys. Ther. 2006, 36, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, M.; Schrader, J.; Applegate, T.; Koceja, D. Unilateral postural control of the functionally dominant and nondominant extremities of healthy subjects. J. Athl. Train. 1998, 33, 319–322. [Google Scholar] [PubMed]
- Stanhope, S.J.; Kepple, T.M.; McGuire, D.; Roman, N.L. Kinematic-based technique for event time determination during gait. Med. Biol. Eng. Comput. 1990, 28, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Jandacka, D.; Plesek, J.; Skypala, J.; Uchytil, J.; Silvernail, J.F.; Hamill, J. Knee Joint Kinematics and Kinetics During Walking and Running After Surgical Achilles Tendon Repair. Orthop. J. Sport. Med. 2018, 6, 232596711877986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weir, G.; van Emmerik, R.; Jewell, C.; Hamill, J. Coordination and variability during anticipated and unanticipated sidestepping. Gait Posture 2019, 67, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Gruber, A.H.; Silvernail, J.F.; Brueggemann, P.; Rohr, E.; Hamill, J. Footfall patterns during barefoot running on harder and softer surfaces. Footwear Sci. 2013, 5, 39–44. [Google Scholar] [CrossRef]
- Dixon, P.C.; Böhm, H.; Döderlein, L. Ankle and midfoot kinetics during normal gait: A multi-segment approach. J. Biomech. 2012, 45, 1011–1016. [Google Scholar] [CrossRef]
- Hamill, J.; Selbie, W.; Kepple, T. Three-dimensional Kinematics. In Research Methods in Biomechanics; Robertson, D., Caldwell, G., Hamill, J., Kamen, G., Whittlesey, S., Eds.; Human Kinetics: Champaign, IL, USA, 2013; pp. 35–60. [Google Scholar]
- Robertson, D.G.E.; Caldwell, G.E.; Hamill, J.; Kamen, G.; Whittlesey, S.N. Research Methods in Biomechanics, 2nd ed.; Human Kinetics: Champaign, IL, USA, 2014; ISBN 0-7360-9340-0. [Google Scholar]
- Yong, J.R.; Silder, A.; Delp, S.L. Differences in muscle activity between natural forefoot and rearfoot strikers during running. J. Biomech. 2014, 47, 3593–3597. [Google Scholar] [CrossRef] [Green Version]
- Hayes, C.W.; Conway, W.F. Evaluation of articular cartilage: Radiographic and cross-sectional imaging techniques. Radiographics 1992, 12, 409–428. [Google Scholar] [CrossRef] [Green Version]
- Cameron, M.L.; Briggs, K.K.; Steadman, J.R. Reproducibility and reliability of the outerbridge classification for grading chondral lesions of the knee arthroscopically. Am. J. Sports Med. 2003, 31, 83–86. [Google Scholar] [CrossRef]
- Jack, C.M.; Rajaratnam, S.S.; Khan, H.O.; Keast-Butler, O.; Butler-Manuel, P.A.; Heatley, F.W. The modified tibial tubercle osteotomy for anterior knee pain due to chondromalacia patellae in adults. Bone Joint Res. 2012, 1, 167–173. [Google Scholar] [CrossRef]
- Jungius, K.-P.; Schmid, M.R.; Zanetti, M.; Hodler, J.; Koch, P.; Pfirrmann, C.W.A. Cartilaginous Defects of the Femorotibial Joint:Accuracy of Coronal Short Inversion Time Inversion-Recovery MR Sequence. Radiol. Clin. N. Am. 2006, 240, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Araujo, P.; van Eck, C.F.; Torabi, M.; Fu, F.H. How to optimize the use of MRI in anatomic ACL reconstruction. Knee Surgery Sport. Traumatol. Arthrosc. 2013, 21, 1495–1501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, S.H.; Choi, J.-Y.; Lee, G.K.; Choi, J.-A.; Chung, H.W.; Kang, H.S. Grading of Anterior Cruciate Ligament Injury. J. Comput. Assist. Tomogr. 2003, 27, 814–819. [Google Scholar] [CrossRef] [PubMed]
- Apprich, S.; Friedrich, K.; Veronika, S. Siegfried Trattnig VIMATS—Vienna Morphological Achilles Tendon Score Target Audience. Proc. Intl. Soc. Mag. Reson. Med. 2013, 14, 3472. [Google Scholar]
- Casula, V.; Hirvasniemi, J.; Lehenkari, P.; Ojala, R.; Haapea, M.; Saarakkala, S.; Lammentausta, E.; Nieminen, M.T. Association between quantitative MRI and ICRS arthroscopic grading of articular cartilage. Knee Surg. Sport. Traumatol. Arthrosc. 2016, 24, 2046–2054. [Google Scholar] [CrossRef] [Green Version]
- Casula, V.; Nissi, M.J.; Podlipská, J.; Haapea, M.; Koski, J.M.; Saarakkala, S.; Guermazi, A.; Lammentausta, E.; Nieminen, M.T. Elevated adiabatic T1ρ and T2ρ in articular cartilage are associated with cartilage and bone lesions in early osteoarthritis: A preliminary study. J. Magn. Reson. Imaging 2017, 46, 678–689. [Google Scholar] [CrossRef] [Green Version]
- Juras, V.; Apprich, S.; Szomolanyi, P.; Bieri, O.; Deligianni, X.; Trattnig, S. Bi-exponential T2* analysis of healthy and diseased Achilles tendons: An in vivo preliminary magnetic resonance study and correlation with clinical score. Eur. Radiol. 2013, 23, 2814–2822. [Google Scholar] [CrossRef] [Green Version]
- Herzog, W. The problem with running injuries. J. Sport Heal. Sci. 2016, 5, 171. [Google Scholar] [CrossRef]
- Novacheck, T.F. The biomechanics of running. Gait Posture 1998, 7, 77–95. [Google Scholar] [CrossRef]
- Vanrenterghem, J.; Venables, E.; Pataky, T.; Robinson, M.A. The effect of running speed on knee mechanical loading in females during side cutting. J. Biomech. 2012, 45, 2444–2449. [Google Scholar] [CrossRef] [PubMed]
- Pollard, C.D.; Davis, I.M.; Hamill, J. Influence of gender on hip and knee mechanics during a randomly cued cutting maneuver. Clin. Biomech. 2004, 19, 1022–1031. [Google Scholar] [CrossRef] [PubMed]
- McClay, I.; Manal, K. A comparison of three-dimensional lower extremity kinematics during running between excessive pronators and normals. Clin. Biomech. 1998, 13, 195–203. [Google Scholar] [CrossRef]
- Rautiainen, J.; Nissi, M.J.; Salo, E.N.; Tiitu, V.; Finnilä, M.A.J.; Aho, O.M.; Saarakkala, S.; Lehenkari, P.; Ellermann, J.; Nieminen, M.T. Multiparametric MRI assessment of human articular cartilage degeneration: Correlation with quantitative histology and mechanical properties. Magn. Reson. Med. 2015, 74, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Ma, C.B.; Link, T.M.; Castillo, D.; Blumenkrantz, G.; Lozano, J.; Carballido-gamio, J. In vivo t1rho and t2 mapping of articular cartilage in osteoarthritis of the knee using 3 tesla mri. Osteoarthr. Cartil. 2007, 15, 789–797. [Google Scholar] [CrossRef] [Green Version]
- Nieminen, M.T.; Casula, V.; Nevalainen, M.T.; Saarakkala, S. Osteoarthritis year in review 2018: Imaging. Osteoarthr. Cartil. 2019, 27, 401–411. [Google Scholar] [CrossRef] [Green Version]
- Schmitz, J.R.; Wang, H.; Kraft, A.R.; Shultz, J.S.; Ross, E.S.; Henson, A.R.; Perrin, H.D. Regional differences in anterior cruciate ligament imaging biomarkers: T2 and T2 star values. Muscles. Ligaments Tendons J. 2018, 8, 238–245. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Imaging Parameter | Axial PD TSE FS | Coronal PD TSE FS | Sagittal PD TSE FS | Coronal T1 TSE | 3D DESS WE | Sagittal T2 Map Cartilage | Sagittal T2 Map ACL | 3D PC MRA |
|---|---|---|---|---|---|---|---|---|
| Repetition time (ms) | 4510 | 5760 | 4250 | 490 | 18 | 1690 | 1500 | 117 |
| Echo time (ms) | 27 | 25 | 26 | 12 | 7.05 | 12, 24, 36, 48, 60 | 12, 24, 36, 48, 60 | 18.7 |
| Slice thickness (mm) | 3 | 3 | 3 | 3.2 | 0.6 | 3 | 3 | 1.1 |
| Field of view (mm) | 150 | 160 | 160 | 160 | 150 | 160 | 160 | 220 |
| Matrix size | 198 × 256 | 235 × 320 | 212 × 320 | 223 × 320 | 230 × 256 | 256 × 256 | 256 × 256 | 144 × 256 |
| Flip angle (°) | 150 | 150 | 150 | 150 | 25 | 180 | 180 | 15 |
| Inter-section gap (mm) | 0.3 | 0.3 | 0.3 | 0.6 | 0.1 | 0.6 | 0.6 | 0.2 |
| Bandwidth (kHz) | 140 | 145 | 140 | 150 | 260 | 230 | 225 | 320 |
| Echo train length | 8 | 10 | 8 | 2 | 2 | 5 | 5 | 0 |
| Signal average | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Number of slices | 30 | 35 | 30 | 28 | 160 | 18 | 5 | 80 |
| Acquisition time (min:s) | 2:08 | 2:08 | 2:09 | 1:36 | 3:41 | 3:55 | 3:29 | 6:33 |
| Imaging Parameter | Axial T2 TSE | Sagittal T1 SE | Coronal T1 TSE | Sagittal PD TSE FS | Axial PD TSE FS | Sagittal T2* Map Short | Sagittal T2* Map Long |
|---|---|---|---|---|---|---|---|
| Repetition time (ms) | 4000 | 555 | 610 | 4620 | 5200 | 485 | 485 |
| Echo time (ms) | 61 | 22 | 11 | 39 | 36 | 3.78, 0.77, 17.15, 23.52, 29.89 | 7.28, 14.28, 21.28, 28.28, 35.28 |
| Slice thickness (mm) | 3 | 3 | 3 | 3 | 3 | 3 | 3 |
| Field of view (mm) | 160 | 410 | 160 | 160 | 135 | 160 | 160 |
| Matrix size | 156 × 196 | 448 × 448 | 180 × 320 | 240 × 320 | 230 × 256 | 205 × 256 | 205 × 256 |
| Flip angle (°) | 150 | 90 | 150 | 150 | 150 | 60 | 60 |
| Inter-section gap (mm) | 0.6 | 0.6 | 0.6 | 0.6 | 1 | 0.6 | 0.6 |
| Bandwidth (kHz) | 210 | 190 | 190 | 200 | 220 | 415 | 415 |
| Echo train length | 12 | 1 | 3 | 12 | 10 | 5 | 5 |
| Signal average | 1 | 1 | 1 | 1 | 1 | 2 | 2 |
| Number of slices | 26 | 18 | 28 | 25 | 35 | 11 | 11 |
| Acquisition time (min:s) | 0:58 | 6:27 | 1:23 | 1:25 | 2:17 | 3:20 | 3:20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jandacka, D.; Uchytil, J.; Zahradnik, D.; Farana, R.; Vilimek, D.; Skypala, J.; Urbaczka, J.; Plesek, J.; Motyka, A.; Blaschova, D.; et al. Running and Physical Activity in an Air-Polluted Environment: The Biomechanical and Musculoskeletal Protocol for a Prospective Cohort Study 4HAIE (Healthy Aging in Industrial Environment—Program 4). Int. J. Environ. Res. Public Health 2020, 17, 9142. https://doi.org/10.3390/ijerph17239142
Jandacka D, Uchytil J, Zahradnik D, Farana R, Vilimek D, Skypala J, Urbaczka J, Plesek J, Motyka A, Blaschova D, et al. Running and Physical Activity in an Air-Polluted Environment: The Biomechanical and Musculoskeletal Protocol for a Prospective Cohort Study 4HAIE (Healthy Aging in Industrial Environment—Program 4). International Journal of Environmental Research and Public Health. 2020; 17(23):9142. https://doi.org/10.3390/ijerph17239142
Chicago/Turabian StyleJandacka, Daniel, Jaroslav Uchytil, David Zahradnik, Roman Farana, Dominik Vilimek, Jiri Skypala, Jan Urbaczka, Jan Plesek, Adam Motyka, Denisa Blaschova, and et al. 2020. "Running and Physical Activity in an Air-Polluted Environment: The Biomechanical and Musculoskeletal Protocol for a Prospective Cohort Study 4HAIE (Healthy Aging in Industrial Environment—Program 4)" International Journal of Environmental Research and Public Health 17, no. 23: 9142. https://doi.org/10.3390/ijerph17239142
APA StyleJandacka, D., Uchytil, J., Zahradnik, D., Farana, R., Vilimek, D., Skypala, J., Urbaczka, J., Plesek, J., Motyka, A., Blaschova, D., Beinhauerova, G., Rygelova, M., Brtva, P., Balazova, K., Horka, V., Malus, J., Silvernail, J. F., Irwin, G., Nieminen, M. T., ... Hamill, J. (2020). Running and Physical Activity in an Air-Polluted Environment: The Biomechanical and Musculoskeletal Protocol for a Prospective Cohort Study 4HAIE (Healthy Aging in Industrial Environment—Program 4). International Journal of Environmental Research and Public Health, 17(23), 9142. https://doi.org/10.3390/ijerph17239142