The Role of Emotional Intelligence and Sociocultural Adjustment on Migrants’ Self-reported Mental Well-Being in Spain: A 14 Month Follow-Up Study

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Instruments
3. Results
3.1. Descriptive Analyses
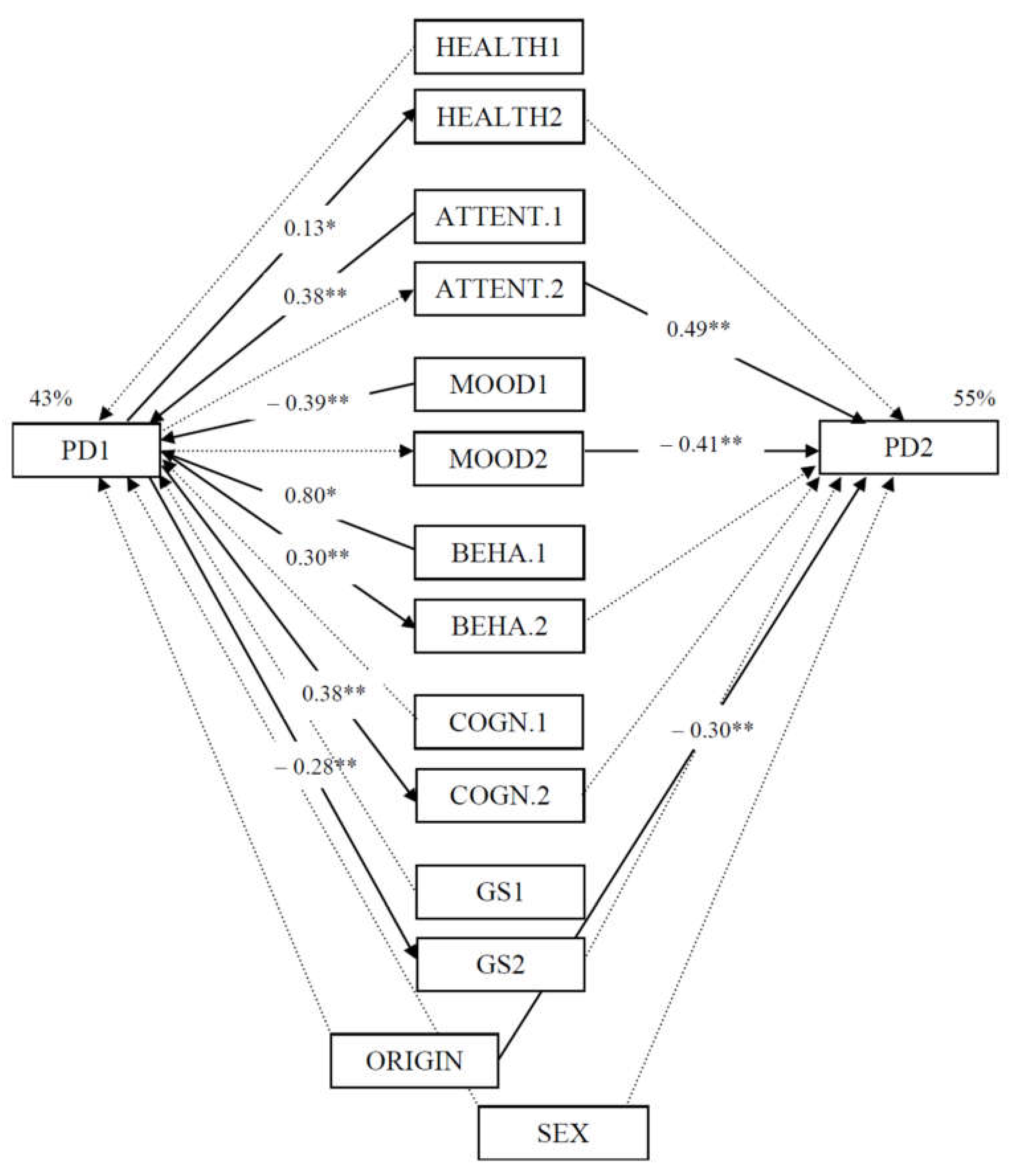
3.2. Model Testing
4. Discussion
5. Conclusion
5.1. Limitations
5.2. Main Contributions
Author Contributions
Funding
Conflicts of Interest
References
- United Nations. International Migration Report; Department of Economic and Social Affairs, Population Division, United Nations: New York, NY, USA, 2017. [Google Scholar]
- Moyce, S.C.; Schenker, M. Migrant Workers and Their Occupational Health and Safety. Annu. Rev. Public Health 2018, 39, 351–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- UNODC. Combating Violence against Migrants. Available online: https://www.unodc.org/documents/justice-and-prison-reform/UNODC_Combating_Violence_against_Migrants.pdf (accessed on 25 July 2019).
- World Health Organization—Europe. Mental Health: Fact Sheet; WHO Regional Office for Europe: Copenhagen, Denmark, 2019; Available online: http://www.euro.who.int/__data/assets/pdf_file/0004/404851/MNH_FactSheet_ENG.pdf?ua=1 (accessed on 7 January 2020).
- National Alliance on Mental Illness. Mental Health by the Numbers. 2020. Available online: https://www.nami.org/learn-more/mental-health-by-the-numbers (accessed on 6 January 2020).
- Berry, J.W.; Phinney, J.S.; Sam, D.L.; Vedder, P.; Berry, J.W.; Phinney, J.S.; Sam, D.L.; Vedder, P. Immigrant youth: Acculturation, identity and adaptation. Appl. Psychol. 2006, 55, 303–332. [Google Scholar] [CrossRef] [Green Version]
- Archuleta, A.J.; Lakhwan, M. Balancing cultures: Acculturation, environmental mastery, emotional regulation, and depressive symptoms among first-generation Latino/a youth. Soc. Work Ment. Health 2016, 14, 271–291. [Google Scholar] [CrossRef]
- Lecerof, S.S.; Stafstrom, M.; Westerling, R.; Östergren, P.-O. Does social capital protect mental health among migrants in Sweden? Health Promot. Int. 2015, 31, 644–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourque, F.I.; van der Ven, E.; Malla, A. A meta-analysis of the risk for psychotic disorders among first- and second-generation immigrants. Psychol. Med. 2011, 41, 897–910. [Google Scholar] [CrossRef]
- Yoon, E.; Chang, C.T.; Kim, S.; Clawson, A.; Cleary, S.E.; Hansen, M.; Bruner, J.P.; Chan, T.; Gomes, A.M. A meta-analysis of acculturation/enculturation and mental health. J. Couns. Psychol. 2013, 60, 15–30. [Google Scholar] [CrossRef]
- Bobowik, M.; Basabe, N.; Páez, D. The bright side of migration: Hedonic, psychological, and social well-being in immigrants in Spain. Soc. Sci. Res. 2015, 51, 189–204. [Google Scholar] [CrossRef]
- Ronda-Pérez, E.; Martínez, J.M.; Reid, A.; Agudelo-Suárez, A.A. Longer Residence of Ecuadorian and Colombian Migrant Workers in Spain Associated with New Episodes of Common Mental Disorders. Int. J. Environ. Res. Public Health 2019, 16, 2027. [Google Scholar] [CrossRef] [Green Version]
- Rudmin, F. Constructs, measurements and models of acculturation and acculturative stress. Int. J. Intercult. Relat. 2009, 33, 106–123. [Google Scholar] [CrossRef]
- Scheffran, J.; Marmer, E.; Sow, P. Migration as a contribution to resilience and innovation in climate adaptation: Social networks and co-development in Northwest Africa. Appl. Geogr. 2012, 33, 119–127. [Google Scholar] [CrossRef]
- Ward, C.; Bochner, S.; Furnham, A. The Psychology of Culture Shock; Routledge: Hove, UK, 2001. [Google Scholar]
- Gonidakis, F.; Korakakis, P.; Ploumpidis, D.; Karapavlou, D.A.; Rogakou, E.; Madianos, M.G. The relationship between acculturation factors and symptoms of depression: A cross-sectional study with immigrants living in Athens. Transcult. Psychiatry 2011, 48, 437–454. [Google Scholar] [CrossRef] [PubMed]
- Ward, C.; Kennedy, A. The measurement of sociocultural adaptation. Int. J. Intercult. Relat. 1999, 23, 659–677. [Google Scholar] [CrossRef]
- Schneeberger, A.R.; Seixas, A.; Schweinfurth, N.; Lang, U.E.; Cajochen, C.; Bux, D.A.; Richards, S.; Jean-Louis, G.; Huber, C.G. Differences in Insomnia Symptoms between Immigrants and Non-Immigrants in Switzerland attributed to Emotional Distress: Analysis of the Swiss Health Survey. Int. J. Environ. Res. Public Health 2019, 16, 289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Leersnyder, J.; Mesquita, B.; Kim, M.S. Where do my emotions belong? A study of emotional acculturation. Personal. Soc. Psychol. Bull. 2011, 37, 451–463. [Google Scholar] [CrossRef] [Green Version]
- Mayer, J.D.; Salovey, P. What is emotional intelligence? In Emotional Development and Emotional Intelligence: Implications for Educator; Salovey, P., Sluyter, D., Eds.; Basic Books: New York, NY, USA, 1997; pp. 3–31. [Google Scholar]
- Salovey, P.; Grewal, D. The science of emotional intelligence. Curr. Dir. Psychol. Sci. 2005, 14, 281–285. [Google Scholar] [CrossRef]
- Singh, Y.; Sharma, R. Relationship between general intelligence, emotional intelligence, stress levels and stress reactivity. Ann. Neurosci. 2012, 19, 107–111. [Google Scholar] [CrossRef] [Green Version]
- Baudry, A.S.; Grynberg, D.; Dassonneville, C.; Lelorain, S.; Christophe, V. Sub-dimensions of trait emotional intelligence and health: A critical and systematic review of the literature. Scand. J. Psychol. 2018, 59, 206–222. [Google Scholar] [CrossRef]
- Schutte, N.; Malouff, J.; Thorsteinsson, E.; Bhullar, N.; Rooke, S. A meta-analytic investigation of the relationship between emotional intelligence and health. Personal. Individ. Differ. 2007, 42, 921–933. [Google Scholar] [CrossRef]
- Fernández-Berrocal, P.; Salovey, P.; Vera, A.; Extremera, N.; Ramos, N. Cultural influences on the relation between perceived emotional intelligence and depression. Int. Rev. Soc. Psychol. 2005, 18, 91–107. [Google Scholar]
- Ekermans, G. Emotional intelligence across cultures: Theoretical and methodological considerations. In Assessing Emotional Intelligence; Parker, J.D.A., Saklofske, D.H., Stough, C., Eds.; Springer: Heidelberg, Germany, 2009; pp. 259–290. [Google Scholar]
- Schmitz, P.G.; Schmitz, F. Inteligencia emocional y aculturación (Emotional intelligence and acculturation). Psicol. Conduct. Behav. Psychol. 2012, 20, 15–41. [Google Scholar]
- Lopez-Zafra, E.; El Ghoudani, K. The influence of culture of honor and emotional intelligence in the acculturation of Moroccan immigrant women. Span. J. Psychol. 2014, 17, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.K.; Humphrey, N. Emotional intelligence as a moderator of stressor-mental health relations in adolescence: Evidence for specificity. Personal. Individ. Differ. 2012, 52, 100–105. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.-C.; Chen, A.S.-Y.; Song, Y.-C. Does your intelligence help to survive in a foreign jungle? The effects of cultural intelligence and emotional intelligence on cross-cultural adjustment. Int. J. Intercult. Relat. 2012, 36, 541–552. [Google Scholar] [CrossRef]
- Salovey, P.; Mayer, J.D.; Goldman, S.L.; Turvey, C.; Palfai, T.P. Emotional attention, clarity, and repair: Exploring emotional intelligence using the trait meta-mood scale. In Emotion, Disclosure, and Health; Pennebaker, J.W., Ed.; American Psychological Association: Washington, DC, USA, 1995; pp. 125–154. [Google Scholar]
- Salguero, J.M.; Palomera, R.; Fernández-Berrocal, P. Perceived emotional intelligence as predictor of psychological adjustment in adolescents: A 1-year prospective study. Eur. J. Psychol. Educ. 2012, 27, 21–34. [Google Scholar] [CrossRef]
- Gohm, C.L.; Clore, G.L. Four latent traits of emotional experience and their involvement in well-being, coping, and attributional style. Cogn. Emot. 2002, 16, 495–518. [Google Scholar] [CrossRef]
- Shulman, T.; Hemenover, S. Is dispositional emotional intelligence synonymous with personality? Self Identity 2006, 5, 147–171. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística (National Statistics Institute). Cifras de Población a 1 de Enero de 2018 (Population Census 1 January 2018). Available online: http://www.ine.es/prensa/cp_2018_p.pdf (accessed on 25 March 2019).
- Biau, D.J.; Kernéis, S.; Porcher, R. The importance of sample size in the planning and interpretation of medical research. Clin. Orthop. Relat. Res. 2008, 466, 2282–2288. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, D.P. Manual of the General Health Questionnaire; NFER Publishing: Windsor, UK, 1978. [Google Scholar]
- Sánchez-López, M.P.; Dresch, V. The 12-Item General Health Questionnaire (GHQ-12): Reliability, external validity and factor structure in the Spanish population. Psicothema 2008, 20, 839–843. [Google Scholar]
- Aierdi, X.; Basabe, N.; Blanco, C.; Olega, J.A. Población Latinoamericana en la CAPV 2007 (Latinamerican Population in the Basque Autonomous Community 2007); Latinoamerikar biztanleria EAE-n 2001-Sintesia; Ikuspegi y UPV/EHU; Observatorio Vasco de Inmigración: Bilbao, Spain, 2008; Available online: www.ikuspegi.org/documentos/documentos_internos/pob_lat_2007_web.pdf (accessed on 14 December 2018).
- Fernández-Berrocal, P.; Extremera, N.; Ramos, N. Validity and reliability of the Spanish modified version of the Trait Meta-Mood Scale. Psychol. Rep. 2004, 94, 751–755. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Lockwood, C.M.; Hoffman, J.M.; West, S.G.; Sheets, V. A comparison of methods to test mediation and other intervening variable effects. Psychol. Methods 2002, 7, 83–104. [Google Scholar] [CrossRef]
- Arbuckle, J.L. Amos 6.0 User’s Guide; SPSS: Chicago, IL, USA, 2005. [Google Scholar]
- Byrne, B.M. Structural Equation Modelling with AMOS: Basic Concepts, Applications and Programming; Routledge: New York, NY, USA, 2009. [Google Scholar]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef] [PubMed]
- Jasinskaja-Lahti, I.; Horenczyk, G.; Kinunen, T. Time and Context in the Relationship between Acculturation Attitudes and Adaptation among Russian-Speaking Immigrants in Finland and Israel. J. Ethn. Migr. Stud. 2011, 37, 1423–1440. [Google Scholar] [CrossRef]
- Mirsky, J.; Baron-Draiman, Y.; Kedem, P. Social support and psychological distress among young immigrants from the former Soviet Union in Israel. Int. Soc. Work 2002, 45, 83–97. [Google Scholar] [CrossRef]
- Salovey, P.; Stroud, L.R.; Woolery, A.; Epel, E.S. Perceived emotional intelligence, stress reactivity, and symptom reports: Further explorations using the Trait Meta-Mood Scale. Psychol. Health 2002, 17, 611–627. [Google Scholar] [CrossRef]
- Lizeretti, N.P.; Extremera, N. Emotional Intelligence and Clinical Symptoms in Outpatients with Generalized Anxiety Disorder (GAD). Psychiatr. Q. 2011, 82, 253–260. [Google Scholar] [CrossRef]
- Martins, A.; Ramalho, N.; Morin, E. A comprehensive meta-analysis of the relationship between emotional intelligence and health. Personal. Individ. Differ. 2010, 49, 554–564. [Google Scholar] [CrossRef]
- Johnson, S.K.; Blanchard, A. Emotional Intelligence and Mental Health: Stress and Symptom Reporting Pathways. J. Ment. Health Couns. 2016, 38, 79–92. [Google Scholar] [CrossRef]
- Saklofske, D.H.; Austin, E.J.; Galloway, J.; Davidson, K. Individual difference correlates of health-related behaviours: Preliminary evidence for links between emotional intelligence and coping. Personal. Individ. Differ. 2007, 42, 491–502. [Google Scholar] [CrossRef]
- Martínez, A.E.; Piqueras, J.A.; Inglés, C. Relaciones entre inteligencia emocional y estrategias de afrontamiento ante el estrés (Relationship between emotional intelligence and stress coping strategies). Electron. J. Res. Educ. Psychol. 2011, 37, 20–21. [Google Scholar]
- Fernández-Abascal, E.G.; Martín-Díaz, M.D. Relations Between Dimensions of Emotional Intelligence, Specific Aspects of Empathy, and Non-verbal Sensitivity. Front. Psychol. 2019, 10, 1066. [Google Scholar] [CrossRef]
- El-Awad, U.; Fathi, A.; Petermann, F.; Reinelt, T. Promoting Mental Health in Unaccompanied Refugee Minors: Recommendations for Primary Support Programs. Brain Sci. 2017, 7, 146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofstede, G. Ecuador and Romania Culture Dimensions. Available online: https://www.hofstede-insights.com/ (accessed on 10 September 2019).
- Matsumoto, D.; Yoo, S.H.; Nakagawa, S. Members of the Multinational Study of Cultural Display Rules. Culture, emotion regulation, and adjustment. J. Personal. Soc. Psychol. 2008, 94, 925–937. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.J.; Richards, J.M.; John, O.P. Emotion Regulation in Everyday Life. In Emotion Regulation in Families: Pathways to Dysfunction and Health; Snyder, D.K., Simpson, J.A., Hughes, J.N., Eds.; American Psychological Association: Washington, DC, USA, 2006; pp. 13–35. [Google Scholar]
- Greenberg, R.S.; Daniels, S.R.; Flanders, W.D.; Eley, J.W.; Boring, J.R. Interpretation of epidemiologic literature. In Medical Epidemiology, 3rd ed.; Greenberg, R.S., Ed.; McGraw Hill: New York, NY, USA, 2001; pp. 175–188. [Google Scholar]
- Good, P.; Hardin, J. Common Errors in Statistics: And How to Avoid Them; John Wiley Sons: Hoboken, NJ, USA, 2003. [Google Scholar]
- Tracey, T.J.G. A Note on Socially Desirable Responding. J. Couns. Psychol. 2016, 63, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Peña-Acuña, B.; Pisonero, C.G. Ethnography and Emotions: Cultural Intelligence Applied to Motherhood Migration Process. Procedia-Soc. Behav. Sci. 2017, 237, 446–451. [Google Scholar]
- Hampton, B.M.; Peter, P.C.; Corus, C.; Brinberg, D. Integrating the unified theory and stages of change to create targeted health messages. J. Appl. Soc. Psychol. 2009, 39, 449–471. [Google Scholar] [CrossRef]
- Jamieson, J.P.; Mendes, W.B.; Nock, M.K. Improving Acute Stress Responses: The Power of Reappraisal. Curr. Dir. Psychol. Sci. 2013, 22, 51–56. [Google Scholar] [CrossRef] [Green Version]
- Larsen, R.J.; Prizmic, Z. Regulation of emotional well-being: Overcoming the hedonic treadmill. In The Science of Subjective Well-Being; Eid, M., Larsen, R.J., Eds.; Guilford Press: New York, NY, USA, 2008; pp. 258–289. [Google Scholar]

{kind=link}
| α | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Psy. Dist. T1 | 0.77 | 0.44 *** | 0.24 * | 0.12 | 0.24 * | −0.02 | −0.28* | −0.13 | −0.26 | 0.02 | 0.43 *** | 0.19 | 0.44 ** | 0.24 | −0.17 | −0.26 * |
| 2. Psy. Dist. T2 | 0.88 | 0.26 * | 0.01 | 0.32 * | 0.25 | −0.01 | −0.02 | 0.02 | −0.15 | 0.44 *** | 0.27 * | 0.29 * | 0.28 * | −0.04 | −0.41 ** | |
| 3. Perc. heal. T1 | 0.60 *** | −0.07 | 0.27 * | −0.26 | 0.20 | −0.04 | 0.22 | 0.35 ** | 0.01 | 0.32 * | 0.03 | 0.16 | −0.03 | |||
| 4. Perc. heal. T2 | 0.03 | 0.07 | −0.08 | 0.04 | −0.01 | 0.09 | 0.02 | 0.05 | 0.03 | 0.06 | 0.06 | 0.04 | ||||
| 5. Attention T1 | 0.87 | 0.25 | 0.26 * | −0.13 | 0.25 * | −0.10 | 0.21 | 0.27 * | 0.27 * | 0.33 ** | −0.08 | −0.08 | ||||
| 6. Attention T2 | 0.84 | −0.19 | 0.50 *** | 0.06 | 0.54 *** | 0.20 | 0.15 | 0.13 | 0.16 | −0.07 | −0.02 | |||||
| 7. Clarity T1 | 0.79 | 0.07 | 0.49 *** | −0.18 | −0.09 | 0.06 | −0.07 | 0.01 | −0.05 | 0.08 | ||||||
| 8. Clarity T2 | 0.87 | 0.08 | 0.59 *** | 0.06 | 0.08 | 0.12 | 0.06 | −0.04 | 0.06 | |||||||
| 9. Mood rep. T1 | 0.93 | 0.17 | 0.03 | 0.12 | 0.07 | 0.16 | 0.15 | 0.24 | ||||||||
| 10. Mood rep. T2 | 0.90 | 0.15 | 0.11 | 0.18 | 0.23 | −0.03 | 0.23 | |||||||||
| 11. Beh. adj. T1 | 0.92 | 0.46 *** | 0.86 *** | 0.44 ** | 0.21 | −0.29 * | ||||||||||
| 12. Beh. adj.T2 | 0.87 | 0.35 ** | 0.85 *** | 0.13 | −0.08 | |||||||||||
| 13. Cog. adj. T1 | 0.94 | 0.45 ** | 0.12 | −0.16 | ||||||||||||
| 14. Cog. adj.T2 | 0.87 | −0.45 | −0.04 | |||||||||||||
| 15. Gen. sit. T1 | 0.16 | |||||||||||||||
| 16. Gen. sit. T2 |
| Variables | Sex | Origin | Wave | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Romanian | Ecuadorian | Time 1 | SD | Time 2 | SD | |||||
| M | SD | M | SD | M | SD | M | SD | |||||
| Psychological Distress T1 | 9.81 | 5.21 | 11.09 | 4.87 | 9.90 | 4.73 | 11.07 | 5.11 | 10.68 | 4.99 | ||
| Psychological Distress T2 | 10.15 | 6.64 | 12.40 | 6.58 | 12.95 | 7.29 | 11.05 | 6.26 | 11.68 | 6.63 | ||
| Perceived health T1 | 2.16 | 0.69 | 2.40 | 0.79 | 2.52 | 0.60 | 2.22 | 0.82 | 2.32 | 0.76 | ||
| Perceived health T2 | 2.25 | 0.85 | 2.37 | 0.73 | 2.52 | 0.60 | 2.24 | 0.82 | 2.33 | 0.76 | ||
| Attention T1 | 3.28 | 0.86 | 3.31 | 0.94 | 2.88 | 0.97 | 3.52 | 0.80 | 3.31 | 0.91 | ||
| Attention T2 | 3.38 | 0.67 | 3.21 | 1.02 | 3.31 | 0.92 | 3.24 | 0.93 | 3.27 | 0.92 | ||
| Clarity T1 | 3.40 | 0.69 | 3.47 | 0.87 | 3.27 | 0.88 | 3.54 | 0.77 | 3.45 | 0.81 | ||
| Clarity T2 | 3.82 | 0.82 | 3.40 | 0.99 | 3.74 | 0.89 | 3.43 | 0.99 | 3.54 | 0.95 | ||
| Mood repair T1 | 3.96 | 0.76 | 4.04 | 0.63 | 3.80 | 0.64 | 4.12 | 0.66 | 4.02 | 0.66 | ||
| Mood repair T2 | 4.13 | 0.64 | 3.80 | 0.82 | 3.92 | 0.68 | 3.90 | 0.83 | 3.91 | 0.78 | ||
| Behavioral adjustment T1 | 2.01 | 0.64 | 1.98 | 0.79 | 1.60 | 0.67 | 2.19 | 0.70 | 1.99 | 0.74 | ||
| Behavioral adjustment T2 | 2.10 | 0.90 | 1.80 | 0.66 | 1.56 | 0.45 | 2.06 | 0.81 | 1.89 | 0.74 | ||
| Cognitive adjustment T1 | 2.18 | 0.87 | 2.18 | 0.96 | 1.73 | 0.87 | 2.41 | 0.88 | 1.90 | 0.75 | ||
| Cognitive adjustment T2 | 2.19 | 0.90 | 1.93 | 0.78 | 1.67 | 0.67 | 2.19 | 0.85 | 2.01 | 0.82 | ||
| General situation T1 | 2.55 | 0.61 | 2.49 | 0.75 | 2.57 | 0.68 | 2.48 | 0.72 | 2.51 | 0.70 | ||
| General situation T2 | 2.70 | 0.47 | 2.53 | 0.74 | 2.62 | 0.59 | 2.57 | 0.70 | 2.59 | 0.60 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Castro, J.L.; Ubillos Landa, S.; Puente Martínez, A.; Vera Perea, M. The Role of Emotional Intelligence and Sociocultural Adjustment on Migrants’ Self-reported Mental Well-Being in Spain: A 14 Month Follow-Up Study. Int. J. Environ. Res. Public Health 2020, 17, 1206. https://doi.org/10.3390/ijerph17041206
González-Castro JL, Ubillos Landa S, Puente Martínez A, Vera Perea M. The Role of Emotional Intelligence and Sociocultural Adjustment on Migrants’ Self-reported Mental Well-Being in Spain: A 14 Month Follow-Up Study. International Journal of Environmental Research and Public Health. 2020; 17(4):1206. https://doi.org/10.3390/ijerph17041206
Chicago/Turabian StyleGonzález-Castro, José Luis, Silvia Ubillos Landa, Alicia Puente Martínez, and Maria Vera Perea. 2020. "The Role of Emotional Intelligence and Sociocultural Adjustment on Migrants’ Self-reported Mental Well-Being in Spain: A 14 Month Follow-Up Study" International Journal of Environmental Research and Public Health 17, no. 4: 1206. https://doi.org/10.3390/ijerph17041206
APA StyleGonzález-Castro, J. L., Ubillos Landa, S., Puente Martínez, A., & Vera Perea, M. (2020). The Role of Emotional Intelligence and Sociocultural Adjustment on Migrants’ Self-reported Mental Well-Being in Spain: A 14 Month Follow-Up Study. International Journal of Environmental Research and Public Health, 17(4), 1206. https://doi.org/10.3390/ijerph17041206