Acute Kidney Injury Biomarker Responses to Short-Term Heat Acclimation

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Methods
2.2. Exercise Protocol
2.3. Data Management and Statistical Analysis
3. Results
3.1. Heat Acclimation
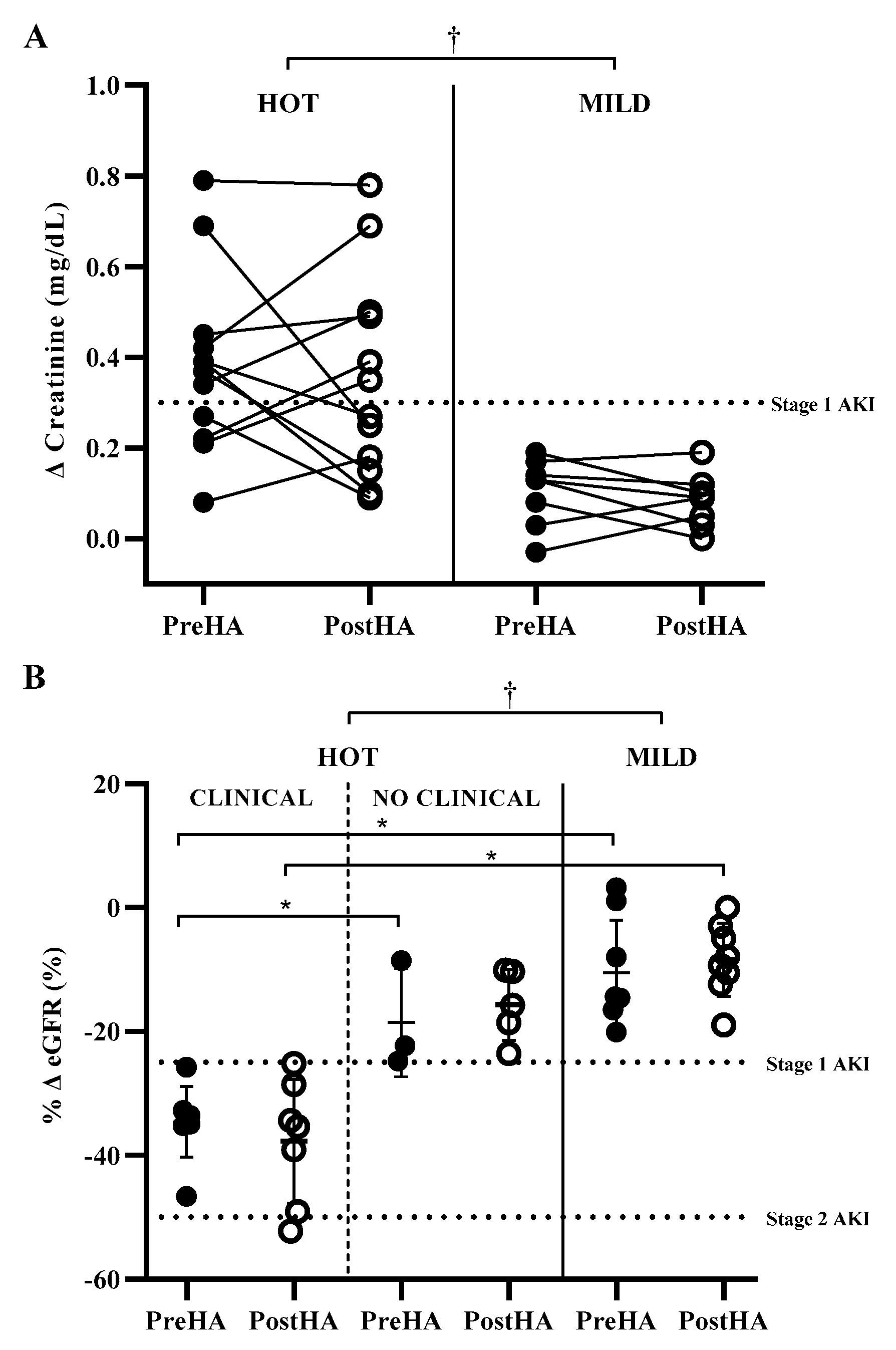
3.2. Impact of HA on Clinical Biomarkers of AKI in HOT and MILD
3.3. Impact of Environment on CLINICAL Incidence
3.4. CLINICAL, NO CLINICAL, and Mild Environment PreHA
3.5. CLINICAL, NO CLINICAL, and Mild Environment PostHA
3.6. Relationships among Clinical Biomarkers of AKI and Cardiovascular Strain, Thermoregulatory Strain, and Hydration
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hostler, D.; Bednez, J.C.; Kerin, S.; Reis, S.E.; Kong, P.W.; Morley, J.; Gallagher, M., Jr.; Suyama, J. Comparison of rehydration regimens for rehabilitation of firefighters performing heavy exercise in thermal protective clothing: A report from the fireground rehab evaluation (fire) trial. Prehosp. Emerg. Care 2010, 14, 194–201. [Google Scholar] [CrossRef] [PubMed]
- DeMartini, J.K.; Martschinske, J.L.; Casa, D.J.; Lopez, R.M.; Ganio, M.S.; Walz, S.M.; Coris, E.E. Physical demands of national collegiate athletic association division I football players during preseason training in the heat. J. Strength Cond. Res. 2011, 25, 2935–2943. [Google Scholar] [CrossRef] [PubMed]
- Yeargin, S.W.; Casa, D.J.; Armstrong, L.E.; Watson, G.; Judelson, D.A.; Psathas, E.; Sparrow, S.L. Heat acclimatization and hydration status of american football players during initial summer workouts. J. Strength Cond. Res. 2006, 20, 463–470. [Google Scholar] [PubMed]
- Horn, G.P.; Blevins, S.; Fernhall, B.; Smith, D.L. Core temperature and heart rate response to repeated bouts of firefighting activities. Ergonomics 2013, 56, 1465–1473. [Google Scholar] [CrossRef] [PubMed]
- Meade, R.D.; D’Souza, A.W.; Krishen, L.; Kenny, G.P. The physiological strain incurred during electrical utilities work over consecutive work shifts in hot environments: A case report. J. Occup. Environ. Hyg. 2017, 14, 986–994. [Google Scholar] [CrossRef] [PubMed]
- Radigan, L.R.; Robinson, S. Effects of environmental heat stress and exercise on renal blood flow and filtration rate. J. Appl. Physiol. 1949, 2, 185–191. [Google Scholar] [CrossRef]
- Smith, J.; Robinson, S.; Pearcy, M. Renal responses to exercise, heat and dehydration. J. Appl. Physiol. 1952, 4, 659–665. [Google Scholar] [CrossRef]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P. Acute renal failure-definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004, 8, R204–R212. [Google Scholar] [CrossRef] [Green Version]
- Khwaja, A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef]
- Schrier, R.W.; Hano, J.; Keller, H.I.; Finkel, R.M.; Gilliland, P.F.; Cirksena, W.J.; Teschan, P.E. Renal, metabolic, and circulatory responses to heat and exercise: Studies in military recruits during summer training, with implications for acute renal failure. Ann. Int. Med. 1970, 73, 213–223. [Google Scholar] [CrossRef]
- Schlader, Z.J.; Chapman, C.L.; Sarker, S.; Russo, L.; Rideout, T.C.; Parker, M.D.; Johnson, B.D.; Hostler, D. Firefighter work duration influences the extent of acute kidney injury. Med. Sci. Sport Exerc. 2017, 49, 1745–1753. [Google Scholar] [CrossRef] [PubMed]
- Moyce, S.; Joseph, J.; Tancredi, D.; Mitchell, D.; Schenker, M. Cumulative incidence of acute kidney injury in California’s agricultural workers. J. Occup. Environ. Med. 2016, 58, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Wegman, D.H.; Apelqvist, J.; Bottai, M.; Ekström, U.; García-Trabanino, R.; Glaser, J.; Hogstedt, C.; Jakobsson, K.; Jarquín, E.; Lucas, R.A.; et al. Intervention to diminish dehydration and kidney damage among sugarcane workers. Scand. J. Work Environ. Heat 2018, 44, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Divine, J.G.; Clark, J.F.; Colosimo, A.J.; Donaworth, M.; Hasselfeld, K.; Himmler, A.; Rauch, J.; Mangine, R. American football players in preseason training at risk of acute kidney injury without signs of rhabdomyolysis. Clin. J. Sport Med. 2018. [Google Scholar] [CrossRef]
- Colombini, A.; Machado, M.; Lombardi, G.; Lanteri, P.; Banfi, G. Modifications of biochemical parameters related to protein metabolism and renal function in male soccer players after a match. J. Sports Med. Phys. Fit. 2014, 54, 658–664. [Google Scholar]
- Hoffman, M.D.; Weiss, R.H. Does acute kidney injury from an ultramarathon increase the risk for greater subsequent injury? Clin. J. Sport Med. 2016, 26, 417–422. [Google Scholar] [CrossRef] [Green Version]
- Hodgson, L.; Walter, E.; Venn, R.; Galloway, R.; Pitsiladis, Y.; Sardat, F.; Forni, L. Acute kidney injury associated with endurance events—Is it a cause for concern? A systematic review. BMJ Open Sport Exerc. Med 2017, 3, e000093. [Google Scholar] [CrossRef] [Green Version]
- McDermott, B.P.; Smith, C.R.; Butts, C.L.; Caldwell, A.R.; Lee, E.C.; Vingren, J.L.; Munoz, C.X.; Kunces, L.J.; Williamson, K.; Ganio, M.S.; et al. Renal stress and kidney injury biomarkers in response to endurance cycling in the heat with and without ibuprofen. J. Sci. Med. Sport 2018, 21, 1180–1184. [Google Scholar] [CrossRef]
- Chapman, C.L.; Johnson, B.D.; Sackett, J.R.; Parker, M.D.; Schlader, Z.J. Soft drink consumption during and following exercise in the heat elevates biomarkers of acute kidney injury. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2019, 316, R189–R198. [Google Scholar] [CrossRef]
- Heung, M.; Steffick, D.E.; Zivin, K.; Gillespie, B.W.; Banerjee, T.; Hsu, C.Y.; Powe, N.R.; Pavkov, M.E.; Williams, D.E.; Saran, R.; et al. Acute kidney injury recovery pattern and subsequent risk of CKD: An analysis of veterans health administration data. Am. J. Kidney Dis. 2016, 67, 742–752. [Google Scholar] [CrossRef]
- Armstrong, L.E.; Maresh, C.M. The induction and decay of heat acclimatisation in trained athletes. Sport Med. 1991, 12, 302–312. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, S.; Esterman, A.; Eston, R.; Bowering, K.J.; Norton, K. Short-term heat acclimation training improves physical performance: A systematic review, and exploration of physiological adaptations and application for team sports. Sport Med. 2014, 44, 971–988. [Google Scholar] [CrossRef]
- Chen, T.-I.; Tsai, P.-H.; Lin, J.-H.; Lee, N.-Y.; Liang, M.T. Effect of short-term heat acclimation on endurance time and skin blood flow in trained athletes. Open Access. J. Sport Med. 2013, 4, 161–170. [Google Scholar]
- Lorenzo, S.; Halliwill, J.R.; Sawka, M.N.; Minson, C.T. Heat acclimation improves exercise performance. J. Appl. Physiol. 2010, 109, 1140–1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pryor, J.L.; Pryor, R.R.; Vandermark, L.W.; Adams, E.L.; VanScoy, R.M.; Casa, D.J.; Armstrong, L.E.; Lee, E.C.; DiStefano, L.J.; Anderson, J.M.; et al. Intermittent exercise-heat exposures and intense physical activity sustain heat acclimation adaptations. J. Sci. Med. Sport 2019, 22, 117–122. [Google Scholar] [CrossRef]
- Finberg, J.; Berlyne, G. Modification of renin and aldosterone response to heat by acclimatization in man. J. Appl. Physiol. 1977, 42, 554–558. [Google Scholar] [CrossRef]
- Montain, S.; Sawka, M.; Latzka, W.; Valeri, C. Thermal and cardiovascular strain from hypohydration: Influence of exercise intensity. Int. J. Sport Med. 1998, 19, 87–91. [Google Scholar] [CrossRef]
- Montain, S.J.; Coyle, E.F. Influence of graded dehydration on hyperthermia and cardiovascular drift during exercise. J. Appl. Physiol. 1992, 73, 1340–1350. [Google Scholar] [CrossRef]
- Patterson, M.J.; Stocks, J.M.; Taylor, N.A. Sustained and generalized extracellular fluid expansion following heat acclimation. J. Physiol. 2004, 559, 327–334. [Google Scholar] [CrossRef]
- Roberts, M.F.; Wenger, C.B.; Stolwijk, J.; Nadel, E.R. Skin blood flow and sweating changes following exercise training and heat acclimation. J. Appl. Physiol. 1977, 43, 133–137. [Google Scholar] [CrossRef]
- Omassoli, J.; Hill, N.E.; Woods, D.R.; Delves, S.K.; Fallowfield, J.L.; Brett, S.J.; Wilson, D.; Corbett, R.W.; Allsopp, A.J.; Stacey, M.J. Variation in renal responses to exercise in the heat with progressive acclimatisation. J. Sci. Med. Sport 2019, 22, 1004–1009. [Google Scholar] [CrossRef] [PubMed]
- Jackson, A.S.; Pollock, M.L. Prediction accuracy of body density, lean body weight, and total body volume equations. Med. Sci. Sport 1976, 9, 197–201. [Google Scholar]
- Kaminsky, L.A.; Arena, R.; Myers, J. Reference standards for cardiorespiratory fitness measured with cardiopulmonary exercise testing: Data from the fitness registry and the importance of exercise national database. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2015; pp. 1515–1523. [Google Scholar]
- Pryor, R.R.; Pryor, J.L.; Vandermark, L.W.; Adams, E.L.; Brodeur, R.M.; Armstrong, L.E.; Lee, E.C.; Maresh, C.M.; Andersen, J.M.; Casa, D.J. Exacerbated heat strain during consecutive days of repeated exercise sessions in heat. J. Sci. Med. Sport 2019, 22, 1084–1089. [Google Scholar] [CrossRef] [PubMed]
- Utter, A.C.; Robertson, R.J.; Green, J.M.; Suminski, R.R.; McAnulty, S.R.; Nieman, D.C. Validation of the Adult OMNI Scale of perceived exertion for walking/running exercise. Med. Sci. Sport Exerc. 2004, 36, 1776–1780. [Google Scholar] [CrossRef] [PubMed]
- Stearns, R.L.; Belval, L.N.; Casa, D.J.; Klau, J.F.; Emmanuel, H.; Armstrong, L.E.; Maresh, C.M. Two environmental symptoms questionnaires during 10 days of exercise-heat acclimation. Aviat. Space Environ. Med. 2013, 84, 797–802. [Google Scholar] [CrossRef]
- Dill, D.B.; Costill, D.L. Calculation of percentage changes in volumes of blood, plasma, and red cells in dehydration. J. Appl. Physiol. 1974, 37, 247–248. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T. A new equation to estimate glomerular filtration rate. Ann. Int. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Pruessner, J.C.; Kirschbaum, C.; Meinlschmid, G.; Hellhammer, D.H. Two formulas for computation of the area under the curve represent measures of total hormone concentration versus time-dependent change. Psychoneuroendocrino 2003, 28, 916–931. [Google Scholar] [CrossRef]
- Junglee, N.A.; Di Felice, U.; Dolci, A.; Fortes, M.B.; Jibani, M.M.; Lemmey, A.B.; Walsh, N.P.; Macdonald, J.H. Exercising in a hot environment with muscle damage: Effects on acute kidney injury biomarkers and kidney function. Am. J. Physiol. Ren. 2013, 305, F813–F820. [Google Scholar] [CrossRef]
- Schlader, Z.J.; Colburn, D.; Hostler, D. Heat strain is exacerbated on the second of consecutive days of fire suppression. Med. Sci. Sport Exerc. 2017, 49, 999–1005. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, L.; Costill, D.; Fink, W. Changes in body water and electrolytes during heat acclimation: Effects of dietary sodium. Aviat. Space Environ. Med. 1987, 58, 143–148. [Google Scholar] [PubMed]
- Shvartz, E.; Bhattacharya, A.; Sperinde, S.; Brock, P.; Sciaraffa, D.; Van Beaumont, W. Sweating responses during heat acclimation and moderate conditioning. J. Appl. Physiol. 1979, 46, 675–680. [Google Scholar] [CrossRef]
- Hodge, D.; Jones, D.; Martinez, R.; Buono, M.J. Time course of the attenuation of sympathetic nervous activity during active heat acclimation. Auton. Neurosci. 2013, 177, 101–103. [Google Scholar] [CrossRef]
- Jones, S.; Musacchia, X.; Tempel, G. Mechanisms of temperature regulation in heat-acclimated hamsters. Am. J. Physiol 1976, 231, 707–712. [Google Scholar] [CrossRef] [PubMed]
- Chayoth, R.; Kleinman, D.; Kaplanski, J.; Sod Moriah, U. Renal clearance of urea, inulin, and p-aminohippurate in heat-acclimated rats. J. Appl. Physiol. 1984, 57, 731–732. [Google Scholar] [CrossRef] [PubMed]
- Rowell, L.B.; Marx, H.J.; Bruce, R.A.; Conn, R.D.; Kusumi, F. Reductions in cardiac output, central blood volume, and stroke volume with thermal stress in normal men during exercise. J. Clin. Investig. 1966, 45, 1801–1816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawka, M.N.; Burke, L.M.; Eichner, E.R.; Maughan, R.J.; Montain, S.J.; Stachenfeld, N.S. American College of Sports Medicine position stand. Exercise and fluid replacement. Med. Sci. Sport Exerc. 2007, 39, 377–390. [Google Scholar]
- Borg, G. Perceived exertion as an indicator of somatic stress. Scand. J. Rehab. Med. 1970, 2, 92–98. [Google Scholar]
- García-Trabanino, R.; Jarquín, E.; Wesseling, C.; Johnson, R.J.; González-Quiroz, M.; Weiss, I.; Glaser, J.; Vindell, J.J.; Stockfelt, L.; Roncal, C.; et al. Heat stress, dehydration, and kidney function in sugarcane cutters in El Salvador—A cross-shift study of workers at risk of Mesoamerican nephropathy. Environ. Res. 2015, 142, 746–755. [Google Scholar] [CrossRef] [Green Version]
- Jayasekara, K.; Kulasooriya, P.; Wijayasiri, K.; Rajapakse, E.; Dulshika, D.; Bandara, P.; Fried, L.; De Silva, A.; Albert, S. Relevance of heat stress and dehydration to chronic kidney disease (CKDu) in Sri Lanka. Prev. Med. Rep. 2019, 15, 100928. [Google Scholar] [CrossRef]
- Nickolas, T.L.; O’Rourke, M.M.J.; Yang, J.; Sise, M.M.E.; Canetta, P.A.; Barasch, M.N.; Buchen, M.C.; Khan, F.; Mori, K.; Giglio, J.; et al. Sensitivity and specificity of a single emergency department measurement of urinary neutrophil gelatinase-associated lipocalin for diagnosing acute kidney injury. Ann. Int. Med. 2008, 148, 810–819. [Google Scholar] [CrossRef] [PubMed]
- Haase, M.; Devarajan, P.; Haase-Fielitz, A.; Bellomo, R.; Cruz, D.N.; Wagener, G.; Krawczeski, C.D.; Koyner, J.L.; Murray, P.; Zappitelli, M.; et al. The outcome of neutrophil gelatinase-associated lipocalin-positive subclinical acute kidney injury: A multicenter pooled analysis of prospective studies. J. Am. Coll. Cardio 2011, 57, 1752–1761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, E.; Schrezenmeier, E.V.; Elger, A.; Seelow, E.R.; Krannich, A.; Luft, F.C.; Schmidt-Ott, K.M. Urinary NGAL-positive acute kidney injury and poor long-term outcomes in hospitalized patients. Kidney Int. Rep. 2016, 1, 114–124. [Google Scholar] [CrossRef] [Green Version]
- Bulluck, H.; Maiti, R.; Chakraborty, B.; Candilio, L.; Clayton, T.; Evans, R.; Jenkins, D.P.; Kolvekar, S.; Kunst, G.; Laing, C.; et al. Neutrophil gelatinase-associated lipocalin prior to cardiac surgery predicts acute kidney injury and mortality. Heart 2018, 104, 313–317. [Google Scholar] [CrossRef] [PubMed]
- Bennett, M.; Dent, C.L.; Ma, Q.; Dastrala, S.; Grenier, F.; Workman, R.; Syed, H.; Ali, S.; Barasch, J.; Devarajan, P. Urine NGAL predicts severity of acute kidney injury after cardiac surgery: A prospective study. Clin. J. Am. Soc. Nephrol. 2008, 3, 665–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Au, V.; Feit, J.; Barasch, J.; Sladen, R.N.; Wagener, G. Urinary neutrophil gelatinase-associated lipocalin (NGAL) distinguishes sustained from transient acute kidney injury after general surgery. Kidney Int. Rep. 2016, 1, 3–9. [Google Scholar] [CrossRef] [Green Version]
- Tidbury, N.; Browning, N.; Shaw, M.; Morgan, M.; Kemp, I.; Matata, B. Neutrophil gelatinase-associated lipocalin as a marker of postoperative acute kidney injury following cardiac surgery in patients with pre-operative kidney impairment. Card Hematol. Disord. Dr. 2019, 19, 239–248. [Google Scholar]
- Gocze, I.; Koch, M.; Renner, P.; Zeman, F.; Graf, B.M.; Dahlke, M.H.; Nerlich, M.; Schlitt, H.J.; Kellum, J.A.; Bein, T. Urinary biomarkers TIMP-2 and IGFBP7 early predict acute kidney injury after major surgery. PLoS ONE 2015, 10, e0120863. [Google Scholar] [CrossRef] [Green Version]
- Wetz, A.J.; Richardt, E.M.; Wand, S.; Kunze, N.; Schotola, H.; Quintel, M.; Bräuer, A.; Moerer, O. Quantification of urinary TIMP-2 and IGFBP-7: An adequate diagnostic test to predict acute kidney injury after cardiac surgery? Crit. Care 2015, 19, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Pilarczyk, K.; Edayadiyil-Dudasova, M.; Wendt, D.; Demircioglu, E.; Benedik, J.; Dohle, D.S.; Jakob, H.; Dusse, F. Urinary [TIMP-2]*[IGFBP7] for early prediction of acute kidney injury after coronary artery bypass surgery. Ann. Intensive Care 2015, 5, 50. [Google Scholar] [CrossRef] [Green Version]
- Schlader, Z.J.; Hostler, D.; Parker, M.D.; Pryor, R.R.; Lohr, J.W.; Johnson, B.D.; Chapman, C.L. The potential for renal injury elicited by physical work in the heat. Nutrients 2019, 11, 2087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Périard, J.; Racinais, S.; Sawka, M.N. Adaptations and mechanisms of human heat acclimation: Applications for competitive athletes and sports. Scand. J. Med. Sci. Sport 2015, 25, 20–38. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Measurement | PreHA | PostHA | ||||||
|---|---|---|---|---|---|---|---|---|
| Hot | Mild (n = 8) | ES | Hot | Mild (n = 8) | ES | |||
| CLINICAL (n = 9) | NO CLINICAL (n = 3) | CLINICAL (n = 7) | NO CLINICAL (n = 5) | |||||
| Urine Specific Gravity | 1.018 ± 0.009 | 1.012 ± 0.008 | 1.014 ± 0.007 | 0.57 | 1.018 ± 0.008 | 1.022 ± 0.010 | 1.018 ± 0.009 | 0.01 |
| Sweat Rate (L·h−1) | 1.70 ± 0.37 * | 1.44 ± 0.12 * | 0.76 ± 0.08 | 0.65 | 1.86 ± 0.57 | 2.04 ± 0.43 * | 1.05 ± 0.80 | 0.29 |
| Total Sweat Loss (L) | 5.81 ± 1.23 * | 5.29 ± 0.97 * | 2.65 ± 0.52 | 0.37 | 6.31 ± 1.22 * | 5.51 ± 0.85 * | 2.87 ± 0.79 | 0.62 |
| Fluid Consumption (L) | 3.61 ± 1.33 * | 4.79 ± 2.13 * | 1.79 ± 0.95 | 0.65 | 4.76 ± 1.82 * | 3.39 ± 1.00 | 1.68 ± 0.83 | 0.74 |
| Percent Fluid Replaced (%) | 61.9 ± 18.9 | 88.6 ± 25.6 | 70.6 ± 40.5 | 1.10 | 73.2 ± 16.4 | 61.9 ± 16.3 | 60.5 ± 33.3 | 0.58 |
| Percent Δ Plasma Volume (%) | −9.0 ± 3.9 * | −3.7 ± 5.6 | −0.6 ± 5.8 | 1.04 | −7.1 ± 5.4 | −3.5 ± 3.3 | −1.3 ± 4.5 | 0.65 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pryor, R.R.; Pryor, J.L.; Vandermark, L.W.; Adams, E.L.; Brodeur, R.M.; Schlader, Z.J.; Armstrong, L.E.; Lee, E.C.; Maresh, C.M.; Casa, D.J. Acute Kidney Injury Biomarker Responses to Short-Term Heat Acclimation. Int. J. Environ. Res. Public Health 2020, 17, 1325. https://doi.org/10.3390/ijerph17041325
Pryor RR, Pryor JL, Vandermark LW, Adams EL, Brodeur RM, Schlader ZJ, Armstrong LE, Lee EC, Maresh CM, Casa DJ. Acute Kidney Injury Biomarker Responses to Short-Term Heat Acclimation. International Journal of Environmental Research and Public Health. 2020; 17(4):1325. https://doi.org/10.3390/ijerph17041325
Chicago/Turabian StylePryor, Riana R., J. Luke Pryor, Lesley W. Vandermark, Elizabeth L. Adams, Rachel M. Brodeur, Zachary J. Schlader, Lawrence E. Armstrong, Elaine C. Lee, Carl M. Maresh, and Douglas J. Casa. 2020. "Acute Kidney Injury Biomarker Responses to Short-Term Heat Acclimation" International Journal of Environmental Research and Public Health 17, no. 4: 1325. https://doi.org/10.3390/ijerph17041325