Exploring the Effect of Market Conditions on Price Premiums in the Online Health Community


Abstract
:1. Introduction
2. Research Model and Hypotheses
2.1. Theory of Supply and Demand
2.2. Research Hypotheses
3. Materials and Methods
3.1. Research Context and Data Collection
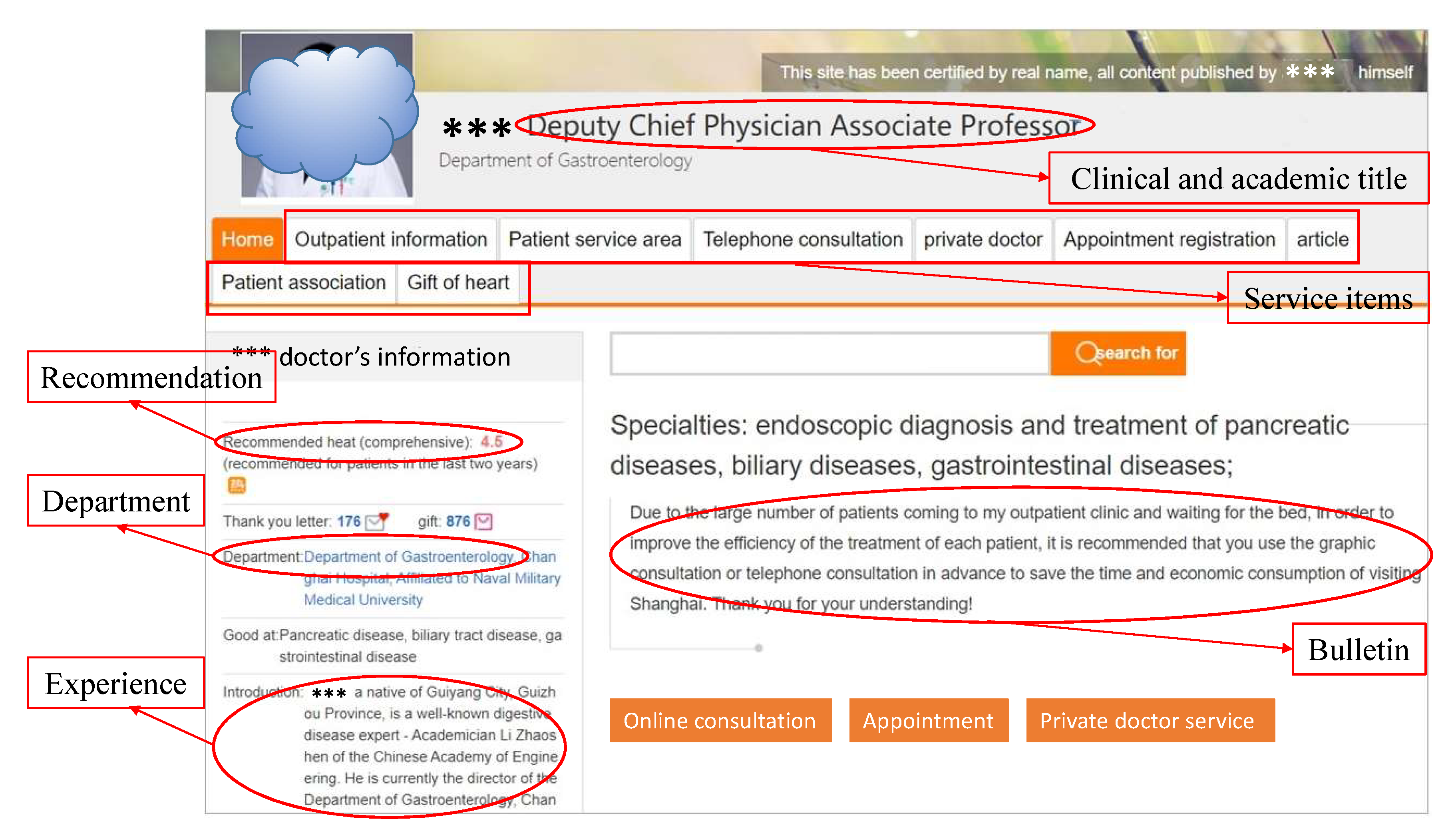
3.2. Variable Measurement
3.3. Estimation Model
- Offline concentration ratio (OfflineCR): In physical hospitals, each clinical department has many offline doctors. Some doctors provide online medical consultation services (OMCSs) in online health communities (OHCs), others do not. Online doctor resources are obtained from offline doctor resources. So, OfflineCR measures the concentration of offline doctor resources, whereas CR measures online doctor resources.
- The average participation ratio (PRmean): As shown in Equation (5), given province p and clinical department j, this is the sum of the participation ratio () divided by the number of hospitals that provide the OMCS associated with clinical department j (). is a set of hospitals that provide the OMCS associated with clinical department j in province p.
4. Results
4.1. Descriptive Statistics and Correlations
4.2. Empirical Results
4.3. Robustness Check
5. Discussion and Implications
5.1. Results Analysis
5.2. Implications
5.3. Limitations and Future Research
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wu, H.; Lu, N. Online written consultation, telephone consultation and offline appointment: An examination of the channel effect in online health communities. Int. J. Med Informatics 2017, 107, 107–119. [Google Scholar] [CrossRef]
- Lu, X.; Zhang, R.; Zhu, X. An empirical study on patients’ acceptance of physician-patient interaction in online health communities. Int. J. Environ. Res. Public Health 2019, 16, 5084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Rai, A.; Guo, X. Physicians’ online popularity and price premiums for online health consultations: A combined signaling theory and online feedback mechanisms explanation. In Proceedings of the Thirty Sixth International Conferences on Information Systems, Fort Worth, TX, USA, 13–16 December 2015; pp. 1–11. [Google Scholar]
- Chen, D.; Zhang, R.; Liu, K.; Hou, L. Knowledge discovery from posts in online health communities using unified medical language system. Int. J. Environ. Res. Public Health 2018, 15, 1291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nambisan, P. Information seeking and social support in online health communities: Impact on patients’ perceived empathy. J. Am. Med. Inform. Assoc. 2011, 18, 298–304. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Pan, M.; Li, J. Does sharing your emotion make you feel better? an empirical investigation on the association between sharing emotions on a virtual mood wall and the relief of patients’ negative emotions. Telemed. E-Health 2019, 25, 987–995. [Google Scholar] [CrossRef] [PubMed]
- Ba, S.; Wang, L. Digital health communities: The effect of their motivation mechanisms. Decis. Support Syst. 2013, 55, 941–947. [Google Scholar] [CrossRef]
- Kucukyazici, B.; Verter, V.; Mayo, N.E. An analytical eramework for designing community-based care for chronic diseases. Prod. Oper. Manag. 2011, 20, 474–488. [Google Scholar] [CrossRef]
- Lu, S.F.; Rui, H. Can we trust online physician ratings? Evidence from Cardiac Surgeons in Florida. Manag. Sci. 2018, 64, 2557–2573. [Google Scholar] [CrossRef]
- Puneet, M.; Packard, G.M.; Pattabhiramaiah, A. Social dollars: The economic impact of customer participation in a firm-sponsored online community. Mark. Sci. 2015, 34, 367–387. [Google Scholar] [CrossRef]
- Guo, S.; Guo, X.; Fang, Y.; Doug, V. How doctors gain social and economic returns in online health-care communities: A professional capital perspective. J. Manag. Inf. Syst. 2017, 34, 487–519. [Google Scholar] [CrossRef]
- Wu, H.; Lu, N. Service provision, pricing, and patient satisfaction in online health communities. Int. J. Med Informatics 2018, 110, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Guo, S.; Douglas, V.; Li, Y. Online healthcare community interaction dynamics. J. Manag. Sci. Eng. 2016, 1, 58–74. [Google Scholar] [CrossRef]
- Maxwell, S. Rule-based price fairness and its effect on willingness to purchase. J. Econ. Psychol. 2002, 23, 191–212. [Google Scholar] [CrossRef]
- Li, Y.; Song, Y.; Zhao, W.; Guo, X.; Ju, X.; Doug, V. Exploring the role of online health community information in patients’ decisions to switch from online to offline medical services. Int. J. Med Inform. 2019, 130, 103951. [Google Scholar] [CrossRef]
- Li, Y. Impact Factors of Physicians’ Service Price in Online Healthcare Community. Master’s Thesis, Harbin Institute of Technology, Harbin, China, 2016. [Google Scholar]
- Constantinides, E.; Fountain, S.J. Web 2.0: Conceptual foundations and marketing issues. J. Direct Data Digit. Mark. Pract. 2008, 9, 231–244. [Google Scholar] [CrossRef]
- Li, J.; Li, F.; Liu, X.; Ma, L. Differentiation strategy in online physician competition: Does specialization matter? Telemed. e-Health 2019. [Google Scholar] [CrossRef] [PubMed]
- Klein, B.; Leffler, K.B. The role of market forces in assuring contractual performance. J. Political Econ. 1981, 89, 615–641. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Tang, J.; Jiang, L.; Chen, J.; Liu, X. Price premiums in the online health consultation market. J. Manag. Sci. 2018, 31, 15–32. [Google Scholar] [CrossRef]
- Buckman, L. Is doctors’ self interest undermining the national health service? BMJ 2007, 334, 235. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.; Liu, L.; Wang, Y.; Gao, F.; Wang, L. Factors associated with burnout among Chinese hospital doctors: A cross-sectional study. BMC Public Health 2013, 13, 786. [Google Scholar] [CrossRef] [Green Version]
- Liu, F.; Li, Y.; Ju, X. Exploring patients’ consultation behaviors in the online health community: The role of disease risk. Telemed. E-Health 2019, 25. [Google Scholar] [CrossRef] [PubMed]
- Cao, X.; Liu, Y.; Zhu, Z.; Hu, J.; Chen, X. Online selection of a physician by patients: Empirical study from elaboration likelihood perspective. Comput. Hum. Behav. 2017, 73, 403–412. [Google Scholar] [CrossRef]
- Chang, M. Social Representations of the Stigmatized Diseases: A Multidimensional Scaling Analysis; Kaohsiung Medical University: Kaohsiung, Taiwan, 2004; pp. 1–15. [Google Scholar]
- Chang, M.; Chen, Y.; Shen, C.; Yu, L. Dimensions of disease stigma in Taiwan: A multidimensional scaling analysis. J. Psychol. Chin. Soc. 2008, 10, 65–84. [Google Scholar]
- Zhou, J.; Zuo, M.; Ye, C. Understanding the factors influencing health professionals’ online voluntary behaviors: Evidence from YiXinLi, a Chinese online health community for mental health. Int. J. Med. Inform. 2019, 130, 103939. [Google Scholar] [CrossRef]
- Mankiw, N. (Ed.) Principles of Microeconomics, 8th ed.; South-Western Cengage Learning: Boston, MA, USA, 2017. [Google Scholar]
- Porter, M.E. (Ed.) Competitive Strategy: Techniques for Analyzing Industries and Competitors; China CITIC Press: Beijing, China, 2016. [Google Scholar]
- Han, Y. Competitive strategy within the marketing. Chin. J. Manag. Sci. 2000, 11, 545–552. [Google Scholar] [CrossRef]
- Kuang, J.; Kuang, L.; Yan, Z. The impact of penetration rate of online health service on service quality and price. In Proceedings of the 3rd International Conference on Crowd Science and Engineering—ICCSE’18, Singapore, 28–31 July 2018; pp. 1–5. [Google Scholar] [CrossRef]
- Januszewski, S.I.; Jens, K.; Winter, J.K. Product market competition, corporate governance and firm performance: An empirical analysis for Germany. Res. Econ. 2002, 56, 299–332. [Google Scholar] [CrossRef] [Green Version]
- Pauly, M.V.; Satterthwaite, M.A. The pricing of primary care physicians’ services: A test of the role of consumer information. Bell J. Econ. 1981, 12, 488–506. [Google Scholar] [CrossRef] [Green Version]
- Johnson, E.J.; Wendy, W.M.; Peter, S.F.; Steven, B.; Gerald, L.L. On the depth and dynamics of online search behavior. Manag. Sci. 2004, 50, 299–308. [Google Scholar] [CrossRef] [Green Version]
- Kwon, W.S.; Sharron, J.L. Reciprocal effects between multichannel retailers’ offline and online brand images. J. Retail. 2009, 85, 376–390. [Google Scholar] [CrossRef]
- Shaked, A.; Sutton, J. Relaxing price competition through product differentiation. Rev. Econ. Stud. 1982, 49, 3–13. [Google Scholar] [CrossRef]
- Dufwenberg, M.; Gneezy, U. Price competition and market concentration: An experimental study. Int. J. Ind. Organ. 2000, 18, 7–22. [Google Scholar] [CrossRef] [Green Version]
- Stavins, J. Price discrimination in the airline market: The effect of market concentration. Rev. Econ. Stat. 2001, 83, 200–202. [Google Scholar] [CrossRef] [Green Version]
- Lambert, S.D.; Loiselle, C.G. Health information seeking behavior. Qual. Health Res. 2017, 17, 1006–1019. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, J.C.; Luo, Z.; Roman, L.A. Fixed effects, random effects and GEE: What are the differences? Stat. Med. 2007, 28, 221–239. [Google Scholar] [CrossRef]
- Fletcher, J.M. Social interactions and smoking: Evidence using multiple student cohorts, instrumental variables, and school fixed effects. Health Econ. 2010, 19, 466–484. [Google Scholar] [CrossRef]
- Wooldridge, J. (Ed.) Introductory Econometrics: A Modern Approach; Nelson Education: Scarborough, ON, Canada, 2015. [Google Scholar]
- Fletcher, J.M.; Ross, S.L. Estimating the effects of friends on health behaviors of adolescents. Health Econ. 2018, 27, 1450–1483. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Variables | Description |
|---|---|
| Dependent variable | |
| Price premium (PP) | Doctor’s service price minus national average service price. |
| Independent variables | |
| Participation ratio (PR) | The percentage of doctors providing online medical consultation services in each clinical department in each hospital. Proxy for resource supply. |
| Concentration ratio (CR) | An index of market structure to measure the concentration of online doctor resources in each clinical department in each province. Proxy for resource concentration. |
| Moderator variable | |
| Social stigma (SS) | Dummy variable to show whether the disease is a stigmatized disease. SS = 1 if it is a stigmatized disease, SS = 0 if it is an ordinary disease. |
| Control variables | |
| Clinic title (ClinicT) | Clinic title is certified by the national agency with uniform standards, four stages (Chief Physician, Deputy Chief Physician, Attending Physician, and Resident). ClinicT = 1 if a doctor is Chief or Deputy Chief Physician, and 0 otherwise. |
| Academic title (AcdT) | The academic title is certified by the educational system, four stages (Professor, Associate Professor, Lecturer, and Assistant). AcdT = 1 if a doctor is a Professor or Associate Professor, and 0 otherwise. |
| Work Experience (Exp) | Character length of work experience. |
| Bulletin length (BL) | Character length of the bulletin. |
| Service items (SerItems) | The number of service functions provided by a doctor. |
| Recommendation (Rec) | The recommendation level displayed on the homepage. |
| Online time (OnlineT) | The number of months since the doctor first joined the online health community. |
| Others | |
| Province | The province (municipality) where a doctor works. |
| Hospital | The hospital to which a doctor belongs. |
| Department | The clinical department to which a doctor belongs. |
| Variables | Min | Max | Mean | Std Err | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. PP | −19 | 976 | 0 | 26.62 | 1 | ||||||||||
| 2. PR | 0.005 | 1 | 0.407 | 0.233 | −0.051 *** | 1 | |||||||||
| 3. CR | 0.111 | 1 | 0.383 | 0.128 | 0.066 *** | 0.056 *** | 1 | ||||||||
| 4. SS | 0 | 1 | 0.115 | 0.319 | 0.074 *** | 0.029 *** | 0.032 *** | 1 | |||||||
| 5. ClinicT | 0 | 1 | 0.467 | 0.499 | 0.238 *** | −0.068 *** | −0.014 *** | 0.025 *** | 1 | ||||||
| 6. AcdT | 0 | 1 | 0.198 | 0.398 | 0.236 *** | −0.073 *** | 0.007 * | 0.004 | 0.508 *** | 1 | |||||
| 7. Exp | 0 | 3914 | 113.4 | 139.7 | 0.304 *** | −0.050 *** | 0.020 *** | −0.001 | 0.490 *** | 0.478 *** | 1 | ||||
| 8. BL | 0 | 14,548 | 21.55 | 74.32 | 0.118 *** | 0 | 0.016 *** | 0.021 *** | 0.108 *** | 0.126 *** | 0.195 *** | 1 | |||
| 9. SerItems | 0 | 9 | 6.559 | 1.119 | 0.339 *** | 0.014 *** | 0.048 *** | 0.067 *** | 0.318 *** | 0.265 *** | 0.384 *** | 0.206 *** | 1 | ||
| 10. Rec | 0 | 5 | 3.72 | 0.295 | 0.517 *** | −0.035 *** | 0.100 *** | 0.048 *** | 0.307 *** | 0.337 *** | 0.398 *** | 0.167 *** | 0.492 *** | 1 | |
| 11. OnlineT | 0 | 136 | 46.13 | 35.82 | 0.212 *** | −0.063 *** | 0.018 *** | 0.003 | 0.382 *** | 0.388 *** | 0.420 *** | 0.177 *** | 0.346 *** | 0.245 *** | 1 |
| Variable | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | Model 7 | Model 8 |
|---|---|---|---|---|---|---|---|---|
| PR | −3.512 *** | −3.756 *** | −7.703 *** | −9.355 *** | −7.703 *** | −7.703 *** | −9.355 *** | −9.355 *** |
| (0.419) | (0.500) | (0.830) | (0.835) | (0.830) | (0.830) | (0.835) | (0.835) | |
| CR | 3.793 *** | 2.649 *** | 1.472 | 1.297 | 1.472 | 1.472 | 1.297 | 1.297 |
| (0.715) | (0.809) | ( 1.295) | (1.289) | (1.295) | (1.295) | (1.289) | (1.289) | |
| SS | 4.042 *** | 4.675 *** | 4.780 *** | 4.701 *** | 4.780 *** | 4.780 *** | 4.701 *** | 4.701 *** |
| (0.325) | (0.345) | (0.340) | (0.338) | (0.340) | (0.340) | (0.338) | (0.338) | |
| SS×PR | 8.943 *** | 8.943 *** | 8.943 *** | |||||
| (2.535) | (2.535) | (2.535) | ||||||
| Control variables | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Province fixed effect | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Hospital fixed effect | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Observations | 68,945 | 68,945 | 68,945 | 68,945 | 68,945 | 68,945 | 68,945 | 68,945 |
| Adjusted | 0.290 | 0.385 | 0.384 | 0.384 | 0.384 | 0.384 | 0.324 | 0.384 |
| Weak identification test | 6859.229 | 3898.806 | 6859.229 | 6859.229 | 3898.806 | 3898.806 | ||
| Hansen J-statistics | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | ||
| Endogeneity test | 32.075 | 42.141 | 32.075 | 32.075 | 42.141 | 42.141 | ||
| p-Value | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, C.; Zhang, E.; Han, J. Exploring the Effect of Market Conditions on Price Premiums in the Online Health Community. Int. J. Environ. Res. Public Health 2020, 17, 1326. https://doi.org/10.3390/ijerph17041326
Li C, Zhang E, Han J. Exploring the Effect of Market Conditions on Price Premiums in the Online Health Community. International Journal of Environmental Research and Public Health. 2020; 17(4):1326. https://doi.org/10.3390/ijerph17041326
Chicago/Turabian StyleLi, Chaoran, E. Zhang, and Jingti Han. 2020. "Exploring the Effect of Market Conditions on Price Premiums in the Online Health Community" International Journal of Environmental Research and Public Health 17, no. 4: 1326. https://doi.org/10.3390/ijerph17041326