High Variability in Sepsis Guidelines in UK: Why Does It Matter?

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Sampling Strategy
2.2. Acquisition of Guidelines
2.3. Data Extraction
2.4. Validation Exercise
3. Results
3.1. Use of Published Scoring Systems and Pathways
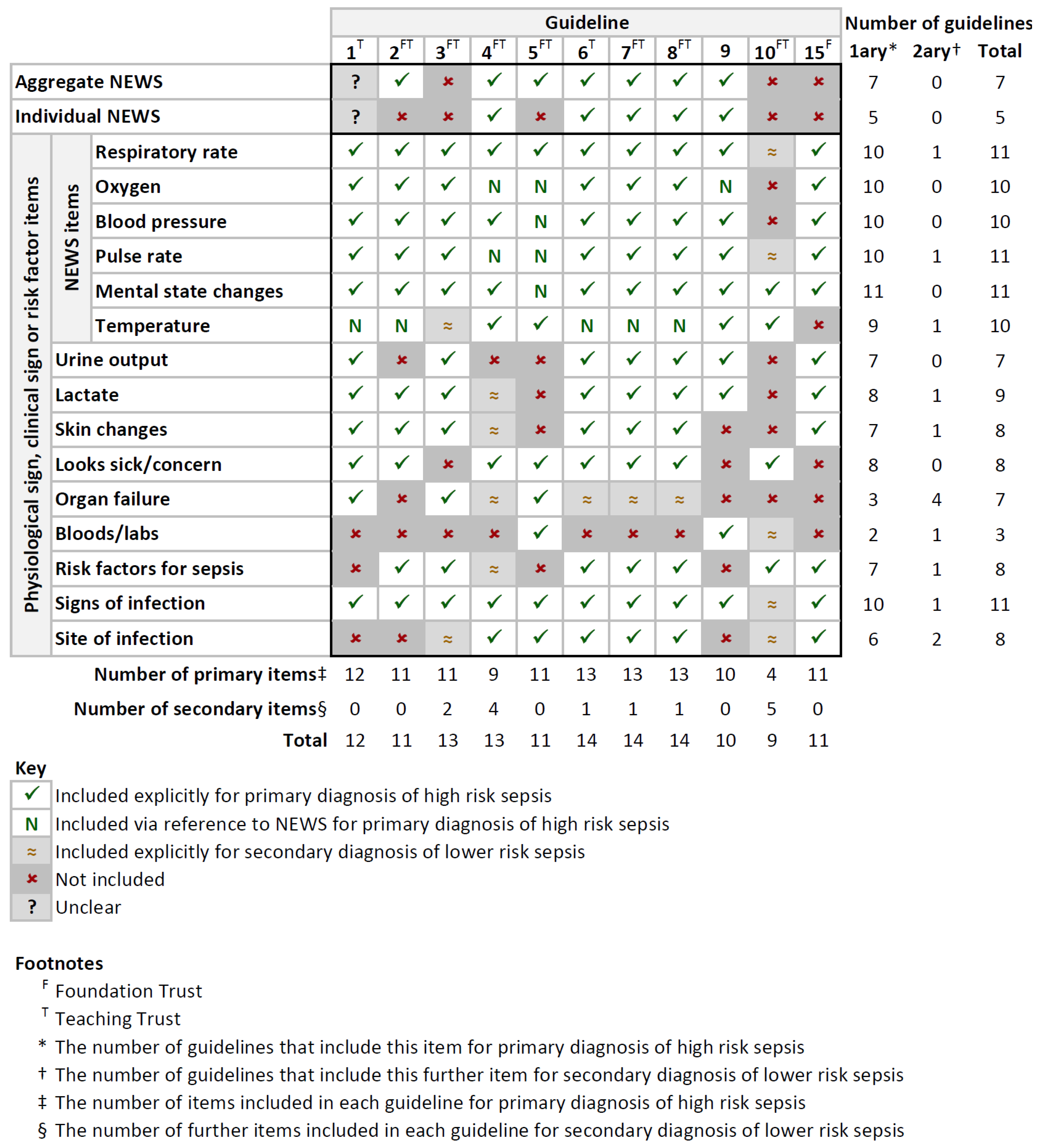
3.2. Physiological Signs and Thresholds
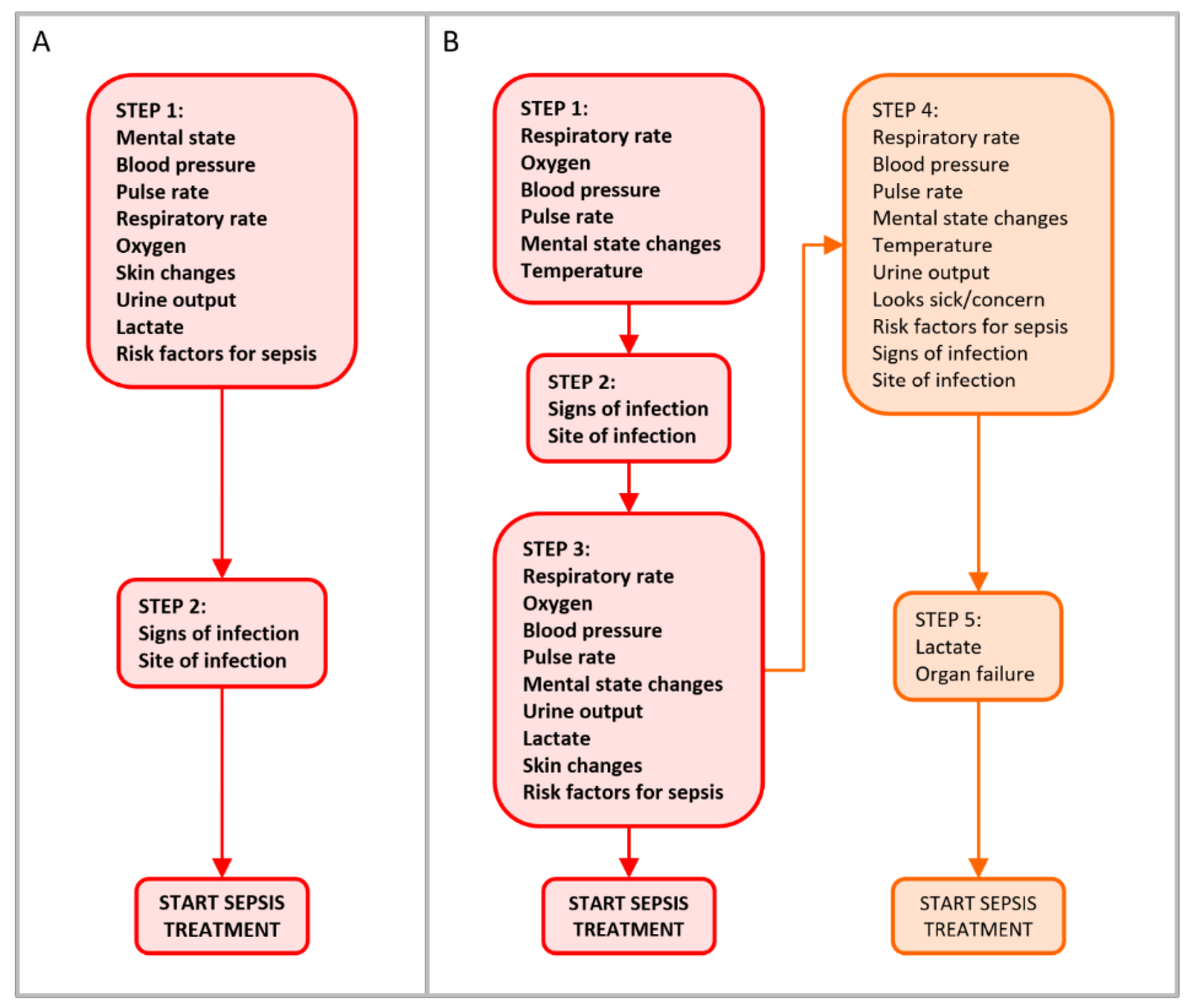
3.3. Pathway Structure
3.4. Validation Exercise
4. Discussion
4.1. Variation in Sepsis Guidelines
4.2. The Potential Impact of Uncertainty in Disease Prevalence on POCT Evaluation and Adoption
4.3. The Potential Impact of Variable Care Pathways in POCT Evaluation and Adoption
4.4. Strength and Weaknesses of the Methodology
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| RESPIRATORY RATE | Respiration rate (part of NEWS) Shortness of breath/abnormal breath sounds/breathing hard |
| OXYGEN | Peripheral capillary oxygen saturation (SpO2) (part of NEWS) |
| Air or oxygen? (part of NEWS) | |
| New need for oxygen to maintain saturation | |
| Oxygen flow rate/concentration (when on O2) | |
| Oxygen saturation (SaO2) | |
| BLOOD PRESSURE | Systolic blood pressure (part of NEWS) |
| Mean arterial pressure | |
| Hypotension | |
| PULSE RATE | Pulse/heart rate (part of NEWS) |
| MENTAL STATE CHANGES | Level of consciousness or new confusion (part of NEWS) |
| New altered mental state | |
| Altered mental state/functional decline | |
| Confusion | |
| New onset confusion | |
| TEMPERATURE | Temperature (part of NEWS) |
| Fever/hypothermia/chills | |
| Rigors | |
| URINE OUTPUT | Urine output |
| LACTATE | Lactate |
| SKIN CHANGES | Mottled/ashen/cyanosis of skin/lips/tongue |
| Non-blanching rash | |
| Purpuric rash | |
| LOOKS SICK/CONCERN | Looks sick |
| Acute unwellness/deterioration | |
| Clinical concern | |
| Relatives concerned | |
| Unwell (fever/chills/confusion) | |
| Non-specific deterioration | |
| ORGAN FAILURE | Acute kidney injury |
| Potentially life-threatening organ dysfunction | |
| Respiratory failure | |
| Circulatory failure | |
| Central nervous system depression | |
| Kidney/gut/liver failure | |
| Other evidence of organ failure | |
| BLOODS/LABS | Altered white blood cell/c-reactive protein count |
| Glucose | |
| White cell count | |
| Lab evidence of organ dysfunction | |
| Positive microbiology | |
| White blood cells in cerebral spinal fluid | |
| Blood sugar | |
| RISK FACTORS FOR SEPSIS | Immunosuppression Recent trauma/surgery Pregnancy/recent delivery Intravenous drug misuse Recent chemotherapy Recent bone marrow/stem cell transplant Neutropaenia/neutrophil count Lines |
| SIGNS OF INFECTION | Possible/suspected/known infection Myalgia Severe malaise New arrhythmia/dysrhythmia Vomiting/diarrhoea Abdominal pain/distention Purulent sputum Chest X-ray changes Abscess Fluid collections |
| SITE OF INFECTION | Sign of infection at wound or surgery site Indwelling catheter Pneumonia/respiratory tract infection Intraperitoneal infection Bone/joint infection Endocarditis Foreign body/implant infection Skin/soft tissue infection Urinary tract infection Biliary tract infection Ear-nose-throat/maxillofacial infection Central nervous system infection Intravascular catheter infection Female reproductive system infection Infection of unknown/other source Pain passing/foul-smelling urine Redness/rash/swelling/cellulitis Meningism Cellulitis/septic arthritis/infected wound/fasciitis Device-related infection Meningitis Abdominal/bowel perforation Peritonitis Endocarditis Catheter infection |
Appendix B
Instructions
- Print the guidelines pack.
- Keep a record of the amount of time spent extracting data from each guideline.
- Read through each document, including all prose, lists, tables, and flow diagrams.
- Complete the Aggregate NEWS and Individual NEWS rows in the data entry table with a tick or cross to indicate whether aggregate and individual NEWS scores are included inform the decision to administer antibiotics for suspected sepsis.
- For each step, determine which sign/symptom/risk factor items are included in that step, and place the step number against those items in the data entry table. Don’t include items that don’t inform the decision to administer antibiotics for suspected sepsis
- Indicate your interpretation of the step numbers on the printed guideline.
- If the item is included only via reference to NEWS, and not explicitly, include “N” after the step number in the data entry table.
- Items separated by “or” or “and/or” should be considered as the same step, those separated by “and” should be considered as separate steps.
- If the current step represents an alternative, lower-risk pathway, and sepsis could have been diagnosed by an earlier step, place the step number in brackets in the data entry table.
- Items may appear in more than one step, hence multiple columns are provided for each item.
- Items may even appear in the same step more than once, both via reference to NEWS and explicitly. In that case, add both the step number, and the step number with “N” (see overleaf for an example).
- Refer to the groupings table to determine which group each item falls into. Every item from the guidelines should be covered in the groupings table.
- Data extraction should stop when sepsis has been diagnosed, indicated by the instruction that antibiotics should be given. The pathway may branch into higher and lower-risk pathways before that point, and all pathways should be documented (see step 9 above).
- Record any comments for each Trust in the final row.
- If discrepancies exist that prevent step numbers from being determined, indicate the items that are present with a tick rather than step numbers. If discrepancies exist that prevent included items being determined, the guideline should be excluded.
Example
- Aggregate NEWS score is included in the pathway, but individual NEWS scores are not.
- Respiratory rate, oxygen, blood pressure, and pulse rate are mentioned explicitly in step 1.
- These items are also included in step 1 via reference to (aggregate) NEWS.
- Mental state changes and temperature are not mentioned explicitly but are included via reference to (aggregate) NEWS in step 1.
- Signs of infection is included in step 2.
- Mental state changes, respiratory rate, and blood pressure are included in step 3, after which antibiotics may be administered.
- Step 4, which represents a lower-risk pathway, includes urine output and lactate, after which antibiotics may be administered.
- The remaining items (skin changes, looks sick/concern, organ failure, bloods/labs, risk factors for sepsis, and site of infection) are not included in the guideline up to the point(s) of antibiotic administration.
| INCLUSION TABLE | X. Trust Name | |||||
|---|---|---|---|---|---|---|
| Aggregate NEWS | ✓ | |||||
| Individual NEWS | ✕ | |||||
| Respiratory rate | 1 | 1N | 3 | |||
| Oxygen | 1 | 1N | ||||
| Blood pressure | 1 | 1N | 3 | |||
| Pulse rate | 1 | 1N | ||||
| Mental state changes | 1N | 3 | ||||
| Temperature | 1N | |||||
| Urine output | (4) | |||||
| Lactate | (4) | |||||
| Skin changes | ||||||
| Looks sick/concern | ||||||
| Organ failure | ||||||
| Bloods/labs | ||||||
| Risk factors for sepsis | ||||||
| Signs of infection | 2 | |||||
| Site of infection | ||||||
Appendix C
| INCLUSION TABLES | Trust 1 | Trust 2 | Trust 3 | Trust 4 | Trust 5 |
|---|---|---|---|---|---|
| Aggregate NEWS | |||||
| Individual NEWS | |||||
| Respiratory rate | |||||
| Oxygen | |||||
| Blood pressure | |||||
| Pulse rate | |||||
| Mental state changes | |||||
| Temperature | |||||
| Urine output | |||||
| Lactate | |||||
| Skin changes | |||||
| Looks sick/concern | |||||
| Organ failure | |||||
| Bloods/labs | |||||
| Risk factors for sepsis | |||||
| Signs of infection | |||||
| Pain score | |||||
| Site of infection | |||||
| Comments |
Appendix D
| INCLUSION TABLES | 1 | 2 | 3 | 4 | 5 | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aggregate NEWS | ? | ✓ | ✕ | ✓ | ✓ | |||||||||||||||
| Individual NEWS | ? | ✕ | ✕ | ✓ | ✕ | |||||||||||||||
| Respiratory rate | 1N | 3 | 1 | 1N | 2 | (3) | 2N | 4 | 1 | 2N | ||||||||||
| Oxygen | 1N | 3 | 1 | 1N | 2 | (3) | 2N | 2N | ||||||||||||
| Blood pressure | 1N | 3 | 1 | 1N | 2 | (3) | 2N | 4 | 2N | |||||||||||
| Pulse rate | 1N | 3 | 1 | 1N | 2 | (3) | 2N | 2N | ||||||||||||
| Mental state changes | 1N | 3 | 1 | 1N | 2 | (3) | 2N | 4 | 2N | |||||||||||
| Temperature | 1N | 1N | (3) | 2N | 3 | 1 | 2N | |||||||||||||
| Urine output | 3 | 2 | ||||||||||||||||||
| Lactate | 3 | 1 | 2 | (5) | ||||||||||||||||
| Skin changes | 3 | 1 | 2 | (5) | ||||||||||||||||
| Looks sick/concern | 1 | 1 | 2 | 2 | ||||||||||||||||
| Organ failure | 3 | 2 | (5) | 2 | ||||||||||||||||
| Bloods/labs | 1 | |||||||||||||||||||
| Risk factors for sepsis | 1 | 2 | (3) | (5) | ||||||||||||||||
| Signs of infection | 2 | 2 | 1 | (3) | 1 | 3 | 1 | |||||||||||||
| Site of infection | (3) | 3 | 1 | |||||||||||||||||
| F | Foundation Trust |
| T | Teaching Trust |
| ✓ | Aggregate/individual NEWS score included |
| ✕ | Aggregate/individual NEWS score not included |
| ? | Unclear whether aggregate/individual NEWS score included |
| e.g., | 1 | Item included explicitly for primary diagnosis of high-risk sepsis in step 1 |
| e.g., | 2N | Item included via reference to NEWS for primary diagnosis of high-risk sepsis in step 2 |
| e.g., | (3) | Item included explicitly for secondary diagnosis of lower-risk sepsis in step 3 |
| Item not included |
| INCLUSION TABLE | 6 | 7 | 8 | 9 | 10 | 15 | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aggregate NEWS | ✓ | ✓ | ✓ | ✓ | ✕ | ✕ | ||||||||||||||||||
| Individual NEWS | ✓ | ✓ | ✓ | ✓ | ✕ | ✕ | ||||||||||||||||||
| Respiratory rate | 1N | 3 | (4) | 1N | 3 | (4) | 1N | 3 | (4) | 1N | 2 | (4) | 1 | |||||||||||
| Oxygen | 1N | 3 | 1N | 3 | 1N | 3 | 1N | 1 | ||||||||||||||||
| Blood pressure | 1N | 3 | (4) | 1N | 3 | (4) | 1N | 3 | (4) | 1N | 4 | 1 | ||||||||||||
| Pulse rate | 1N | 3 | (4) | 1N | 3 | (4) | 1N | 3 | (4) | 1N | 2 | (4) | 1 | |||||||||||
| Mental state changes | 1N | 3 | (4) | 1 | 1N | 3 | (4) | 1N | 3 | (4) | 1N | 2 | 4 | 1 | 1 | |||||||||
| Temperature | 1N | (4) | 1N | (4) | 1N | (4) | 1N | 2 | 1 | (4) | ||||||||||||||
| Urine output | 3 | (4) | 3 | (4) | 3 | (4) | 4 | 1 | ||||||||||||||||
| Lactate | 3 | (5) | 3 | 3 | (5) | 4 | 1 | |||||||||||||||||
| Skin changes | 3 | 3 | 3 | 1 | ||||||||||||||||||||
| Looks sick/concern | 1 | (4) | 1 | (4) | 1 | (4) | 1 | |||||||||||||||||
| Organ failure | (5) | (5) | (5) | |||||||||||||||||||||
| Bloods/labs | 2 | 4 | (4) | |||||||||||||||||||||
| Risk factors for sepsis | 3 | (4) | 3 | (4) | 3 | (4) | 2 | 3 | 1 | |||||||||||||||
| Signs of infection | 2 | (4) | 2 | (4) | 2 | (4) | 3 | (5) | 2 | |||||||||||||||
| Site of infection | 2 | 2 | (4) | 2 | (4) | (5) | 2 | |||||||||||||||||
| F | Foundation Trust |
| T | Teaching Trust |
| ✓ | Aggregate/individual NEWS score included |
| ✕ | Aggregate/individual NEWS score not included |
| ? | Unclear whether aggregate/individual NEWS score included |
| e.g., | 1 | Item included explicitly for primary diagnosis of high-risk sepsis in step 1 |
| e.g., | 2N | Item included via reference to NEWS for primary diagnosis of high-risk sepsis in step 2 |
| e.g., | (3) | Item included explicitly for secondary diagnosis of lower-risk sepsis in step 3 |
| Item not included |
References
- Kinsman, L.; Rotter, T.; James, E.; Snow, P.; Willis, J. What is a clinical pathway? Development of a definition to inform the debate. BMC Med. 2010, 8, 31. [Google Scholar] [CrossRef] [PubMed]
- Monaghan, P.J.; Robinson, S.; Rajdl, D.; Bossuyt, P.M.; Sandberg, S.; St John, A.; O’Kane, M.; Lennartz, L.; Röddiger, R.; Lord, S.J.; et al. Practical guide for identifying unmet clinical needs for biomarkers. EJIFCC 2018, 29, 129–137. [Google Scholar] [PubMed]
- Abel, L.; Shinkins, B.; Smith, A.; Sutton, A.J.; Sagoo, G.S.; Uchegbu, I.; Allen, A.J.; Graziadio, S.; Moloney, E.; Yang, Y.; et al. Early Economic Evaluation of Diagnostic Technologies: Experiences of the NIHR Diagnostic Evidence Co-operatives. Med. Decis. Mak. Int. J. Soc. Med. Decis. Mak. 2019, 39, 857–866. [Google Scholar] [CrossRef] [PubMed]
- Access. NOfM. Available online: https://www.nice.org.uk/about/what-we-do/life-sciences/office-for-market-access (accessed on 13 January 2020).
- Gül, F.; Arslantaş, M.K.; Cinel, İ.; Kumar, A. Changing Definitions of Sepsis. Turk. J. Anaesthesiol. Reanim. 2017, 45, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- NCEPOD. Just Say Sepsis. 2015. Available online: https://www.ncepod.org.uk/2015sepsis.html (accessed on 16 March 2020).
- Kumar, A.; Roberts, D.; Wood, K.E.; Light, B.; Parrillo, J.E.; Sharma, S.; Suppes, R.; Feinstein, D.; Zanotti, S.; Taiberg, L.; et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit. Care Med. 2006, 34, 1589–1596. [Google Scholar] [CrossRef]
- Ferrer, R.; Martin-Loeches, I.; Phillips, G.; Osborn, T.M.; Townsend, S.; Dellinger, R.P.; Artigas, A.; Schorr, C.; Levy, M.M. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: Results from a guideline-based performance improvement program. Crit. Care Med. 2014, 42, 1749–1755. [Google Scholar] [CrossRef]
- The Cost of Sepsis Care in the UK: Final Report. Available online: http://allcatsrgrey.org.uk/wp/download/health_economics/YHEC-Sepsis-Report-17.02.17-FINAL.pdf (accessed on 31 January 2018).
- NICE. Sepsis: Recognition, Diagnosis and Early Management. Available online: https://www.nice.org.uk/guidance/ng51 (accessed on 16 March 2020).
- RCP. National Early Warning Score (NEWS). Available online: https://www.rcplondon.ac.uk/file/9559 (accessed on 16 March 2020).
- RCP. National Early Warning Score (NEWS) 2. Available online: https://www.rcplondon.ac.uk/projects/outputs/national-early-warning-score-news-2 (accessed on 16 March 2020).
- UK Sepsis Trust. Red Flag Sepsis. Available online: https://sepsistrust.org/wp-content/uploads/2018/06/ED-adult-NICE-Final-1107.pdf (accessed on 16 March 2020).
- RCEM. Severe Sepsis and Septic Shock Clinical Audit 2016/17 National Report. Available online: https://www.rcem.ac.uk/docs/QI%20+%20Clinical%20Audit/RCEM%20Severe%20Sepsis%20and%20Septic%20Shock%20National%20Audit%20Report.pdf?dm_i=21A8,4Z05S,FLXFHF,IX1KI,12017 (accessed on 16 March 2020).
- NHS England. NHS Organisations in England, Quarter 4, 2017–2018. 2018. Available online: https://www.england.nhs.uk/statistics/statistical-work-areas/bed-availability-and-occupancy/bed-data-overnight/ (accessed on 16 March 2020).
- GOV. How to Make a Freedom of Information (FOI) Request. 2018. Available online: https://www.gov.uk/make-a-freedom-of-information-request (accessed on 16 March 2020).
- Burns, S.M.; Earven, S.; Fisher, C.; Lewis, R.; Merrell, P.; Schubart, J.R.; Truwit, J.D.; Bleck, T.P. Implementation of an institutional program to improve clinical and financial outcomes of mechanically ventilated patients: One-year outcomes and lessons learned. Crit. Care Med. 2003, 31, 2752–2763. [Google Scholar] [CrossRef]
- Allen, D.; Rixson, L. How has the impact of ‘care pathway technologies’ on service integration in stroke care been measured and what is the strength of the evidence to support their effectiveness in this respect? Int. J. Evid. Based Healthc. 2008, 6, 78–110. [Google Scholar]
- Algaze, C.A.; Shin, A.Y.; Nather, C.; Elgin, K.H.; Ramamoorthy, C.; Kamra, K.; Kipps, A.K.; Yarlagadda, V.V.; Mafla, M.M.; Vashist, T.; et al. Applying Lessons from an Inaugural Clinical Pathway to Establish a Clinical Effectiveness Program. Pediatr. Q. Saf. 2018, 3, e115. [Google Scholar] [CrossRef]
- Malley, M.; Bruce, M.; Devlin, H.; Patel, H.; Narendra, D.; Cox, S.; Chotalia, R. It is time to standardise the length of postnatal antibiotic administration nationally. Arch. Dis. Child. Fetal. Neonatal Ed. 2019, 104, F225. [Google Scholar] [CrossRef] [PubMed]
- Rhee, C.; Kadri, S.S.; Danner, R.L.; Suffredini, A.F.; Massaro, A.F.; Kitch, B.T.; Lee, G.; Klompas, M. Diagnosing sepsis is subjective and highly variable: A survey of intensivists using case vignettes. Crit. Care 2016, 20, 89. [Google Scholar] [CrossRef] [PubMed]
- Rhee, C.; Brown, S.R.; Jones, T.M.; O’Brien, C.; Pande, A.; Hamad, Y.; Bulger, A.L.; Tobin, K.A.; Massaro, A.F.; Anderson, D.J.; et al. Variability in determining sepsis time zero and bundle compliance rates for the centers for medicare and medicaid services SEP-1 measure. Infect. Control Hosp. Epidemiol. 2018, 39, 994–996. [Google Scholar] [CrossRef] [PubMed]
- Ferrante di Ruffano, L.; Hyde, C.J.; McCaffery, K.J.; Bossuyt, P.M.; Deeks, J.J. Assessing the value of diagnostic tests: A framework for designing and evaluating trials. BMJ 2012, 344, e686. [Google Scholar] [CrossRef]
- Bossuyt, P.M.; Irwig, L.; Craig, J.; Glasziou, P. Comparative accuracy: Assessing new tests against existing diagnostic pathways. BMJ 2006, 332, 1089–1092. [Google Scholar] [CrossRef]
- Lijmer, J.G.; Leeflang, M.; Bossuyt, P.M. Proposals for a phased evaluation of medical tests. Med. Decis. Mak. Int. J. Soc. Med. Decis. Mak. 2009, 29, E13–E21. [Google Scholar] [CrossRef]
- Bossuyt, P.M.; Reitsma, J.B.; Linnet, K.; Moons, K.G. Beyond diagnostic accuracy: The clinical utility of diagnostic tests. Clin. Chem. 2012, 58, 1636–1643. [Google Scholar] [CrossRef]
- Leeflang, M.M.; Bossuyt, P.M.; Irwig, L. Diagnostic test accuracy may vary with prevalence: Implications for evidence-based diagnosis. J. Clin. Epidemiol. 2009, 62, 5–12. [Google Scholar] [CrossRef]
- Hajian-Tilaki, K. Sample size estimation in diagnostic test studies of biomedical informatics. J. Biomed. Inform. 2014, 48, 193–204. [Google Scholar] [CrossRef]
- Whitewater Charitable Trust. The Cost of Sepsis Care in the UK Final Report. Consortium. YYHE, editor. Available online: http://allcatsrgrey.org.uk/wp/wpfb-file/yhec-sepsis-report-17-02-17-final-pdf/2017 (accessed on 16 March 2020).
- St John, A.; Price, C.P. Economic Evidence and Point-of-Care Testing. Clin. Biochem. Rev. 2013, 34, 61–74. [Google Scholar]
- Briggs, A.; Sculpher, M.; Claxton, K. Decision Modelling for Health Economic Evaluation, 2nd ed.; Oxford University Press: Oxford, UK, 2006. [Google Scholar]
- Quercioli, C.; Nisticò, F.; Troiano, G.; Maccari, M.; Messina, G.; Barducci, M.; Carriero, G.; Golinelli, D.; Nante, N. Developing a new predictor of health expenditure: Preliminary results from a primary healthcare setting. Public Health 2018, 163, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Woolf, S.H.; Grol, R.; Hutchinson, A.; Eccles, M.; Grimshaw, J. Clinical guidelines: Potential benefits, limitations, and harms of clinical guidelines. BMJ 1999, 318, 527–530. [Google Scholar] [CrossRef] [PubMed]
- Churpek, M.M.; Snyder, A.; Han, X.; Sokol, S.; Pettit, N.; Howell, M.D.; Edelson, D.P. Quick Sepsis-related Organ Failure Assessment, Systemic Inflammatory Response Syndrome, and Early Warning Scores for Detecting Clinical Deterioration in Infected Patients outside the Intensive Care Unit. Am. J. Respir. Crit. Care Med. 2017, 195, 906–911. [Google Scholar] [CrossRef]
- Appleton, J.V.; Cowley, S. Analysing clinical practice guidelines. A method of documentary analysis. J. Adv. Nurs. 1997, 25, 1008–1017. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. Available online: www.handbook.cochrane.org (accessed on 16 March 2020).
- Mathes, T.; Klaßen, P.; Pieper, D. Frequency of data extraction errors and methods to increase data extraction quality: A methodological review. BMC Med. Res. Methodol. 2017, 17, 152. [Google Scholar] [CrossRef] [PubMed]
- Brouwers, M.C.; Kho, M.E.; Browman, G.P.; Burgers, J.S.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Grimshaw, J.; Hanna, S.E.; et al. AGREE II: Advancing guideline development, reporting and evaluation in health care. CMAJ 2010, 182, E839–E842. [Google Scholar] [CrossRef]
- Drennan, V.M.; Norrie, C.; Cole, L.; Donovan, S. Addressing incontinence for people with dementia living at home: A documentary analysis of local English community nursing service continence policies and clinical guidance. J. Clin. Nurs. 2013, 22, 339–346. [Google Scholar] [CrossRef]
- Stiel, S.; Heckel, M.; Christensen, B.; Ostgathe, C.; Klein, C. In-service documentation tools and statements on palliative sedation in Germany—Do they meet the EAPC framework recommendations? A qualitative document analysis. Support. Care Cancer 2016, 24, 459–467. [Google Scholar] [CrossRef]
- Coates, L.C.; Moverley, A.R.; McParland, L.; Brown, S.; Navarro-Coy, N.; O’Dwyer, J.L.; Meads, D.M.; Emery, P.; Conaghan, P.G.; Helliwell, P.S. Effect of tight control of inflammation in early psoriatic arthritis (TICOPA): A UK multicentre, open-label, randomised controlled trial. Lancet 2015, 386, 2489–2498. [Google Scholar] [CrossRef]
- Jacobs, I.J.; Menon, U.; Ryan, A.; Gentry-Maharaj, A.; Burnell, M.; Kalsi, J.K.; Amso, N.N.; Apostolidou, S.; Benjamin, E.; Cruickshank, D.; et al. Ovarian cancer screening and mortality in the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS): A randomised controlled trial. Lancet. 2016, 387, 945–956. [Google Scholar] [CrossRef]
- Atkin, W.; Wooldrage, K.; Parkin, D.M.; Kralj-Hans, I.; MacRae, E.; Shah, U.; Duffy, S.; Cross, A.J. Long term effects of once-only flexible sigmoidoscopy screening after 17 years of follow-up: The UK Flexible Sigmoidoscopy Screening randomised controlled trial. Lancet 2017, 389, 1299–1311. [Google Scholar] [CrossRef]


| # | Region of England | Size | Foundation? | Teaching? | Reason of Exclusion |
|---|---|---|---|---|---|
| 1 | East Midlands | 95–100% | No | Yes | |
| 2 | North-East | 95–100% | Yes | Yes | |
| 3 | South-East | 85–90% | Yes | Yes | |
| 4 | Yorkshire and the Humber | 80–85% | Yes | Yes | |
| 5 | London | 75–80% | Yes | Yes | |
| 6 | London | 70–50% | No | Yes | |
| 7 | North-West | 70–50% | Yes | Yes | |
| 8 | South-West | 65–70% | Yes | Yes | |
| 9 | South-West | 60–65% | No | No | |
| 10 | North-West | 55–60% | Yes | Yes | |
| 11 | North-West | 45–50% | No | Yes | Discrepancies in guideline |
| 12 | North-East | 40–45% | Yes | No | Response did not include a sepsis guideline |
| 13 | West Midlands | 40–45% | No | No | Response did not include a sepsis guideline |
| 14 | East of England | 35–40% | Yes | Yes | Response did not include a sepsis guideline for a general adult population |
| 15 | Yorkshire and the Humber | 25–30% | Yes | No |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bray, A.; Kampouraki, E.; Winter, A.; Jesuthasan, A.; Messer, B.; Graziadio, S. High Variability in Sepsis Guidelines in UK: Why Does It Matter? Int. J. Environ. Res. Public Health 2020, 17, 2026. https://doi.org/10.3390/ijerph17062026
Bray A, Kampouraki E, Winter A, Jesuthasan A, Messer B, Graziadio S. High Variability in Sepsis Guidelines in UK: Why Does It Matter? International Journal of Environmental Research and Public Health. 2020; 17(6):2026. https://doi.org/10.3390/ijerph17062026
Chicago/Turabian StyleBray, Alison, Emmanouela Kampouraki, Amanda Winter, Aaron Jesuthasan, Ben Messer, and Sara Graziadio. 2020. "High Variability in Sepsis Guidelines in UK: Why Does It Matter?" International Journal of Environmental Research and Public Health 17, no. 6: 2026. https://doi.org/10.3390/ijerph17062026
APA StyleBray, A., Kampouraki, E., Winter, A., Jesuthasan, A., Messer, B., & Graziadio, S. (2020). High Variability in Sepsis Guidelines in UK: Why Does It Matter? International Journal of Environmental Research and Public Health, 17(6), 2026. https://doi.org/10.3390/ijerph17062026